 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 51, No. 3, July-September, 2005, pp. 169-173 Original Article A study of sutopsy findings in 62 cases of leptospirosis in a metropolitan city in India Salkade HP, Divate S*, Deshpande JR, Kawishwar V, Chaturvedi R, Kandalkar BM, Vaideeswar P* Dept. of Pathology, Topiwala National Medical College
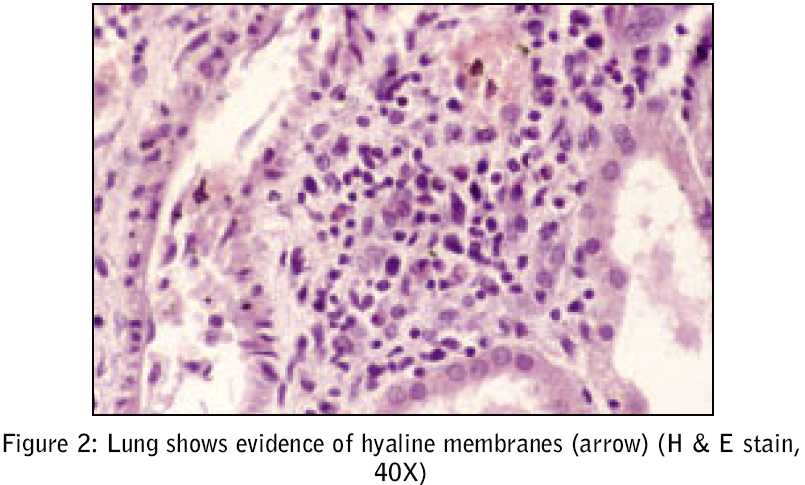
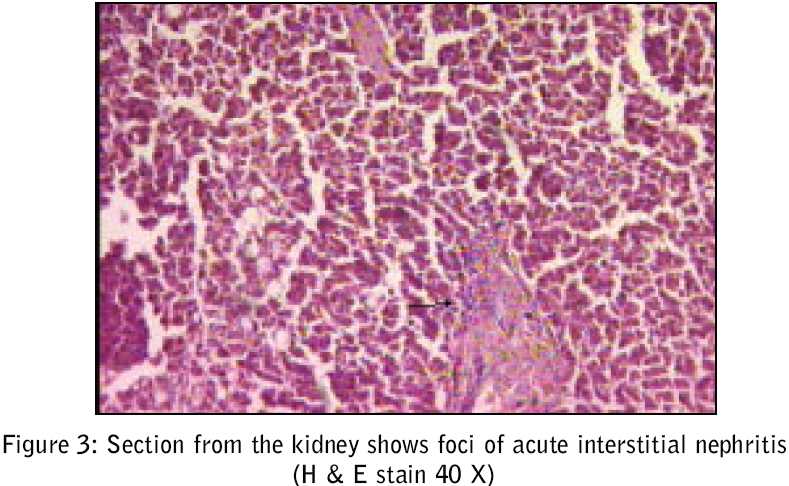
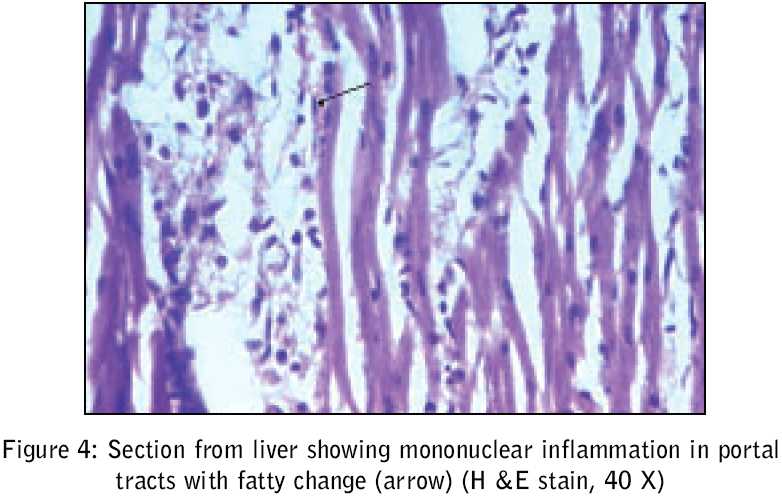
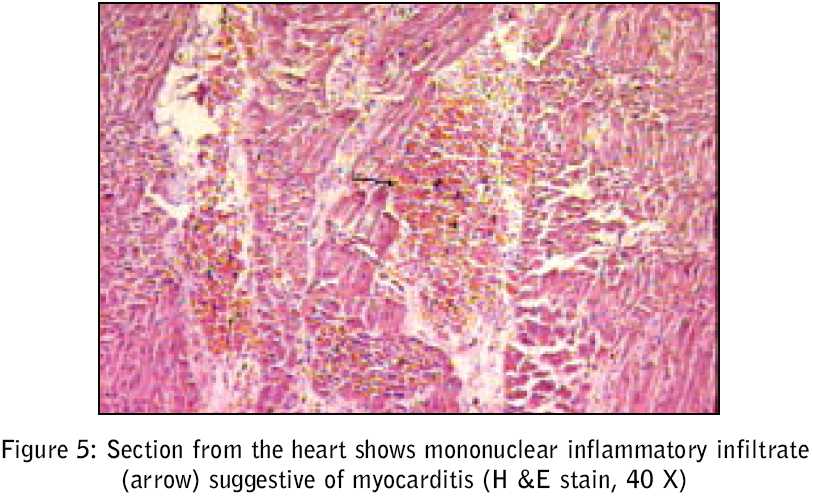
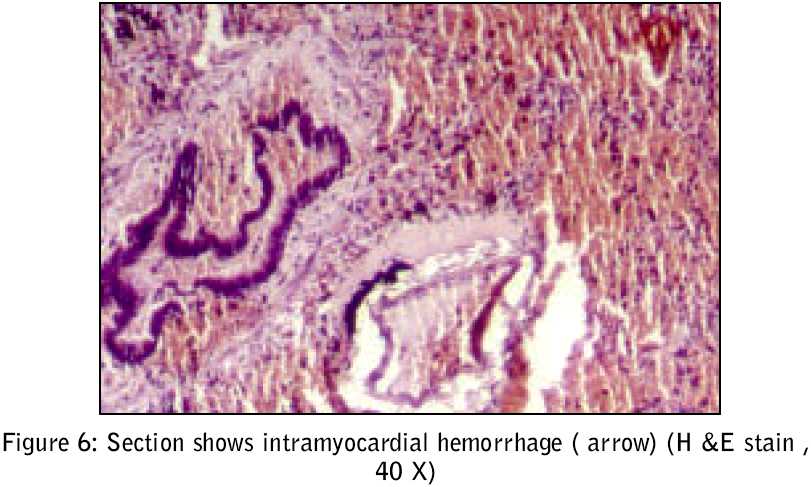
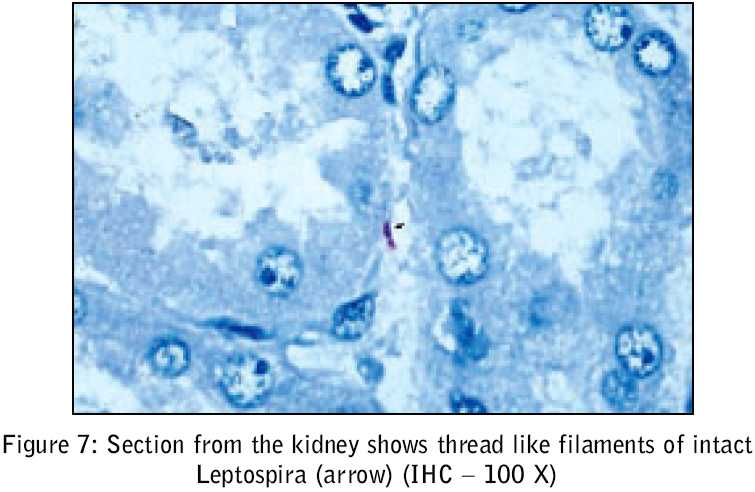
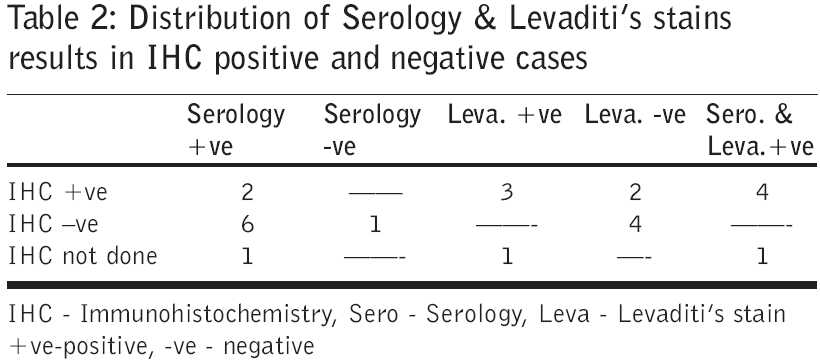
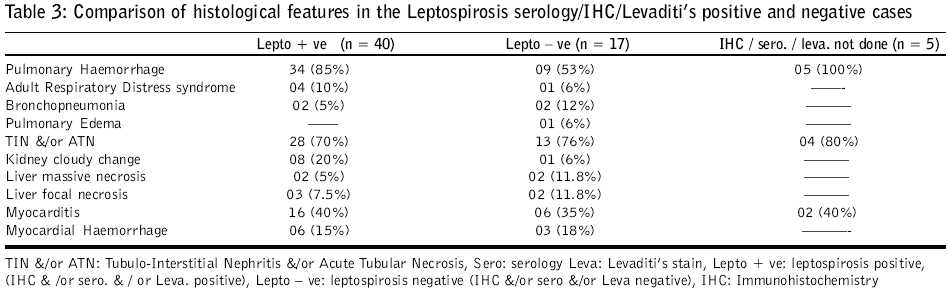
and B. Y. L. Nair Ch. Hospital, *Regional Office for Health and Family Welfare, Government of India, Kormangala, Bangalore-560034, India Code Number: jp05068 Abstract Background: Leptospirosis is an important sporadic zoonotic disease caused by the spirochete Leptospira icterohaemorrhagiae . The disease becomes a major public health problem, particularly during the monsoon months.Materials and Methods : Analysis of autopsy findings of 62 cases of clinically suspected leptospirosis was carried out to identify the pathology and determine the cause of death. Results : Most patients were young males who presented with fever, breathlessness, haemoptysis, bleeding, oliguria and icterus. They died after a brief stay in hospital. A post-mortem diagnosis of leptospirosis was made on the basis of characteristic organ findings, aided by results of serology, Levaditi's staining and / or immunohistochemistry (IHC) on kidney sections. Massive intra-alveolar haemorrhage (48 cases), acute interstitial nephritis and / or acute tubular necrosis (45 cases) and myocarditis (24 cases) were the main autopsy findings. Haemorrhage in various organs like the heart, gastrointestinal tract, brain, pancreas and adrenals were also seen. Thirty of 54 kidney sections were positive for leptospiral antigens by IHC. There was extensive haemorrhages in the lungs in 48 (77%) cases and that was the cause of death in most of these cases. Conclusion : Bleeding into various tissues and organs is the main finding noted in this study. The post-mortem examination of patients dying of leptospirosis revealed that pulmonary haemorrhage was the cause of death in most individuals. Keywords: Leptospirosis, Post-mortem histopathology, Acute respiratory distress syndrome, Acute renal failure, Pulmonary haemorrhage Leptospirosis is a globally important zoonotic disease and its transmission depends on interaction between humans and mammalian reservoir hosts.[1] It presents with fever, jaundice, azotaemia, haemorrhages, anaemia and altered consciousness.[2] Laboratory diagnosis of the disease is difficult and tedious and has been the main hurdle in confirming the clinical diagnosis and in describing the epidemiological study of this disease.