 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 50, No. 2, April-June, 2004, pp. 89-93 Original Article Imaging using Tc99m-tetrofosmin for the detection of the recurrence of brain tumour: A comparative study with Tc99m-glucoheptonate Barai Sukanta , Bandopadhayaya GP, Julka PK, Malhotra A, Bal CS, Dhanpathi H Departments of Nuclear Medicine, All India Institute of Medical Sciences, New Delhi Code Number: jp04029 ABSTRACT BACKGROUND: In the past "blood-brain barrier" agents such as Tc99m-glucoheptonate were routinely used for the diagnosis of brain tumours. Of late, agents used for studying myocardial perfusion namely, Tc99m-tetrofosmin, Thallium-201, and Tc99m-sestamibi have replaced the "blood-brain barrier agents" when imaging is undertaken for the detection of the recurrence of brain tumours. However, the incremental diagnostic information provided by Tc99m-tetrofosmin when compared with a blood brain barrier agent in the diagnosis of recurrent brain tumour has not been evaluated till date. AIMS: The study was carried out to substantiate whether Tc99m-tetrofosmin provides any incremental diagnostic information not provided by the blood brain barrier agent Tc99m-glucoheptonate. MATERIAL AND METHODS: Brain SPECT scans were performed using Tc99m-tetrofosmin and Tc99m-glucoheptonate in 126 patients of recurrent brain tumour. Bio-distribution and uptake properties of both the tracers were analysed by measuring relative uptake of both the tracers in tumour compared to background (T/B ratio), nasopharynx (T/N ratio) and scalp (T/S ratio). STATISTICAL ANALYSIS: Descriptive statistics were calculated for each variable. Pearson's correlation coefficient was applied to see agreement of the continuous variables. Paired t test was used to evaluate the difference between two means. RESULTS: Uptake properties of both the tracers were analysed in 105 patients in whom both Tc99m-tetrofosmin and Tc99m-glucoheptonate showed concentration. The remaining 21 patients in whom the tumour mass did not show Tc99m-tetrofosmin concentration were excluded from the study. Mean T/B ratio, T/N ratio and T/S ratio was 5.83 ± 2.09 and 5.99 ± 2.26, 0.53 ± 0.21 and 0.55 ± 0.22 and 1.11 ± 0.60 and 1.26 ± 0.52 for Tc99m-tetrofosmin and Tc99m-glucoheptonate respectively. No statistically significant difference between T/B ratio and T/N ratio of Tc99m-tetrofosmin and Tc99m-glucoheptonate was found; p values were 0.25 and 0.83 respectively. However there was significant difference (P=0.006) between the T/S ratio of Tc99m-tetrofosmin and that of Tc99m-glucoheptonate. CONCLUSION: Tc99m-tetrofosmin does not provide any incremental diagnostic information not provided by the blood brain barrier agent Tc99m-glucoheptonate. Keywords: Tetrofosmin, glucoheptonate, brain tumour, fan beam collimator Functional imaging of the brain in the form of single photon emission computed tomography (SPECT) is frequently performed to evaluate the viability of a mass lesion detected by anatomical imaging modalities.[1],[2],[3] Various radiopharmaceuticals have been evaluated as brain tumour-seeking tracers. Before the introduction of thallium-201 and thallium analogues like Tc99m-tetrofosmin, radiopharmaceuticals like unlabelled technetium pertechnetate, Tc99m-glucoheptonate, and Tc99m-diethylene triamine penta acetic acid (Tc99m-DTPA) were used. These tracers concentrate in the tumour primarily due to the increased permeability of the blood-brain barrier. These agents are, therefore, referred to as "blood-brain barrier" agents.[4],[5],[6] Presently, oncophilic substances like thallium-201, Tc99m-sestamibi and Tc99m-tetrofosmin have replaced blood-brain barrier imaging agents for the diagnosis of recurrent brain tumour. Initially introduced as an agent for studying myocardial perfusion, Technetium-99m labelled tetrofosmin (Tc99m-tetrofosmin) has been successfully applied in the imaging of recurrent brain tumour also.