 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
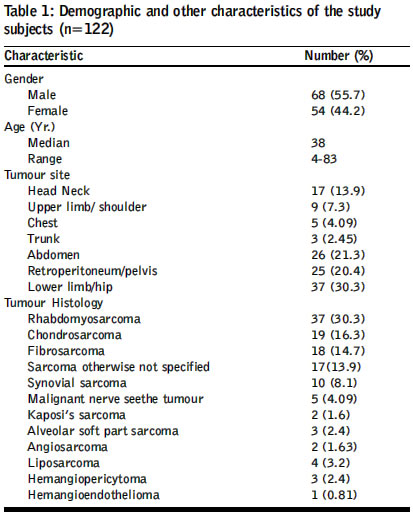
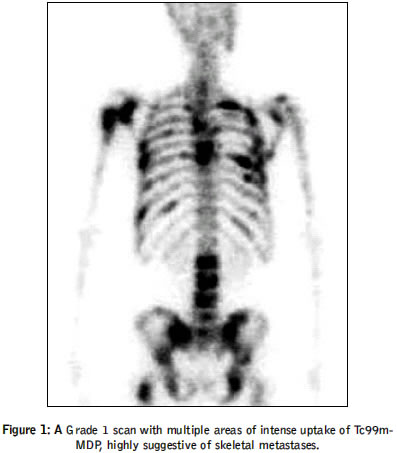
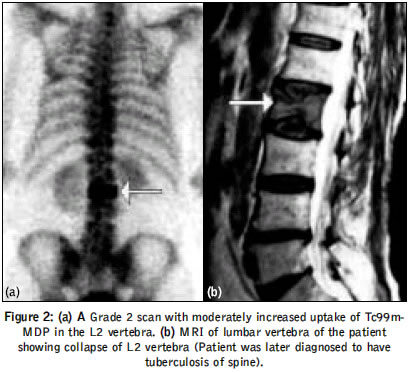
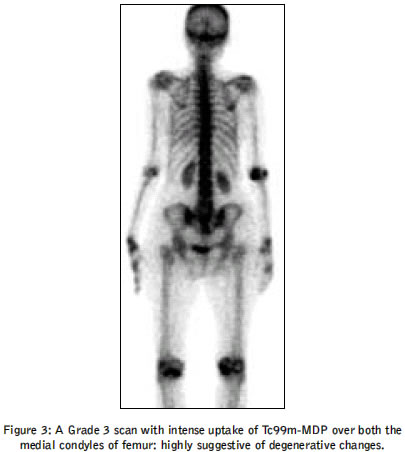
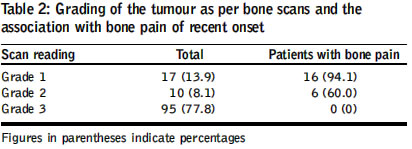
Journal of Postgraduate Medicine, Vol. 50, No. 3, July-September, 2004, pp. 180-184 Original Article Role of skeletal scintigraphy in soft tissue sarcoma: Improving the diagnostic yield Barai Sukanta, Bandopadhayaya GP, Chumber S, Gupta DK, Patel CD, Dhanpati H Department of Nuclear Medicine, All India Institute of Medical Sciences, New Delhi Code Number: jp04058 Abstract Background: The presence of skeletal metastases significantly influences the therapeutic strategy adopted for soft tissue sarcoma. However, literature on the prevalence of skeletal metastases in soft tissue sarcoma is limited and none of the available data is based on the Indian patient population. Aim: To determine the prevalence of skeletal metastases at presentation in patients of soft tissue sarcoma and to rationalise the use of preoperative skeletal scintigraphy in such patients. Methods and Material: Preoperative bone scans were evaluated in 122 patients with soft tissue sarcoma (median age, 34 years; range, 4-83). The scans were classified into 3 grades: Grade 1: metastases very likely; Grade 2: equivocal; Grade 3: normal or benign lesion. In all the patients studied, the ability of the patient to localize the site or sites of pain was recorded and that was correlated with the site of metastases in scintigraphy. Result: Seventeen (13.9%) patients had Grade 1 scan; 16 of them had bony pain that was not readily explainable by trauma or other local factors. Ten ( 8.1%) patients had Grade 2 scan, five of them had bony pain which was not readily explainable by trauma or other local factors. Ninety-five patients (77.8%) had Grade 3 scan. Of these, 9 had localised bone pain which could be definitely associated with trauma or joint degeneration. Conclusion: The prevalence of skeletal metastases at presentation in patients with soft tissue sarcoma is low (13.9%). The low rates of skeletal metastases in bone pain-free patients (0.9%) versus the high rate in symptomatic patients (76.1%) supports the use of bone scanning in symptomatic patients only. KEY WORDS: Skeletal metastases, scintigraphy, soft tissue sarcomas Soft tissue sarcomas are a heterogeneous group of malignancies arising from mesenchymal structures accounting for around 1% of all cancers.[1] They are locally aggressive and frequently invade the surrounding structures. The therapeutic strategy adopted for their treatment depends on the type of tumour, its site and presence of local invasion or distant metastasis.[2] At presentation, systemic spread of the disease is not very common, with frequencies ranging from 7%-25%.[3],[4],[5] The most common site of metastasis is the lung but bones are also involved.[6] The presence of skeletal metastases significantly influences the therapeutic strategy adopted. However, there is limited literature estimating the prevalence of skeletal metastasis in patients with soft tissue sarcoma and none of it is based on the Indian patient population. As genetic, ethnic and racial factors are known to influence the incidence and behaviours of several malignancies, a study was undertaken to determine the prevalence of skeletal metastasis at presentation in Indian patients with soft tissue sarcoma and to rationalise the use of preoperative skeletal scintigraphy in such patients. Materials and Methods Preoperative bone scans were performed in 122 consecutive patients of soft tissue sarcoma (median age, 34 years; range, 4-83) who had undergone skeletal scintigraphy between 1999 and 2003. Thirty-six patients were under the age of eighteen. Patient and tumour characteristics are presented in [Table - 1]. Pathological diagnosis was based on tumour material obtained from a diagnostic biopsy or during therapeutic resection. Bone scan was performed before resection of tumour as a part of standard metastatic work-up along with skeletal survey, CT scanning of chest and ultrasound of abdomen. The presence or absence of skeletal pain and location of pain were evaluated and recorded in the pre-scan clinical examination. Bone scan was performed 