 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
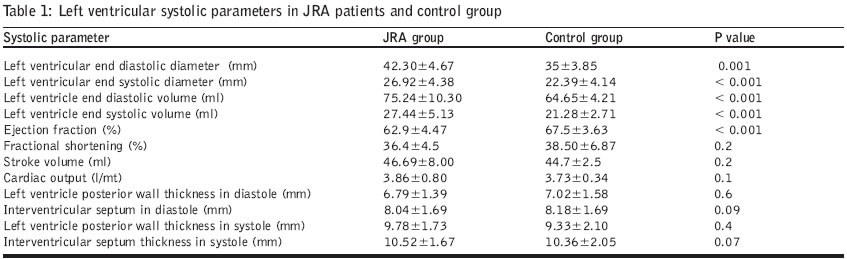
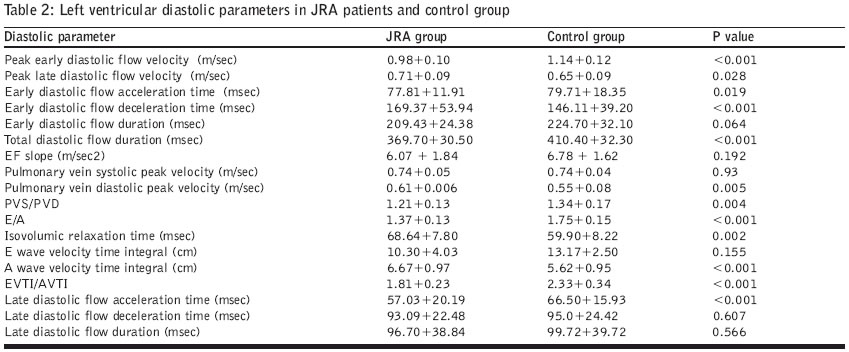
Journal of Postgraduate Medicine, Vol. 50, No. 4, October-December, 2004, pp. 262-267 Original Article Assessment of left ventricular systolic and diastolic function in juvenile rheumatoid arthritis Bharti Bishwa BhushanB, Kumar Sudeep, Kapoor Aditya, Agarwal Amita, Mishra Ramnath, Sinha Nakul Departments of Cardiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow Code Number: jp04090 ABSTRACT Background and Aims: Recognizing the paucity of data regarding echocardiographic studies of Left ventricular (LV) systolic and diastolic function in patients with juvenile rheumatoid arthritis (JRA), a study was carried out to study these parameters in these subjects.Settings, Design and Methods: Thirty-five patients with JRA and an equal number of age- and sex-matched controls were studied by two-dimensional and Doppler echocardiography. Results: Patients with JRA had higher systolic and diastolic blood pressures, resting heart rates, LV systolic (26.9±4.3 vs. 22.4 ± 4.1 mm, p=0.001) and diastolic size (42.3±4.6 vs. 35.4±3.8 mm, p<0.001) and volumes. Though ejection fraction (EF) and fractional shortening (FS) were normal, they were lower in those with JRA as compared to controls (EF: 62.9±4.47 vs. 67.5±3.63 %, p<0.001; FS: 36.4±4.5 vs. 38.5 ± 6.87, p=0.2). On Doppler analysis the JRA group had lower peak E velocity, higher peak A velocity, higher A VTI and more prolonged IVRT. Male patients had higher A VTI and IVRT as compared to females. Those with longer duration of disease had larger LV systolic (r=0.517, p=0.01) and diastolic dimension (r=0.40, p=0.05) and lower FS (r=-0.506, p=0.01). Patients with polyarticular JRA had higher E and A VTI as compared to those with systemic or oligoarticular types. Conclusion: Despite an asymptomatic cardiac status, significant systolic and diastolic functional abnormalities exist in patients with JRA. The duration of the disease, mode of presentation, patient’s age and gender have a significant impact on the left ventricular systolic and diastolic functions in patients with JRA. KEY WORDS: Juvenile rheumatoid arthritis, diastolic dysfunction, systolic dysfunction Juvenile rheumatoid arthritis (JRA) is the commonest cause of chronic inflammatory arthritis in childhood. Cardiac (pericardial, myocardial or endocardial) involvement is known to occur in patients with JRA, as it does in adults with rheumatoid arthritis (RA). Though pericarditis is identifiable in nearly 45% cases at autopsy, clinical manifestations of pericardial involvement are much less commonly observed.[1] Endocardial involvement leads to aortic and mitral valve incompetence, and usually occurs in late onset oligoarthritis type of JRA. Clinical manifestations are usually mild and surgery is rarely required.[2] Myocardial involvement may present as congestive heart failure or arrhythmias. Though systolic and diastolic functions of the left ventricle (LV) have been frequently studied in adults with RA, similar data on JRA is scarce.[3],[4] Moreover, no previous study has attempted to correlate whether variables like duration of disease, mode of presentation, age and gender of patients have any effect on LV systolic and diastolic function in patients with JRA. The aim of the study was to undertake a detailed analysis of LV systolic and diastolic functions in patients with JRA and analyse the effect of patient-related variables on these functional parameters. MATERIALS AND METHODS Thirty-five children with JRA (American College of Rheumatology criteria) 5 seen in the department of Clinical Immunology outpatient clinic between January 2001 and January 2002 were included in the study after obtaining verbal informed consent from parents or eligible and competent adult patients. The control group consisted of children presenting to the paediatric outpatient department and included 35 age- and sex- matched healthy controls. All patients underwent a detailed echocardiography, which included an M-mode, two dimensional, colour and Doppler (continuous and pulse wave) examination. Images were obtained on a Hewlett-Packard Sonos 5500 with a 4 MH transducer. Recordings were performed with subjects in the supine or left lateral positions. M-mode tracings were obtained at the level of tips of mitral leaflets in parasternal long axis position and measurements of left ventricular end-systolic dimension (LVESD), LV end-diastolic dimension (LVEDD) were performed according to the recommendations of the American Society of