[7] However, no study has evaluated if Tc99m-tetrofosmin provides any incremental diagnostic information as compared with a blood-brain barrier agent like Tc99m-glucoheptonate in the diagnosis of recurrent brain tumour. This study was designed to evaluate whether Tc99m-tetrofosmin provides any incremental diagnostic information when compared with Tc99m-glucoheptonate. MATERIAL AND METHODS Brain SPECT with Tc99m--tetrofosmin and Tc99m-glucoheptonate was performed in 126 patients of brain tumour with recurrence of disease suspected clinically and confirmed by contrast enhanced magnetic resonance imaging. All eligible patients were sequentially enrolled and followed through the cancer clinic and imaged between 1998 and 2002. There were 43 females and 83 male patients in the group with an age range of 5-67 years. The histological type was ependymoma in 8 patients, meningioma in 15 patients, glioblastoma multiforme in 42 patients, anaplastic astrocytoma in 30 patients and low-grade gliomas in 31 patients. All of them had prior tumour debulking surgery followed by external beam radiotherapy (Range: 54-64 Gray). Multiple cycles of cytotoxic chemotherapy were given to 94 patients. Patients who had undergone any therapeutic intervention in the preceding 6 months were excluded from the study. The Institution′s ethics committee approved the study and patients were enrolled in the study after obtaining an informed consent from the subject or his/ her legal guardians. Brain SPECT with both Tc99m-tetrofosmin and Tc99m-glucoheptonate was performed in all 126 patients on separate days with a gap of 72-96 hours. Brain SPECT was acquired one-hour post intravenous administration of 370-740 MBq (10-20mCi) of Tc99m-tetrofosmin or Tc99m-glucoheptonate using a dual head single photon emission computed tomography system (Varicam, Elscint, Haifa, Israel) equipped with fan beam collimator. The dose was calculated as body surface area divided by 1.73 and then multiplied by the adult dose of 740 MBq. Energy setting was 140 KeV with 20% energy window. In total 90 views were obtained with one view at every 4° for 25 seconds per view in a 128 x 128 matrix. Acquisition time was approximately 20 minutes. Projection data was pre-filtered before back projection and reconstruction was performed with a two-dimensional Metz filter (cut off=0.43 cm, P=30, Value of max=124, position of max=23, FWHM=100). Attenuation correction was performed by Chang′s method.[8] No scatter correction was done. Reconstructed images were displayed and analysed using transverse, sagittal and coronal views with a slice thickness of approximately 7 mm. Data Analysis: Two experienced nuclear medicine physicians evaluated the scan findings independently. Abnormally increased radiotracer uptake more than or equal to scalp tracer concentration in the primary tumour bed was considered indicative of viable tumour. The intensity of the tracer concentration in the tumour mass was expressed as tumour to background ratio (T/B ratio). In addition, tumour to nasopharynx (T/N ratio), and tumour to scalp ratio (T/S ratio) were calculated in both sets of studies. For tumour to background (T/B ratio) ratio estimation an irregular
region of interest (ROI) was drawn encircling the tumour on the transverse
SPECT
slice with greatest tumour activity and the average pixel count within
the ROI was obtained. To obtain the background activity an exactly similar
ROI was generated by computer software on the corresponding site of the
opposite lobe and an average pixel count obtained. The ratio of the two
average pixel counts was the T/B ratio. For tumour to nasopharynx (T/N
ratio) ratio estimation, a ROI was drawn around the nasopharynx in the
midline sagittal slice showing the highest nasopharyngeal uptake and
the average pixel count was obtained. The ratio of the average pixel
count of tumour ROI to nasopharyngeal ROI was designated as the T/N ratio.
