 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
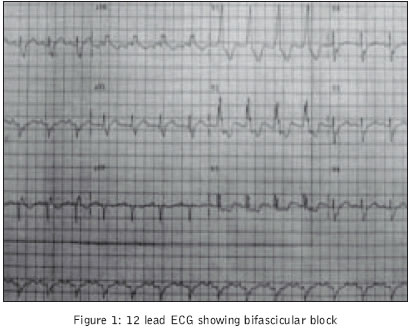
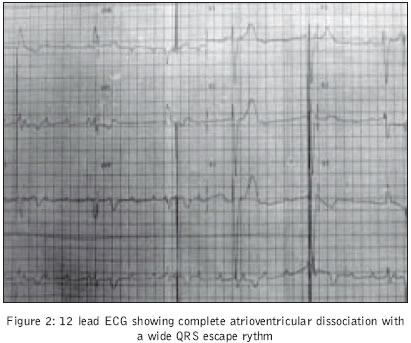
Journal of Postgraduate Medicine, Vol. 50, No. 4, October-December, 2004, pp. 291-292 Grand Round Case Recurrent syncopal attacks in a lady with rheumatoid arthritis Kubba Samir, Bali HK, Bahl A, Nand Kumar S Department of Cardiology, Postgraduate Institute of Medical Education and Research, Chandigarh Code Number: jp04101 A-48-year-old lady presented with a history of frequent syncopal attacks since 7 days. There was no history of seizure, headache, vomiting, breathlessness, chest pain, palpitations or vertigo. She was a non-diabetic, non-smoker, non-hypertensive and had no significant family history of coronary artery disease. She had a 16-year old history of seropositive rheumatoid arthritis (RA) with intermittent relapses. Initially, she was on diclofenac but for the last 4 years her therapy had been changed to chloroquine 500 mg/day and indomethacin 75 mg/day. She had never received steroids, methotrexate or other disease-modifying anti-rheumatoid drugs in the past. She had attained menopause 2 years back and was not on any hormone replacement therapy. At the time of presentation, she had symmetrical fixed joint deformities of the hands and feet and no clinical features to suggest active disease. Examination revealed heart rate of 40 beats per minute, supine blood pressure of 120/80 mmHg, intermittent cannon waves in the jugular venous pulse and pallor. Cardiovascular examination revealed mild cardiomegaly and a soft ejection systolic murmur grade 2/6 at the left sternal border. There was no hepatosplenomegaly. The chest was clear. She had with her a 4-day-old ECG [Figure - 1]. We repeated an ECG on her admission [Figure - 2]. What do the ECGs show? The first ECG shows left anterior hemiblock, right bundle block and a PR interval of 0.18 seconds. This is suggestive of bifascicular block. The second ECG shows complete atrioventricular dissociation with a broad QRS complex (QRS duration =0.14 seconds) ventricular escape rhythm of 48 per minute. What are the likely factors predisposing to heart block in patients with RA? Multiple factors can predispose to complete heart block in patients with RA.[1] These are: a. Rheumatoid nodule compressing the conduction tissue[2] What are the various cardiovascular manifestations of RA? The cardiovascular manifestations of RA include:[1] a. Pericardial disease-chronic asymptomatic effusive pericardial disease, acute pericarditis, pericardial calcification, constrictive pericarditis How would you investigate this patient? a. Complete haemogram with peripheral smear and ESR Since the patient was experiencing frequent syncopal attacks, a temporary pacemaker was inserted. Investigations revealed haemoglobin of 9g%, Total leuckocyte count of 5400/mm3 with 70% polymorphs 30% lymphocytes, ESR 16mm/1st hour, platelet count 2,00,000/mm3. Peripheral smear revealed a microcytic hypochromomic picture and the iron studies were consistent with iron deficiency anaemia. The renal functions, liver functions, serum electrolytes, urine examination, lipid profile and blood glucose were normal. Cardiac enzymes were not elevated at baseline and on serial follow-up. C-reactive protein was not elevated. Antinuclear antibodies were negative. The chest X-ray revealed mild cardiomegaly and the lung fields were clear. X-rays of the hand and foot revealed juxta-articular osteopenia. Echocardiography showed normal left ventricular systolic and diastolic function, without regional wall motion abnormality or pulmonary artery hypertension. Coronary angiography done to rule out coronary artery disease as the cause for the conduction block, revealed significant disease in the first diagonal branch of the left anterior descending artery which was a small vessel; other coronary arteries were normal. What could be the most likely cause for the complete heart block in this patient after the analysis of the above-mentioned investigations? Rheumatoid nodule compressing the conduction system, coronary arteritis and rheumatoid myocarditis are more often seen in patients with severe rheumatoid disease, often with extraarticular manifestations or high titers of rheumatoid factor.[6] However, the clinical profile, supplemented with the relevant investigations ruled out the presence of active disease in our patient. So these factors are unlikely to cause the conduction disturbance in this patient. Though coronary artery disease is more common in patients with RA our patient did not have coronary lesions severe enough to explain the conduction block. And although long-term chloroquine therapy causing complete heart block (CHB) has been described (due to the quinidine-like action of the drug), the absence of any other side-effect of chloroquine therapy such as myopathy, pigmentation or visual disturbance (fundus examination was normal in our patient) make chloroquine toxicity unlikely to be the cause for CHB in our patient. However, the possibility of chloroquine causing or contributing to the heart block cannot be completely ruled out. Secondary amyloidosis as the cause for the conduction disturbance was ruled out by relevant investigations. CHB can rarely occur in the well-controlled phase of the disease even in the absence of the above mentioned complicating factors.[7] As the disease typically has remissions and relapses, repeated episodes of inflammation interrupted by the quiescent phases of the disease can cause permanent damage to the conduction system leading to heart blocks.[7] This could have been the likely cause for CHB in our patient though other factors like long-term chloroquine therapy and CAD could have contributed as well. How would you manage this patient? As the disease is not in its active phase the focus should be on the conduction disturbance which is producing symptoms of cerebral ischaemia. Since conduction blocks once established in the disease do not respond to anti-inflammatory treatment,[1] the patient should undergo permanent pacemaker implantation. Our patient received a single chamber VVI permanent pacemaker implantation. She was also started on 10 mg leflunomide, a relatively new disease modifying anti-rheumatic drug. Though the drug may not benefit the permanent joint deformities it will decrease the relapses and the overall inflammatory milieu thereby reducing the progression of CAD and cerebrovascular disease. For the CAD, she was started on 150 mg aspirin, 20 mg atorvastatin and 25 mg bid metoprolol. She has been discharged and is symptom-free at 6 months of follow-up. REFERENCES
Copyright 2004 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp04101f1.jpg] [jp04101f2.jpg] |
| |||||||||

{kind=link}
{kind=link}