
|
Journal of Postgraduate Medicine
Medknow Publications and Staff Society of Seth GS Medical College and KEM Hospital, Mumbai, India
ISSN: 0022-3859 EISSN: 0972-2823
Vol. 50, Num. 2, 2004, pp. 110-112
|
Journal of Postgraduate Medicine, Vol. 50, No. 2, April-June, 2004, pp. 110-112
Case Report
Cerebellar medulloblastoma presenting with skeletal metastasis
Barai Sukanta , Bandopadhayaya GP, Julka PK, Dhanapathi H, Haloi AK, Seith A
Departments of Nuclear Medicine, Radiotherapy and Radiology,All India Institute of Medical Sciences, New Delhi, India
Correspondence Address:Departments of Nuclear Medicine, All India Institute of Medical Sciences, New Delhi
danzig@rediffmail.com
Code Number: jp04034
Abstract
Medulloblastomas are highly malignant brain tumours, but only rarely produce skeletal metastases. No case of medulloblastoma has been documented to have produced skeletal metastases prior to craniotomy or shunt surgery. A 21-year-old male presented with pain in the hip and lower back with difficulty in walking of 3 months' duration. Signs of cerebellar dysfunction were present hence a diagnosis of cerebellar neoplasm or skeletal tuberculosis with cerebellar abscess formation was considered. MRI of brain revealed a lesion in the cerebellum suggestive of medulloblastoma. Bone scan revealed multiple sites of skeletal metastases excluding the lumbar vertebrae. MRI of lumbar spine and hip revealed metastases to all lumbar vertebrae and both hips. Computed tomography-guided biopsy was obtained from the L3 vertebra, which revealed metastatic deposits from medulloblastoma. Cerebrospinal fluid cytology showed the presence of medulloblastoma cells. A final diagnosis of cerebellar medulloblastoma with skeletal metastases was made. He underwent craniotomy and histopathology confirmed medulloblastoma.
Keywords: Medulloblastoma, skeletal metastases, bone scan
Primary tumours of the central nervous system of both neuronal and glial origin are known to give rise to neuraxial and less frequently extra-neuraxial metastases. Skeletal metastases from brain tumours are rare, but when they occur, they almost always follow surgery for the primary tumour or after various shunting procedures for symptomatic relief of raised intracranial pressure.[1] Medulloblastomas are highly malignant tumours of primitive neuroectodermal (PNET) origin, representing more than 20% of all childhood brain tumours and have the highest incidence of bone marrow metastasis among central nervous system malignancies.[2] About 94 cases of medulloblastoma with skeletal metastases have been described in the English literature but none from the Indian population. In all the reported cases skeletal metastasis developed after the resection of the primary tumour and mostly after a cerebrospinal fluid shunt was placed. We report a case of a 21-year-old male who presented with skeletal metastases producing bony pain at multiple sites from a cerebellar medulloblastoma.
Case History
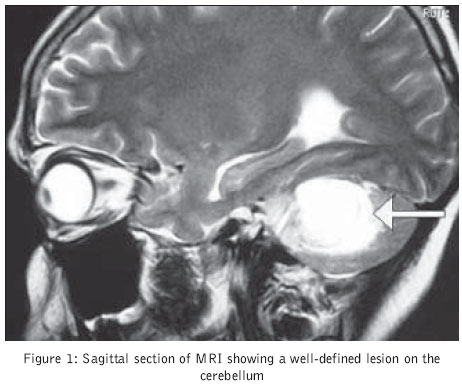
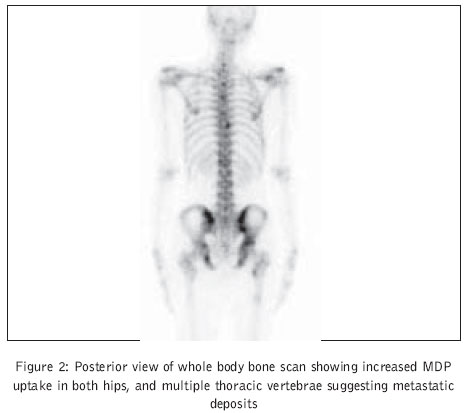
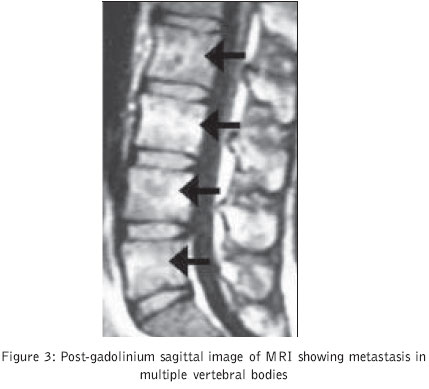
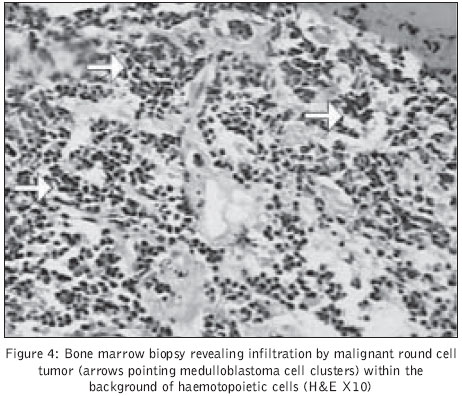
A 21-year-old young man presented with pain in the hip and lower back and difficulty in walking of 3 months′ duration. On examination several other sites of tenderness over the spine were found. Leg raising test was negative. But cerebellar signs were present in the form of ataxia and incoordination. Ophthalmological examination revealed bilateral papilloedema. A clinical diagnosis of cerebellar neoplasm or skeletal tuberculosis with cerebellar abscess formation was made. Magnetic resonance imaging (MRI) of brain revealed a lesion in the cerebellum suggestive of medulloblastoma (Figure 1) . Bone scan, performed for the evaluation of pain in the hip, revealed increased radiotracer (Tc99m-MDP) uptake in both the hips, multiple thoracic vertebrae and sternum suggesting metastatic deposits, however no lumbar