
|
Journal of Postgraduate Medicine
Medknow Publications and Staff Society of Seth GS Medical College and KEM Hospital, Mumbai, India
ISSN: 0022-3859 EISSN: 0972-2823
Vol. 50, Num. 2, 2004, pp. 115-117
|
Journal of Postgraduate Medicine, Vol. 50, No. 2, April-June, 2004, pp. 115-117
Case Report
Abdominal mass secondary to actinomyces infection: An unusual presentation and its treatment
Sumer Y, Yilmaz Bilsel, Emre B, Ugur C
Departments of General Surgery and Pathology, Istanbul University, Istanbul Medical Faculty, 34390, Istanbul, Capa, Turkey
Correspondence Address:Departments of General Surgery, Istanbul
University, Istanbul Medical Faculty, 34390, Istanbul, Capa tbilsel@superonline.com
Code Number: jp04036
Abstract
Abdominal actinomycosis may appear as an abdominal mass and/or abscess. This mass can mimic a malignant tumour. The diagnosis and management of abdominal actinomycosis will be discussed through a review of the literature and a case report from our own institution. The patient was a 17-year-old boy who presented with abdominal discomfort and a palpable right lower quadrant mass defined on CT scan. He underwent en bloc resection of the mass for a presumed diagnosis of tumour of uncertain type with intestinal involvement. The diagnosis was reversed, when histology revealed filamentous organisms consistent with actinomyces. He was treated with high dose penicillin for several weeks and was discharged from the hospital taking penicillin orally.
Preoperative diagnosis of abdominal actinomycosis is difficult. An accurate diagnosis is always obtained in a histological or microbiological examination, often requiring surgical resection. Recognition is important because successful treatment requires combined surgery and prolonged penicillin treatment.
Keywords: Abdominal actionomycosis, Abdominal mass/abscess, Diagnosis, Treatment
Actinomycosis is a chronic infection produced by opportunistic organisms that normally colonize the upper respiratory tract, gastrointestinal tract, and female genital tract. Actinomyces israelii is the most common pathogenic species. The organisms have a low virulence potential and cause disease only when the normal mucosal barrier is broken, leading to multiple abscess formation, fistula, or a mass lesion.[1] The areas of suppuration are commonly surrounded by fibrosing granulation tissue, which gives the surface overlying the involved tissues a hard or woody consistency. We present a case of abdominal actinomycosis with a picture of abdominal mass that was incorrectly diagnosed at operation as a malignant tumour of the small intestines.
Case History
A 17 year-old male was admitted to our hospital with severe right lower abdominal pain and fever that had persisted for two months. He stated that two months previously, he had experienced a periumblical pain, which radiated to the right iliac fossa after several hours. A urinary infection had been diagnosed in another hospital and he had been prescribed parenteral gentamycin for 15 days. There was no change in the nature of the discomfort. A few weeks later the pain intensified and was localized to the right lower quadrant. There were no gastrointestinal or urogenital symptoms.
On admission, his temperature was 37.7°C and he looked pale. Physical examination revealed a firm and tender mass in the right lower quadrant, without rebound tenderness. On digital rectal examination there was a tender mass palpated at pouch of Douglas.
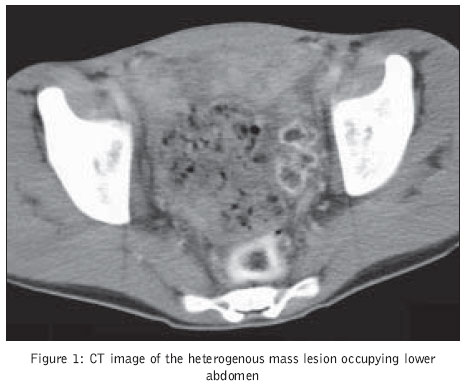
Laboratory results were all within the reference range except for a mild leucocytosis (12.700/mm3), and an erythrocyte sedimentation rate of 110 mm in the first hour. Ultrasonography of the lower abdomen showed a mixed hypoechogenic and hyperechogenic mass measuring 90 x 140 mm and grade II right hydronephrosis. This was verified by a computed tomography that showed an ill defined abdominal mass with numerous fluid collections that contained air suggesting abscess formation and a hydronephrosis on right side (Figure 1) . The small bowel proximal to the diseased area appeared to be dilated.
We decided to make a laparotomy with a presumptive diagnosis of periappendicular abscess due to a ruptured appendicitis. Under general anaesthesia, a median laparotomy was performed after the placement of a right pig-tail catheter into the right ureter by cystoscopy. At exploratory laparotomy we found a mass of about 10 cm diameter surrounded by a fibrous capsule, together with a number of cavities bordered by necrotic material, in which the cecum and terminal ileum were involved. Similar lesions of 1 to 3 cm in diameter were also seen scattered along the transverse mesocolon and ileal mesentery. Although the appearance was mimicking tumour of the small intestines, there was no true invasion of the neighbouring structures. Therefore, en bloc excision of the mass was performed, which required removal of 60 cm of distal ileum and caecum, and an end to side anastomosis was performed between the ileum and the ascending colon. The other lesions were excised separately. Postoperatively, the patient recovered uneventfully.
