
|
Journal of Postgraduate Medicine
Medknow Publications and Staff Society of Seth GS Medical College and KEM Hospital, Mumbai, India
ISSN: 0022-3859 EISSN: 0972-2823
Vol. 50, Num. 2, 2004, pp. 125-126
|
Journal of Postgraduate Medicine, Vol. 50, No. 2, April-June, 2004, pp. 125-126
Images in Medicine
Juvenile hyaline fibromatosis
Nischal KC, Sachdev D, Kharkar V, Mahajan S
Department of Dermatology, Seth G. S. Medical College
and KEM Hospital, Parel, Mumbai - 400012, India
Correspondence Address:Department of Dermatology, Seth G. S. Medical College
and KEM Hospital, Parel, Mumbai - 400012 kc_nischal@yahoo.com
Code Number: jp04040
An 18-month-old female child born of a second degree consanguineous marriage presented with asymptomatic, pink, raised lesions on the body since the age of six months and boggy swellings on the scalp since the age of 12 months. There was a gradual increase in the size of the skin and scalp lesions. A progressive, painless, flexion deformity of both the upper and lower limbs was noticed since birth. Other siblings and parents were unaffected.
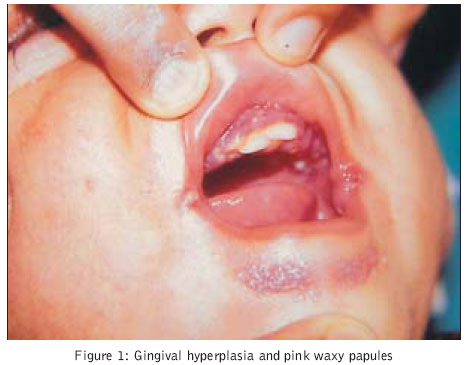
Examination revealed gingival hyperplasia (Figure1) and fixed flexion contracture of both elbows (Figure 2) and knee joints. Multiple, firm, non-tender, pink, waxy papules and nodules were symmetrically distributed over the angle of the mouth (Figure 1) , nasolabial folds, retroauricular region, nape of the neck and the dorsae of finger joints. The papules had coalesced to form plaques in the perianal region. There were three, soft, skin-coloured, boggy, non-tender, mobile, variable-sized masses, measuring up to 5 cm in diameter, over the parietal and occipital eminences of the scalp. There was no significant lymphadenopathy or hepatosplenomegaly. Her head circumference was 52 cm. Her weight and height were 6.25 kg (<5th percentile) and 67cm (<5th percentile) respectively, implying Grade IV malnutrition.
Evaluation of her milestones revealed delayed dentition and restriction of language development to production of a few meaningful words only. Though she could sit without support, she was unable to stand even with support. Hand to mouth co-ordination was poor due to contractures at elbow joints. Her social age was 6-7 months by the Vineland Social Maturity Scale and her social quotient was 33 (normal 90-100). Thus, she had severe mental retardation and delayed motor development. Her haemogram, biochemical profile, VDRL, ECG and chest roentgenogram were normal. Antinuclear antibodies and rheumatoid factor were negative. Hearing and vision were normal. Screening for inborn errors of metabolism and lysosomal disorders yielded normal results. Roentgenogram of the skull and CT scan brain revealed multiple osteolytic lesions and soft tissue masses. Biopsy of the scalp and neck lesion revealed homogenous eosinophilic hyaline deposits in the dermis with fibroblasts surrounded by empty spaces due to shrinkage artefact, giving them a ′chondroid′ appearance. Pale blue deposits of mucin were seen in the dermis with Alcian blue and PAS stain. Thus, based on the above clinicopathological findings, a diagnosis of Juvenile hyaline fibromatosis (JHF) was reached. Parents were counselled about the progressive nature of this disorder and prognosis. Passive physiotherapy exercises were advised for improving joint mobility along with surgical excision of the scalp lesions.
Discussion
JHF is a rare, crippling autosomal recessive disorder, first described by McMurray in 1873 as Molluscum Fibrosum and renamed by Kitano as JHF in 1972.[1] It is diagnosed based on clinical findings of cutaneous lesions, gingival hyperplasia, joint contractures and osteolytic lesions. Severe gingival hyperplasia can interfere with eating and delay dentition too. Joint contractures, the earliest and the most constant feature cripple patients and retard normal motor development when they occur in early infancy. A total of 68 cases have been reported in the world literature. Mental development is usually normal.[1] To the best of our knowledge, this is the first case report of JHF with severe mental retardation.
Infantile Systemic Hyalinosis (ISH) is a condition similar to JHF but with severe multiple internal organ involvement and a poorer prognosis. Winchester syndrome, lipoid proteinosis[1] and other fibrous proliferations of infancy and childhood have to be considered in the differential diagnosis.[2] Various abnormalities in the biosynthesis of glycosaminoglycans and defects in collagen III and VI have been reported.[3] Recently, further investigation of chromosome 4q21[1] JHF disease locus has revealed mutations in the capillary morphogenesis factor-2 gene (CMG2) in both JHF, and ISH.[4],[5] Thus, JHF and ISH are postulated to be allelic disorders. The disease has a relentlessly progressive course,[1] with most patients surviving only up to the 4th decade. As of now, there is no specific treatment for this disorder. Genetic counselling is essential to explain to parents about a 25% chance of having a diseased baby in any pregnancy. With the gene for the disease being mapped recently, techniques for antenatal diagnosis are likely to be established.
References
| 1. | Rahman N, Dustan M, Teare MD, Hanks S, Edkins SJ, Hughes J, et al. The gene for Juvenile Hyaline Fibromatosis maps to 4q21. Am J Hum Genet 2002;71:975-80. Back to cited text no. 1 |
| 2. | Bigler C, Burgdorf WHC. Benign neoplasm, premalignant conditions and malignancy. In: Schachner LA, Hansen RC, editors. Pediatric Dermatology. 2nd edn. New York: Churchill Livingstone Inc; 1995. p. 998-1001. Back to cited text no. 2 |
| 3. | Breier F, Fang-Kircher S, Wolff K, Jurecka W. Juvenile hyaline fibromatosis: impaired collagen metabolism in human skin fibroblasts. Arch Dis Child 1997;77: 436-40. Back to cited text no. 3 |
| 4. | Hanks
S, Adams S, Douglas J, Arbour L, Atherton DJ, Balci S, et al. Mutations in
the gene encoding capillary morphogenesis protein 2 cause juvenile hyaline
fibromatosis and infantile systemic hyalinosis. Am J Hum Genet 2003;73:791-800. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Dowling
O, Difeo A, Ramirez MC, Tukel T, Narla G, Bonafe L, et al. Mutations in capillary
morphogenesis gene-2 result in the allelic disorders juvenile hyaline fibromatosis
and infantile systemic hyalinosis. Am J Hum Genet 2003;73:957-66. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
Copyright 2004 - Journal of Postgraduate Medicine
The following images related to this document are available:
Photo images
[jp04040f2.jpg]
[jp04040f1.jpg]
|

{kind=link}
{kind=link}