For tumour to scalp (T/S ratio) ratio estimation, a ROI was drawn around
the scalp excluding the tumour margins on the transverse slice from which
the tumour to background ratio was obtained and the average pixel count
was obtained. The ratio of the average pixel count of tumour ROI to scalp
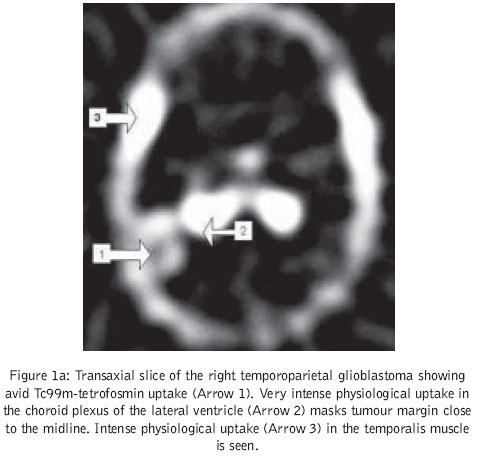
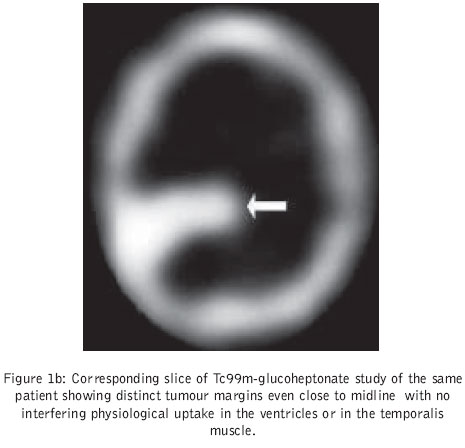
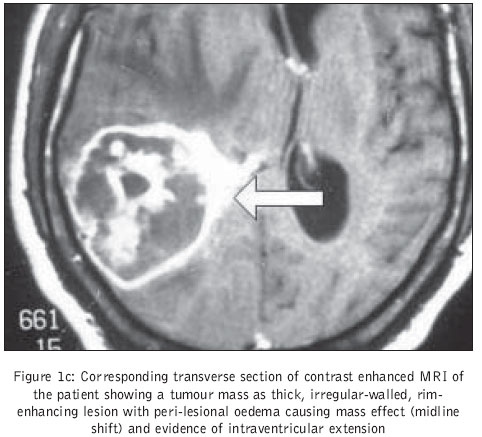
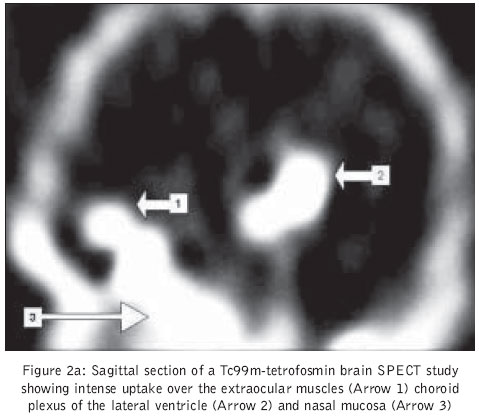
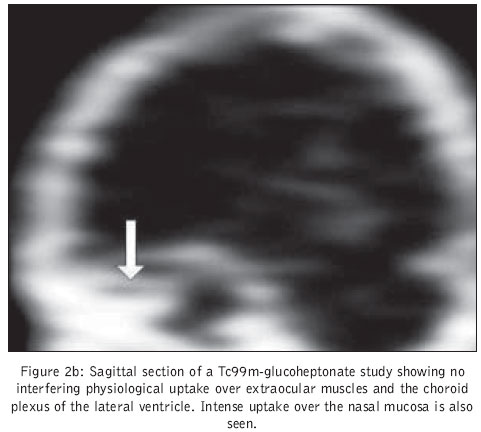
ROI was designated as the T/S ratio. Results Discussion For the proper evaluation of a tumour, the tracer should not only have the ability to localise in the tumour in a quantity sufficient to allow imaging but should also have an ideal intra- and pericardial misdistribution. Misdistribution of Tc99m-tetrofosmin was not very suitable for brain tumour evaluation. Tetrofosmin shows intense physiological uptake in the choroid plexus of the ventricles, temporalis muscles, and extra-ocular muscles, which significantly interfered with tumour evaluation [Figure:1a], [Figure:1b] and [Figure:1c]. Tc99m-glucoheptonate did not reveal any of these confounding physiological uptakes. Therefore, misdistribution of Tc99m-glucoheptonate was more favourable for brain tumour evaluation [Figure:2a] and [Figure:2b]. Tumour to background ratio, which reflects the intensity of tracer uptake in the tumour, and how distinctly the lesion was seen from the surrounding healthy brain parenchyma, was 5.83 ± 2.09 and 5.99 ± 2.26 for Tc99m-tetrofosmin and Tc99m-glucoheptonate respectively. There was no significant difference between the two ratios (P value 0.83) and both the agents allowed equally good visualisation of tumour mass. Tumour to nasopharynx ratio, which reflects how distinctly lesions close to the nasal mucosa can be visualised, was 0.53 ± 0.21 and 0.55 ± 0.22 for Tc99m-tetrofosmin and Tc99m-glucoheptonate respectively. There was no significant difference between the two ratios, signifying that neither of the tracers offer any advantage in evaluating a tumour mass close to the nasal mucosa, as may be in the case of a tumour located in the basifrontal region. Tumour to scalp ratio, which reflects how distinctly lesions close to scalp can be visualised, was 1.11 ± 0.60 and 1.26 ± 0.52 for Tc99m-tetrofosmin and Tc99m-glucoheptonate respectively. There was a significant difference between the two ratios (P value, 0.006) signifying that tumour margins close to the skull are better visualised in Tc99m-glucoheptonate images. This finding is explainable from the fact that the temporalis muscles, which are attached to both the temporal bones, show intense Tc99m-tetrofosmin uptake resulting in a higher scalp uptake when compared with Tc99m-glucoheptonate. Thallium-201 and Tc99m-sestamibi are commonly used for imaging brain tumours. Nagamachi et al have reported a sensitivity of 90.3% and a specificity of 77.4% for Tc99m-MIBI, which was comparable to that of Tl-201 (90.3% and 80.6%, respectively).[9] No investigator has reported the sensitivity and specificity of Tc99m-tetrofosmin as brain tumour imaging agent to date. However, Barai et al have reported poor sensitivity of Tc99m-tetrofosmin for the detection of posterior fossa tumours.[10] Pentavalent Dimercapto succinic acid (DMSA-V) is also used for brain tumour imaging. Hirano et al have reported a sensitivity of approximately 93% and 88% for DMSA and thallium respectively.