[3] Although leptospirosis is known to occur in India for over a century, its incidence has increased over the last two decades and attained the proportions of a major health problem. It is interesting to note that the disease has been presenting as acute respiratory distress syndrome with haemorrhage not only in India[4] but in other countries, as well.[5],[6] This study was undertaken to determine the cause of death in 62 fatal cases of clinically diagnosed leptospirosis. The main objective of the study was to determine the final cause of death and to analyse the varying clinical presentations and autopsy findings including immunohistochemistry (IHC). Materials and Methods The post-mortem findings in 62 cases of clinically suspected leptospirosis from two tertiary medical institutions in Mumbai were retrospectively analysed. These cases were seen in a period of four weeks from July to August, 2000, following a spell of heavy rains and flooding. Other febrile illnesses like malaria, enteric fever and tuberculosis were excluded from the study. Available clinical history was studied and complete post-mortem examination was performed in each case. Detailed gross examination of all organs was carried out and representative sections from each organ were taken. Routine processing and staining were done. In 15 cases, kidney sections were stained with Levaditi′s stain for Leptospira .[7] In 54 cases, kidney sections were sent to Centers for Disease Control and Prevention (CDC), Atlanta for immunohistochemical (IHC) staining for leptospira. The IHC screening assays used a mixture of reference rabbit polyclonal antisera reactive with 16 leptospiral strains.[5] Serology was done in 15 cases by Lepto-dridot kit, a macroscopic agglutination test that detects IgG and IgM antibodies against leptospiral antigens. On the basis of serology and results of IHC and / or Levaditi′s staining, the cases were classified into three groups: those where these tests were positive (Group A), where these tests were negative (Group B) and where these tests were not done (Group C)Results Post-mortem examination was done in the 62 (50 males, 12 females) clinically suspected cases of leptospirosis, who died in July-August 2000. Their ages ranged from 9 to 75 years (mean: 32.9 +/- 13.9 years). Forty patients had a very brief stay in hospital and succumbed within 48 hours of admission. The clinical manifestations seen in 62 subjects are detailed in [Table - 1]. The striking feature at the autopsy was noted in the lungs which were dark red, plum-coloured on gross examination. Histologically extensive intra-alveolar haemorrhage was observed in 48 cases [Figure - 1]. Amongst these, 11 cases showed a few hyaline membranes. Five other cases showed extensive hyaline membranes