Echocardiography.6 The left ventricular end-diastolic and end-systolic volumes (LVEDV, LVESV) were calculated from the apical four-chamber view, using the ellipsoid single plane algorithm. The end-systolic and end-diastolic frames from five consecutive beats were selected and the endocardial outlines were traced. Mean left ventricular volumes and ejection fraction were automatically calculated using an in-built software in the echocardiography system. Cardiac output was measured by multiplying heart rate with stroke volume. LV diastolic function was assessed by measuring the mitral flow velocity recorded in the apical four-chamber view. The pulse Doppler sample volume was placed in the left ventricular inflow tract at the level of mitral leaflet tips and three consecutive measurements were averaged. The various variables of diastolic function that were measured included: (1) peak early (E; m/sec) and peak atrial filling velocity (A; m/s), (2) ratio of E to A (E/A), (3) E acceleration time (Eat; m/s), (4) E deceleration time (Edt; m/s), (5) E duration (Edur; msec), (6) Total duration (Tdur; msec), (7) ratio of Edur/Tdur, (8) E deceleration slope (Efslp; m/sec2), (9) E wave velocity time integral (E VTI, cm), (10) A wave velocity time integral (A VTI; cm), (11) ratio of E VTI to A VTI, (12) A acceleration time (Aat; m/s), (13) A deceleration time (Adt; m/s), (14) A duration (A dur; ms), (15) ratio of A duration by Total duration (Adur/Tdur), (16) isovolumic relaxation time (IVRT; ms), (17) pulmonary vein systolic peak flow (PVS; m/s), (18) pulmonary vein diastolic peak flow (PVD; m/s), (19) ratio of PVS to PVD (PVS/PVD). Isovolumic relaxation time (IVRT) was measured in the apical five-chamber view with the sample volume placed between the aorta and mitral valve where the recordings of both valves were taken simultaneously. STATISTICAL ANALYSIS All data are expressed as mean and standard deviation. Student′s t test was used for inter-group comparisons. Pearson correlation coefficient test was used to assess the degree of association between different variables. For comparing three groups (in analysing according to types of presentation), comparison was done by analysis of variance to see the significant difference amongst the three groups (p<0.05 taken as significant). RESULTS The study population included 35 patients with JRA (23 males, 12 females). The mean age of patients was 15.03 ± 5.3 years (range 7-28 yrs) while the mean duration of disease was 51.8 ± 41.6 months (range 2 -168 months). The mean heights (145.7±16.6 vs. 139 ± 24 cm, p=0.3) and weight (35.5±11.6 vs. 35.0±14.2 kg, p=0.8) were comparable among patients and controls. JRA was of the polyarticular type in 16/35 (45.71%), oligoarticular type in 11/35 (31.43 %) and systemic type in 8/35 (22.86%). The Rheumatoid factor (RF) was positive in 3 (8.6%) subjects. The mean concentration of haemoglobin in patients was 10.2 ±1.9 gm% and the mean ESR at the end of one hour was 44.8 ± 19.5. None of the patients had any symptoms related to cardiovascular involvement, nor were there any abnormal auscultatory findings among them. The systolic (120.06+8.03 vs. 106.05 +5.10 mm Hg, p <0.001) and diastolic blood pressures (77.25+2.6 vs. 63.16+6.08, p <0.001) were significantly higher among patients with JRA as compared to the corresponding values found in controls, though the absolute values were within the normal limits for this population. Resting heart rates were also higher (85.21±9.57 vs. 79.9±6.14 bpm, p = 0.02) among the patients as compared to controls. Patients with JRA had significantly higher LVESD and LVEDD [Table - 1]. In view of the enlarged LV size, patients with JRA also had significantly higher LVEDV and LVESV. Though EF and FS were within the normal range, the values were lower among patients with JRA as compared to controls, with only the difference in EF reaching statistical significance [Table - 1]. The stroke volume and cardiac output were comparable between the two groups. Significant differences were observed in almost all diastolic parameters in patients of JRA as compared to controls [Table - 2]. Peak trans-mitral E velocity was lower and Peak A velocity was higher amongst the patients with JRA. This was also reflected by the E/A velocity ratio, which was significantly lower among patients as compared to the healthy population. Though E VTI was similar in the two groups, patients with JRA had a much higher A VTI when compared to controls. This led to significantly lesser E VTI/A VTI values in patients with JRA. Eat, Aat and E duration were significantly lower and Edt