[11] 3-[(123)I]Iodo-alpha-methyl-L-tyrosine (IMT) is an artificial amino acid which exhibits high uptake in brain tumours, though it is not incorporated into cellular proteins. Henze et al in their comparative study between MIBI and IMT reported a sensitivity of 94% and specificity of 100% for IMT and 53% and 75% for MIBI in differentiating progressive tumours from post-radiation gliosis.[18] Positron emission tomography (PET) using various radiotracers is widely utilized for evaluating residual or recurrent tumours following therapy, and can be used to survey patients with low-grade brain tumours for evidence of degeneration into high-grade malignancy.[19] In the case of suspected tumour recurrence or progression, PET can aid in defining appropriate targets for biopsy. FDG-PET is however less sensitive than contrast-enhanced MRI for detecting intracranial metastases. Chao et al evaluated 43 patients with brain tumour by FDG-PET. For all tumour types, the sensitivity of FDG PET for diagnosing tumour was 75% and the specificity was 81%. For brain metastasis without MRI co-registration, FDG PET had a sensitivity of 65% and a specificity of 80%. For brain metastasis with MRI co-registration, FDG PET had a sensitivity of 86% and specificity of 80%.[20] Other tracers, such as 11C-methionine and [(18) F] fluorocholine (fluoromethyl-dimethyl-2-hydroxyethylammonium [FCH], also avidly accumulate in brain tumours and have the advantage of low background cortical activity.[21] The relationship between the degree of uptake of these agents and tumour grade is not established. One limitation of FDG-PET is the occasional inability to distinguish radiation necrosis from recurrent high-grade tumour. Necrotic mass intensely infiltrated with inflammatory cells sometimes also reveals increased glucose metabolism.[22] Amino-acid tracers, such as C11-methionine, are better for this purpose and thus play a complementary role to FDG. L-methionine uptake is known to correlate better than FDG with tumour proliferative activity.[23] Given the poor prognosis of patients with primary brain tumour, particularly with high-grade lesions, the overall clinical utility of single photon emission computed tomography (SPECT) and PET in characterising recurrent lesions remains dependent on the availability of effective treatments. Tc99m-tetrofosmin brain SPECT provided false negative results in 21(16.6%) patients in our study. Tc99m-tetrofosmin does not show any concentration in tumours expressing p-glycoprotein, a product of multidrug resistance gene.[24],[25] p-glycoprotein expression study was not performed in these 21 patients but it is possible that these tumours were expressing p-glycoprotein. Imaging brain tumours expressing p-glycoprotein is a great challenge since they do not concentrate the commonly used tracers like Tc99m-sestamibi and Tc99m-tetrofosmin.[26],[27] Tc99m-glucoheptonate accumulation does not appear to be influenced by the expression of p-glycoprotein. The tumours that did not show any Tc99m-tetrofosmin concentration showed avid Tc99m-glucoheptonate concentration. The lack of histopathological verification of diagnosis in those 21 patients with no tetrofosmin uptake along with the lack of information regarding the p-glycoprotein expression in them are the principal limitations of this study. Conclusion Tc99m-tetrofosmin does not provide any incremental diagnostic information not provided by the blood brain barrier agent Tc99m-glucoheptonate. References
Copyright 2004 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp04029t1.jpg] [jp04029f2b.jpg] [jp04029f1c.jpg] [jp04029f1a.jpg] [jp04029f1b.jpg] [jp04029f2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}