vertebra was found to be involved (Figure 2) . Since the patient had pain and tenderness over the lumbar vertebrae, MRI of lumbar spine and hip was performed which revealed multiple areas of altered marrow signal intensity involving multiple lumbar vertebral bodies (Figure 3) and both femoral heads which were hypointense on T-1 weighted images and hyperintense on T-2 weighted and STIR images. The lesions showed abnormal enhancement on post-gadolinium images. These features were considered highly suggestive of metastatic deposits. Considering the discrepancy between the bone scan and the MRI findings of lumbar vertebrae, computed tomography-guided biopsy was obtained from the L3 vertebra, which revealed metastatic deposits from medulloblastoma (Figure 4) . Cerebrospinal fluid cytology showed the presence of medulloblastoma cells. A final diagnosis of cerebellar medulloblastoma with skeletal metastases was made. He was operated upon for the cerebellar primary and histopathology confirmed the lesion to be medulloblastoma. He received palliative radiotherapy of 64 Gray and a further course of cytotoxic chemotherapy was advised.
Discussion
CNS malignancies were once believed to not metastasize extracranially. In 1930 Bailey demonstrated that medulloblastoma tends to seed along the cerebrospinal fluid pathway.[3] In 1936 Nelson reported the first well-documented case of metastasis outside the central nervous system in a patient with cerebellar medulloblastoma.[4] In 1955 Weiss proposed rigid criteria for the diagnosis of extracranial metastasis from primary CNS malignancies.[5] These included a single histologically characteristic CNS tumour, a clinical history indicating a primary CNS lesion, a complete postmortem examination to exclude peripheral primaries and similar histological findings between the CNS and peripheral lesions. In our patient, all these criteria were fulfilled antemortem. Though medulloblastoma is considered to be a highly malignant tumour, metastasis from medulloblastoma outside the craniospinal axis is rare, with an overall incidence of around 7.1%.[6] Bone is the most frequent site for extracranial metastasis (77%), whereas liver is the most frequent (13%) abdominal viscus involved as reported by Rochkind et al.[6]
Glioblastoma multiforme and medulloblastoma are the two most common malignant brain tumours to spread outside the central nervous system, but the pattern of spread is different for each of these tumours. Skeletal metastases are two times more frequent in medulloblastoma than in glioblastoma.[6] Conversely, the lung is the most frequent site of involvement in glioblastoma (60%) but is much less frequently involved (13%) in medulloblastoma.[6]
There are three different histological sub-types of medulloblastoma, namely classical medulloblastoma, lipomedulloblastoma and medullomyoblastoma.[7] On microscopic examination the tumour is extremely cellular, with sheets of anaplastic cells. Individual tumour cells are small with little cytoplasm and hyperchromatic nucleoli that are frequently elongated or crescent shaped. Mitoses are abundant and markers for cellular proliferation such as Ki-67, are detected in a high percentage of cells. The tumour has the potential to express neurosecretory granules and Homer-Wright rosettes, as occur in neuroblastoma.[7]
No case of medulloblastoma has been described in English literature where skeletal metastasis was documented before any kind of intervention for the primary tumour. The iatrogenic haematogenous mechanism of metastatic spread was proposed to explain the development of metastasis following surgery. However Chretien reported a case of glioblastoma multiforme where metastasis developed in the absence of craniotomy where autopsy revealed invasion of dural venous sinuses by tumour mass, which could have facilitated haematogenous metastases.[8] This same mechanism could also have operated in this case of medulloblastoma.