3 hours post-intravenous administration of 185-1000 MBq (5-27m Ci) of Tc99m-Methylene diphosphonate (Tc99m-MDP) using a dual head single photon emission computed tomography system fitted with low-energy high resolution collimator (Varicam and millennium VG from General Electric, Milwaukee, USA). Dose was calculated as body surface area divided by 1.73 and then multiplied by the adult dose of 1,000 MBq. Whole body acquisition was done using step and shoot method with 180 seconds per view. For any spinal lesion, single photon emission computed tomography (SPECT) of the involved vertebral lesion was performed. Bone SPECT was acquired in a 128 x 128 matrix with 90 views at every 4° for 25 seconds per view were obtained. Projection data was prefiltered before back projection and reconstruction performed with a two-dimensional hanning filter (cut off=0.23 cm, P=50). Attenuation correction was done by Chang′s method.[7] No scatter correction was done. Reconstructed images had a slice thickness of 7 mm and were displayed and analysed using transverse, sagittal and coronal views. Two experienced nuclear medicine physicians evaluated the scan findings independently and both of them were blinded to the findings of other investigators but were aware of the primary disease and its location. Abnormally increased radiotracer uptake away from joints, which is not readily explainable by trauma or other local factors, was considered as skeletal metastasis. Scans were classified into three Grades: Grade 1 (high probability scan for skeletal metastases), Grade 2 (definite characterisation as malignant or benign lesion not possible), or Grade 3 (normal or certainly benign lesions). The presence or absence of bone metastases was determined based on the combination of bone scan findings, the results of other investigations (absence or presence of typical sclerotic lesions on X-rays, appearance of tumour tissue in bone, bone cortex defect, or signal changes as visible in CT or magnetic resonance imaging [MRI], and a follow-up bone scan whenever available. Results Grade 1 scans were found in 17 of 122 patients (13.9%); all bone metastases were confirmed by additional investigations [Figure - 1]. Sixteen of these patients reported pain and the site of pain could not be definitely associated with trauma or joint degeneration. One patient had no pain or discomfort over any of the sites of skeletal metastasis. Grade 2 (definite characterisation as malignant or benign lesion not possible) scans were present in 10 of 122 patients (8.1%). All these patients underwent further investigations, which excluded skeletal metastases. In 3 patients the equivocal lesion was in the same bone region involved but was distinctly separated from the primary soft tissue mass. Seven patients had increased tracer uptake over vertebra, but the intensity of increased tracer uptake was not sufficient to place them into Grade 1. MRI of spine, performed in these patients revealed only degenerative changes [Figure - 2]a,b. Five patients with Grade 2 scan complained of bone pain which could not be readily explained by trauma or joint degeneration. Grade 3 (normal) bone scans were found in 95 patients (77.8%) [Figure - 3]. Lesions described as ′almost certainly benign′were usually the result of degenerative disease of the spine or clearly caused by recent trauma (focally increased rib uptake over the site of pleural tap in 2 patients). Nine of these patients also had localised bone pain but that could be definitely associated with trauma or joint degeneration, and hence excluded from further analysis of results. Skeletal survey performed in these patients excluded any skeletal metastases. Overall, in 3 cases (3.06%), there was a difference in interpretation between two observers as Grade 2 versus Grade 3 and that was resolved by consensus. Overall, bone pain was present in 22 patients (excluding those patients where pain was due to trauma and degenerative joint disease). Of these, in 16 patients (72.7%) [Table - 2], this pain could be correlated to bone metastases. Hence skeletal metastases were present in 76.1% patients with bone pain as against only in 0.9% patients without bone pain. Discussion In this study, routine bone scan had a relatively low yield. Therefore, if bone scan had been obtained