was significantly longer amongst patients as compared to controls [Table - 2]. IVRT was significantly more prolonged in patients with JRA, though the absolute mean values were still in the normal range. Though PVS velocities were comparable in the two groups, PVD velocities were significantly higher amongst patients, thus leading to much lower PVS/PVD ratios in the patient population. None of the patients had aortic or mitral valve involvement. The mean left atrial size (27.3±5.1 vs. 27.4±4.9 mm, p=0.9) and mean Aortic dimension (24.1±3 vs. 22.9±5.1 mm, p=0.4) were also comparable between the two groups. Lack of any significant aortic valvular involvement was also borne out by the fact that the mean aortic annulus (17.8±2.5 vs. 17.9±4.1 mm), mean aortic velocity (1.29±0.2 vs. 1.17±0.2 cm/sec), and mean aortic VTI (23.1 ± 5.7 vs 22.7 ± 5.2 cm) were not significantly different among the two groups. Patient age had a significant correlation with LVED dimension (r=0.410, p=0.02) and SV (r=0.436, p=0.01). There was no correlation with LVESV, LVEDV, CO, EF and any of the LV diastolic function parameters. There was no correlation between gender and any systolic function parameters. Of the diastolic parameters, gender correlated significantly only with A VTI (r=-0.433, p<0.01) and IVRT (r=-0.375, p=0.03). Males had higher values of A VTI (6.98±0.98 vs. 6.06±0.54 cm, p=0.002) and IVRT (69.43±6.01 vs. 63±10.2, p=-0.03) as compared to females. Duration of the disease had a significant correlation with only three of the LV systolic functional parameters. Those with longer duration of disease had larger LVES dimension (r=0.517, p=0.01), larger LVED dimension (r=0.40, p=0.05) and lower FS (r=-0.506, p=0.01). The duration of disease had no correlation with any of the studied diastolic functional parameters. The patients were divided into three groups according to mode of presentation viz. polyarticular (Group 1), oligoarticular (Group 2) and systemic onset (Group 3). The mean age, weight, height, weight, systolic- and diastolic- blood pressure and LV systolic function parameters were comparable amongst the three groups. Analysis of diastolic functions revealed that patients with polyarticular type had higher peak E velocity (1.01±0.10 vs. 0.92±0.10 p=0.05) as compared to the systemic type, while there was no difference with Group 2 (0.98±0.11). Patients of Group 1 also had higher E VTI (13.49±1.80) in comparison to Group 2 (11.21±1.75, p=0.004) or Group 3 (11.36±1.70, p=0.01). Group 1 patients also had highest A VTI (7.27±0.97) as compared to Group 2 (6.20±0.61, p=0.004) or Group 3 (5.94±0.69, p<0.0001). Other diastolic parameters were comparable among the three groups. Comparison between the three groups by analysis of variance revealed that three diastolic parameters viz. E VTI (p 0.004), A VTI (p 0.001) and A dur/T dur (0.029) were discriminatory among them. None of the other diastolic or systolic parameters was significantly different among the three groups. DISCUSSION This study of the assessment of the systolic and diastolic functions in subjects with JRA who had no cardiac symptoms demonstrated that patients had significantly higher systolic and diastolic blood pressures as compared to controls. This could be related to NSAID intake (being taken by all patients), which can cause salt and water retention. Adult patients with RA are known to have a higher incidence of hypertension. Even though the absolute levels of blood pressure in our patients of JRA were within normal range, mean levels were higher as compared to controls. Such differences in childhood may lead to onset of overt hypertension as age advances. Since hypertension is an important cause of cardiac mortality in adults with RA, our finding of JRA patients having higher blood pressures as compared to controls, despite being in the normal range, assumes importance. Patients with JRA need close blood pressure monitoring so that early onset hypertensions can be detected and treated adequately. Although pathological studies have suggested a higher prevalence of pericarditis in patients with JRA, such a diagnosis on clinical grounds is relatively uncommon. We did not find pericardial effusion or pericardial thickening on echocardiography in any of the patients. This is in contrast to what has been reported by Bernstein et al[3] where pericardial effusion was noted in 37% cases with JRA. However, other studies[4],[7] have also reported absence of pericardial effusion in their series of juvenile arthritis. We found that patients with JRA had enlarged LV size and reduced systolic function