The primary factors responsible for the rarity of extracranial metastasis are considered to be short postoperative lifespan of these patients, which does not allow metastasis to develop or manifest; absence of lymphatics in the central nervous system; early occlusion of venous channels due to compression by the tumour; and immune response to the tumour cells. On the other hand, it has been shown experimentally that primary brain tumour cells can keep on growing outside the central nervous system.[9]
The presence of skeletal metastases can change the treatment modality adopted for medulloblastoma; hence it is essential that a sensitive diagnostic modality be applied for the detection of skeletal metastases. This case has demonstrated that bone scan may not be able to detect all skeletal metastatic deposits, especially in the vertebrae and for the diagnosis of vertebral metastases MRI appears to be a superior modality.[10]
References
| 1. | Bellezza G, Pietropaoli N, Sidoni A. Medulloblastoma during pregnancy. Description of a case with extraneural metastases and review of the literature. Pathologica 1997;89:301-3. Back to cited text no. 1 [PUBMED] |
| 2. | Girolami UDe, Douglas C, Anthony, Frosch MP. The central nervous system. Pathologic basis of disease. Robins. 6th edition. Philadelphia: WB Saunders Company; 1999. p. 1348-9. Back to cited text no. 2 |
| 3. | Bailley P. Further notes on the cerebellar medulloblastomas. The effect of roentgen radiation. Am J Path 1930;6:126-36. Back to cited text no. 3 |
| 4. | Nelson A A. Metastases of intracranial tumours. Am J Cancer 1936;28:1-12. Back to cited text no. 4 |
| 5. | Weiss L. A metastasizing ependymoma of the cauda equina. Cancer 1955;8: 161-71. Back to cited text no. 5 [PUBMED] |
| 6. | Rochkind S, Blatt I, Sadeh M, Goldhammer Y. Extracranial metastases of medulloblastoma in adults: literature review. J Neural Neurosurgeon Psychiatry 1991;54:80-6. Back to cited text no. 6 [PUBMED] |
| 7. | McLendon RE, Provenzale J. Glioneuronal tumors of the central nervous system. Brain Tumor Pathol 2002;19:51-8. Back to cited text no. 7 [PUBMED] |
| 8. | Chretien F, Gray F, Funalot B, Authier FJ, Peltier E, Lange F, et al. Extracerebral metastases of a glioblastoma, in the absence of surgery. Arch Anat Cytol Pathol 1995;43:342-9. Back to cited text no. 8 [PUBMED] |
| 9. | Brisson C, Lelong-Rebel I, Mottolese C, Jouvet A, Fevre-Montange M, Saint Pierre G, et al. Establishment of human tumoral ependymal cell lines and coculture with tubular-like human endothelial cells. Int J Oncol 2002;21:775-85. Back to cited text no. 9 [PUBMED] |
| 10. | Gosfield E 3rd, Alavi A, Kneeland B. Comparison of radionuclide bone scans and magnetic resonance imaging in detecting spinal metastases. J Nucl Med 1993; 34:2191-8. Back to cited text no. 10 [PUBMED] |
Copyright 2004 - Journal of Postgraduate Medicine
The following images related to this document are available:
Photo images
[jp04034f1.jpg]
[jp04034f4.jpg]
[jp04034f3.jpg]
[jp04034f2.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}