indicative of a predominant acute respiratory distress syndrome [Figure - 2]. Four cases had bronchopneumonia and pulmonary edema was the only feature seen in one case. The kidneys were pale and swollen. Microscopic evidence of acute interstitial nephritis in the form of interstitial inflammatory infiltrate containing lymphocytes, macrophages, plasma cells and eosinophils, was seen in 45 cases [Figure - 3]. In addition, acute tubular necrosis, cloudy change of tubular epithelium and foci of haemorrhage were also seen. Portal triaditis in the liver [Figure - 4] was seen in 12 cases. Focal necrosis (5 cases), massive necrosis (4 cases), fatty change, and cholestasis were other hepatic abnormalities noted. Myocarditis with moderate lymphocytic infiltration and necrosis of myocyte was seen in 24 cases [Figure - 5]. These were also associated with intra-myocardial and epicardial haemorrhages [Figure - 6]. Coronary arteries were normal on gross appearance, and hence were not examined histologically. Haemorrhages were seen in various other organs such as gastro-intestinal tract, brain, pancreas and adrenals. In 30 cases, Leptospira could be identified as filamentous thread-like structures or as granular forms in the tubules or interstitium, in the kidney sections by IHC [Figure - 7]. In the remaining 24 cases, these organisms could not be demonstrated by IHC. Levaditi′s stain on sections of the kidneys showed numerous blackish, tiny curved rods resembling Leptospira in nine cases, while serology was positive for leptospirosis in 14 cases . Results of serology and Levaditi′s stain in IHC positive and IHC negative cases are outlined in [Table - 2]. A comparison of histological features of the cases in the three groups is given in [Table - 3]. Extensive haemorrhage in the lungs, tubulo-interstitial nephritis in the kidneys and myocarditis were seen in all three groups. Discussion In most instances, leptospirosis presents as a sporadic disease especially among occupational groups like conservancy and agricultural workers.[8] Such patients usually manifest as acute febrile illness with varying degrees of jaundice and renal dysfunction. However, the disease assumes epidemic proportions whenever there is excessive flooding due to natural calamities like cyclones. Since a carrier state exists in the animal population, the environment becomes conducive for disease transmission when there is flooding and this explains the outbreaks in India.[9] There have been sporadic episodes of leptospirosis in Mumbai, which are usually diagnosed on the basis of clinical criteria devised to differentiate leptospirosis from other acute febrile illnesses.