parameters (lower EF and FS, though both were still within the normal range) as compared to controls. Our patients also had significantly higher resting heart rates as compared to controls, which could be related to the presence of inflammatory mediators in patients with JRA. Our observation of resting tachycardia, dilated LV and lower FS and EF in patients could also represent a sub-clinical myocarditis. Whether this progresses to clinical systolic dysfunction with time, can only be revealed by long-term follow-up studies. Hence, it is important to have baseline LV systolic function assessment in patients with JRA despite their asymptomatic status to see if LV dilatation or systolic function impairment exists. Our data demonstrating dilatation of LV in patients with JRA is consistent with data from previous studies done in adult patients with RA.[8],[9] In a study of 30 patients with JRA, Oguz et al[4] also reported higher LV systolic dimensions and lower EF as compared to controls. However, unlike our study, they did not find any significant differences in the resting heart rate or LV diastolic dimensions and volumes. We observed significant diastolic dysfunction in patients with JRA in the form of reduced peak E velocity, higher A velocity, lower E/A velocity ratio, higher A VTI and lower E/A VTI ratios. This pattern, which is a reversal of the normal pattern, possibly reflects the increased LV filling during late atrial systole as compared to the early passive filling phase. This reflects an alteration in LV compliance and impaired diastolic relaxation.[10] Corrao et al[9] in a study of adult patients with RA also reported higher trans-mitral A velocity and lower E/A ratios and postulated that these abnormalities may reflect LV structural alterations (increased interstitial connective tissue in the myocardium). Diastolic dysfunction has also been reported in other studies of adult patients with RA.[11],[12] In a study of HLA B27 associated juvenile arthritis, Huppertz et al[7] reported that LV diastolic function abnormalities are apparent only after exercise in the patient population. This is in contrast to our study where we noted diastolic dysfunction at rest in our patients with JRA. Decreased preload, elevated after-load, or impaired LV relaxation can all account for the abnormalities reported by us. The presence of dilated LV in our patients, however, makes reduction in preload to be an unlikely possibility. Higher blood pressure in our patients suggests that an increased after-load could be contributing to the diastolic dysfunction. Other factors like an increase in myocardial fibrosis, (due to enhanced interstitial connective tissue deposition) and higher resting heart rate (with consequent reduced time available for myocardial relaxation) could also play a role. We observed that those with longer duration of disease had larger LV end-systolic and diastolic diameters, and lower FS, suggesting that the abnormalities might progress over a period of time. Though there was no correlation of gender with LV systolic functional parameters, males with JRA had higher A VTI and IVRT as compared to females, reflecting perhaps a greater degree of diastolic dysfunction in male patients with JRA. Patients with a polyarticular mode of presentation had higher E VTI and A VTI as compared to other modes of presentation (viz. oligoarticular and systemic). To the best of our knowledge, no previous study has analysed the effect of these variables on LV systolic or diastolic parameters in JRA. However, since patient numbers are small, studies with larger number of patients are required to study these issues in more detail. The diastolic dysfunction observed by us is usually seen in disorders such as systemic hypertension, ischaemic heart disease and cardiomyopathy. Though our patients were young and asymptomatic, diastolic dysfunction was apparent. Such dysfunction might appear years before overt cardiac dysfunction becomes apparent. Hence, the study highlights the fact that patients with JRA need close monitoring. CONCLUSIONS Patients with JRA have significantly higher LV systolic and diastolic dimensions and volumes as compared to controls. Diastolic dysfunction is also common, in the form of lower transmitral E volicty, higher A velocity and prolonged IVRT. The presence of these despite an asymptomatic cardiac status highlights the importance of early diagnosis and detection of these abnormalities. REFERENCES
Copyright 2004 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp04090t2.jpg] [jp04090t1.jpg] |
| |||||||||

{kind=link}
{kind=link}