only in the 21(17.2%) patients with bone pain, 101(82.7%) bone scans could have been avoided. In that case bone metastases would have been missed in one patient without bone pain. This patient had clinically advanced disease with lung and brain metastasis. Bone scans in this patient revealed extensive skeletal metastases. Therefore, the clinical yield would have been almost the same if bone scan had been performed only in patients with bone pain and would have saved 101 unnecessary bone scans. As a method to detect skeletal metastases, skeletal scintigraphy proved to be accurate. All cases of Grade 1 scan indeed had skeletal metastases, as evidenced by other imaging studies whereas all cases with a Grade 3 reading were free of bone metastases. The equivocal group (Grade 2 reading) was relatively small (8.1%) and no bony metastases were found. Several investigators have reported a low incidence of skeletal metastases in soft tissue sarcoma (STS) patients. Yoshikawa et al reported an incidence of 9.4% in a series of 320 patients.[8] Jager et al reported an incidence of 7% in a series of 109 patients.[9] Our study revealed a slightly higher prevalence (13.9%) of skeletal metastases as compared to other studies. This could be partly due to referral bias and partly due to a larger proportion of those tumours, which produce skeletal metastases more frequently like rhabdomyosarcoma and poorly differentiated soft tissue sarcoma. Isolated skeletal metastases were present in 5 patients. However, lung metastases were more common than bone metastasis. Twenty-one patients had lung metastases and one patient had cerebral metastasis. There is no widely accepted view on the level of incidence of skeletal metastases that justifies routine bone scan in all patients. Skeletal scintigraphy is a very sensitive modality for the detection of skeletal metastases but has poor specificity. Trauma, degenerative disease, and inflammatory disease also cause increase in tracer uptake which can sometimes mimic skeletal metastasis. However, the pattern of abnormalities together with detailed clinical history increases the specificity of bone scan. In case of multiple lesions randomly spread all over the skeleton, the likelihood of bone metastasis is very high. Conversely, if the bone scan is normal it virtually rules out the possibility of skeletal metastasis. In many cases the pattern of abnormalities does not follow a specific pattern and further investigations are required to exclude the possibility of skeletal metastasis. Bone scanning with its high sensitivity and low specificity is cost- effective only when applied to a subgroup of patients with increased risk of skeletal metastases. Bone pain of relatively recent onset has been suggested as a predictor of the presence of skeletal metastasis.[9] Our study also demonstrates the utility of bone pain of recent onset as a predictor of the presence of skeletal metastasis; 76.1% patients with bone pain had skeletal metastasis whereas only 0.9% of patients without bone pain had skeletal metastasis. Apart from the use in staging the disease, bone scan is also performed to detect local bone involvement by the soft tissue sarcoma. However, MRI and CT scan studies have been demonstrated to be more precise, especially CT scans which reliably detect defects in the bone cortex.[10],[11] A bone scan can be false positive in this scenario due to tumour-associated local hyperemia, though bone scan is occasionally performed when anatomical imaging studies are equivocal. A limitation of the study was the absence of follow-up bone scan in Grade 3 patients. However, bone metastases were not confirmed in any of the patients with even more abnormal bone scan (Grade 2) who did have extensive metastatic work-up and serial follow-up bone scan. It could be concluded that skeletal metastases at presentation in soft tissue sarcoma patients are low (13.9%). The low rates of skeletal metastases in bone pain-free patients (0.9%) versus the high rate in symptomatic patients (76.1%) supports the use of bone scanning in symptomatic patients only. References
Copyright 2004 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp04058f3.jpg] [jp04058t1.jpg] [jp04058f2.jpg] [jp04058t2.jpg] [jp04058f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}