[2] Following torrential rains and consequent flooding in the months of July and August 2000, the public hospitals reported an increasing incidence of haemorrhagic leptospirosis, with 62 fatalities in two institutions. All of them underwent autopsy. A striking feature in all the admissions was the preponderance of respiratory symptoms often accompanied by other features related to hepatorenal dysfunction and/or coagulation defects. Such a manifestation of leptospiral disease has been reported earlier,[10],[11],[12] even in the Andaman Islands.[4] Cases of febrile illness with acute respiratory distress and hemorrhagic manifestations have occurred in that region since 1988 and have been designated as Andaman haemorrhagic fever.[9] Under normal circumstances, the clinical presumption of leptospirosis is confirmed by demonstration of the organisms in fluids or serological tests at the appropriate stage of the disease.[1] In the current situation, apart from the severely morbid condition of the patients, diagnosis and therapy were hindered by lack of adequate measures to diagnose and tackle the outbreak. Hence, serological tests could not be carried out in all the cases. Besides, it was also important to rule out other common causes such as falciparum malaria. Most of the series reported have been clinical case studies confirmed on serology. [10],[11],[12] Only a few reports have had demonstration of antigen on tissues obtained as post-mortem biopsies or actual autopsies.[5],[13] To the best of our knowledge, this is the largest autopsy series to be reported. IHC demonstration was sought in kidney sections in 54 cases and was found positive in 30 (55.5%) cases. The remaining 24 cases (44.4%) negative for IHC had a similar clinical presentation and autopsy findings. Various technical and financial constraints prevailed that prevented the study of the lung, heart, coronary arteries and liver for the presence of leptospira on IHC. Levaditi′s stain, a laborious and time-consuming procedure was done in 15 cases. On post-mortem examination, striking gross and microscopic features were noted in the lungs, kidney and heart, with lesser changes in the liver. Lung and kidney involvement was seen in 87% of patients. Massive pulmonary haemorrhage, as seen in 77% of our cases, is a challenging clinical syndrome, often associated with poor prognosis. Such an involvement of the lungs has been reported in population studies in the range of 2% to 43%.[5],[11],[12] In one post-mortem analysis by Nicodemo et al, 75% of cases showed haemorrhagic pneumopathy with septal capillary lesions.[13] Nally et al, showed evidence of septal deposition of immunoglobulin and complement in a guinea pig model of severe pulmonary leptospirosis.[14] Acute tubulo-interstitial nephritis and / or acute tubular necrosis were observed in 72% of these cases. Such patients present with oliguria and acute renal failure.[15],[16] It is postulated that leptospiral infection may induce tubulo-interstitial nephritis through a toxic component in the outer membrane followed by expression of inflammatory genes.