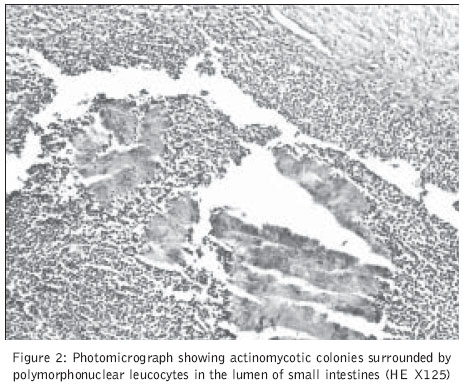
After the histological examination, the diagnosis of tumour of uncertain type with intestinal involvement was reversed. Microscopy showed the mass to be of an inflammatory nature, composed of fibrous tissue, granulation tissue and inflammatory cells. Within a focus of suppuration groups of radiating gram-positive filamentous organisms were seen consistent with the diagnosis of actinomyces (Figure 2) . Appendix was assumed to be the possible source of infection. The patient was given 12 million units of penicillin G per day for four weeks, and followed by oral amoxicillin for 6 months. The ureteral catheter was removed at postoperative 1st month. At follow-up he was well and a control CT scan at first year showed no recurrence of the disease.
Discussion
The overall incidence of registered cases of actinomycosis is decreasing. Pelvic and abdominal actinomycosis, however, are increasing in frequency.[2] This is predominantly related to long-term, indwelling, intrauterine devices (IUD), particularly after their removal. The close association between actinomyces infection and the use of IUD is well documented, with over 90 reported cases in the literature.[3],[4]
Abdominal actinomycosis is one of the greatest challenges for diagnosis. It has been called "one of the greatest imitators in clinical practice".[5] It is uncommon and accounts for 20 % of actinomycosis infection.[6] Delayed diagnosis is the rule rather than the exception. It presents as an indolent chronic suppurative process with atypical symptoms that are often misinterpreted as malignant disease; the correct diagnosis is usually achieved only at operation. The appendix is the most frequently involved organ, which once ruptured stimulates pathologic growth of these organisms and causes right- sided symptoms.[6] When outside the intestine, actinomycosis generally grows by local spread with only rare incidences of haematogenous or lymphatic dissemination.[7] The localised response manifests in abscess formation.
Actinomyces is an obligate anaerobe, and requires the presence of many other types of bacteria to proliferate. This ecosystem destroys local tissue in any highly vascularised region and replaces it with a poorly irrigated granulated tissue, permitting an anaerobic milieu.[8] There is no specific radiological evidence or endoscopic appearance of the disease. The isolation of the organism is also quite difficult. The definitive diagnosis is often based on recognition of typical sulphur granules in the abscess material.
Despite the good response to penicillin treatment, cure is rarely achieved without operation to eradicate the inflammatory process. Therefore, surgical debridment remains a mainstay of therapy.[9] The usual recommended antibiotic regimen is intravenous penicillin G (18-24 million units/day) for 2-6 weeks, followed by oral penicillin or amoxicillin for 6-12 months.[10] For patients allergic to penicillin, tetracycline, erythromycin, minocycline, and clindamycine are good alternatives.[10]
A number of conclusions can be drawn from this case and review of the literature. First, clinical and imaging findings are likely to suggest the presence of malignancy, and tissue specimens are necessary for exact diagnosis. Second, precipitating factors of abdominal actinomycosis include gastrointestinal surgery, inflammation (acute appendicitis, diverticulitis) and IUD in many pelvic cases in women. Third, extensive resection is useful therapeutically for the purpose of debulking. Finally, antibiotic treatment is necessary for complete cure, and should be given for several months in order to prevent recurrence.
References
| 1. | Berardi RS. Abdominal actinomycosis. Surg Gynecol Obstet 1979;149:257-66. Back to cited text no. 1 [PUBMED] |
| 2. | Yeguez JF, Martinez SA, Sands LR, Hellinger MD. Pelvic actinomycosis presenting as malignant large bowel obstruction: a case report and a review of the literature. Am Surg 2000;66:85-90. Back to cited text no. 2 [PUBMED] |
| 3. | Fiorino AS. Intrauterine contraceptive device associated actinomycotic abscess and actinomyces detection on cervical smear. Obstet Gynecol 1996;87:142-9. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Chaudhuri S, Billings PJ. Intra-abdominal actinomycosis presenting as complex abdominopelvic mass. J Indian Med Assoc 2002;100:463-4. Back to cited text no. 4 [PUBMED] |
| 5. | Dayan K, Neufeld D, Zissin R, Bernheim J, Paran H, Schwartz I et al. Actinomycosis of the large bowel: Unusual presentations and their surgical treatment. Eur J Surg 1996;162:657-60. Back to cited text no. 5 [PUBMED] |
| 6. | Davies M, Keddie NC. Abdominal actinomycosis. Br J Surg 1973;60:18-22. Back to cited text no. 6 [PUBMED] |
| 7. | Meyer P, Nwariaku O, McClelland RN, Gibbons D, Leach F, Sagalowsky AI, et al. Rare presentation of actinomycosis as an abdominal mass: report of a case. Dis Colon Rectum 2000;43:872-5. Back to cited text no. 7 [PUBMED] |
| 8. | Miller M, Haddad AJ. Cervical actinomycosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:496-508. Back to cited text no. 8 [PUBMED] |
| 9. | Wagenlehner FME, Mohren B, Naber KG, Mannl HFK. Abdominal actinomycosis. Clin Microbiol Infect 2003;9:881-5. Back to cited text no. 9 |
| 10. | Russo TA. Agents of actinomycosis. In: Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious diseases. 4th ed. New York: Churchill Livingstone; 1995. p. 2280-8. Back to cited text no. 10 |
Copyright 2004 - Journal of Postgraduate Medicine
The following images related to this document are available:
Photo images
[jp04036f2.jpg]
[jp04036f1.jpg]
|

{kind=link}
{kind=link}