[15] Oliguria was noted as an independent risk factor for death.[16] Cardiac involvement was observed in 53% cases with myocarditis and/or myocardial haemorrhage. However, it was not clinically suspected in any of these cases. Similar cardiac lesions and even coronary arteritis and aortitis have been observed. [17],[18],[19],[20] Massive liver necrosis was noted only in four cases, though jaundice was observed in 25 cases. Sorabjee mentions the presence of cholestasis in patients who are deeply jaundiced and that elevated bilirubin levels result from hemolysis and diminished urinary bilirubin excretion due to renal failure.[21] Although no single serovar was implicated in various epidemics, serovar copenhageni was isolated in 87% of the cases in Brazil,[10] canicola in Nicaragua,[22] lai from Korea[12] and gryppotyphosa in the Andamans.[4] According to Vinetz et al [1], the importance of pulmonary haemorrhage as a lethal complication of leptospirosis is widely recognised. However, population-based studies indicate that there is a poor correlation between infecting leptospira strain and clinical expression of the disease. Genetic transformation of a leptospira species has now been reported, which may explain these varied presentations.[1] Massive pulmonary haemorrhage was the most prominent finding in this epidemic that came in the wake of heavy rains and flooding in Mumbai, India. It was seen in IHC-confirmed as well as IHC-negative cases and in those in whom IHC was not done. Some of IHC- negative cases were serologically positive for leptospirosis [Table - 2], suggesting that IHC negativity could be due to antigenic loss or improper fixation and storage of tissues or the presence of new/previously unrecognised serovars. These serovars as suggested by Trevejo et al are perhaps more likely to cause pulmonary hemorrhage.[22] Hence, in patients with acute febrile illness and severe respiratory symptoms, a diagnosis of leptospirosis should be promptly considered followed by early management. Besides, the presence of myocarditis, which will add to the cardiorespiratory embarrassment, needs to be looked for specifically during clinical evaluation of all cases of leptospirosis. Acknowledgement Shieh Wun-Ju-Pathologist / Medical Officer, Infectious disease pathology activity, DVRD / NCID / CDC Atlanta for doing IHC study on kidney sections for leptospira. Dr. Vinaya Shah, Assoc. Prof. at Nair Hospital for doing Levaditi′s stain on kidney sections.References
Copyright 2005 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp05068t1.jpg] [jp05068f7.jpg] [jp05068t2.jpg] [jp05068f5.jpg] [jp05068t3.jpg] [jp05068f3.jpg] [jp05068f6.jpg] [jp05068f2.jpg] [jp05068f4.jpg] [jp05068f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}