 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
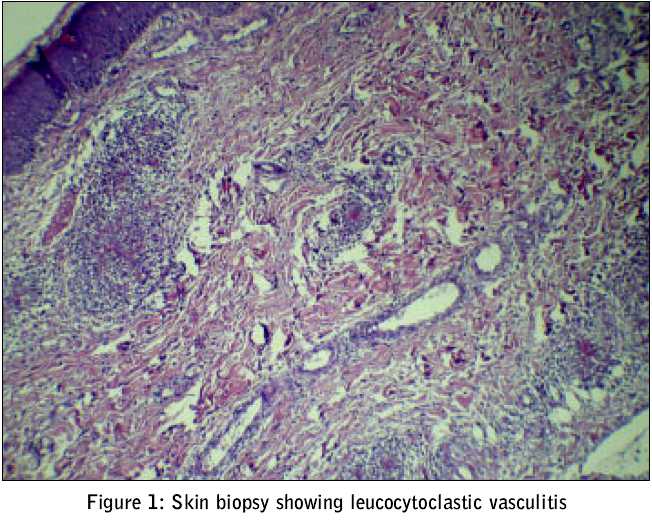
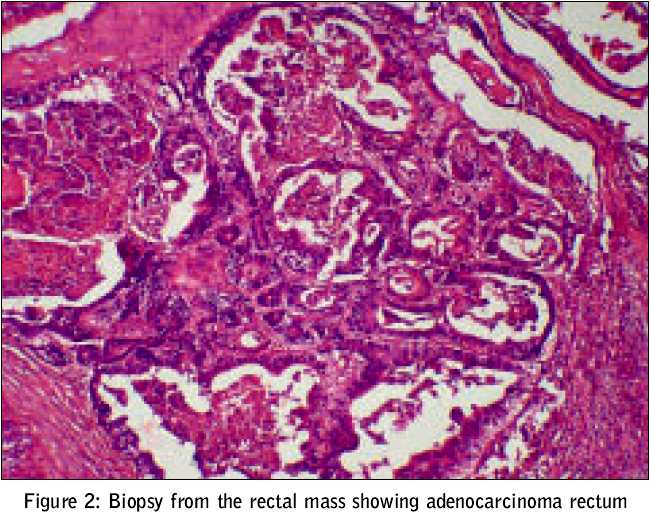
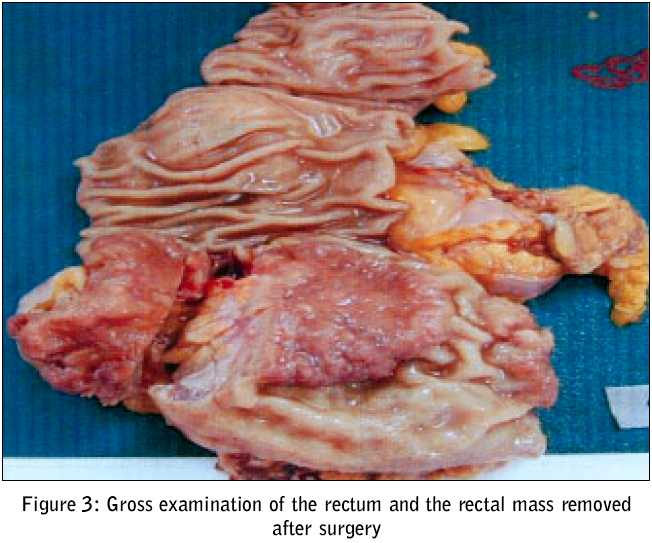
Journal of Postgraduate Medicine, Vol. 51, No. 3, July-September, 2005, pp. 215-217 Case Reports Leucocytoclastic vasculitis as a presentation of adenocarcinoma rectum Gogia A, Kakar A, Bhalla* S, Byotra SP Department of Medicine, and *Pathology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi-110 060 Code Number: jp05077 Abstract Vasculitis has been linked to several processes, like infections, drugs and allergic, rheumatologic and neoplastic diseases. Neoplasm-associated vasculitis described in the medical literature has mostly been reported in association with haemotological neoplasms. Adenocarcinoma of rectum presenting as leucocytoclastic vasculitis is rare. We present a case of a 43-year-old male with paraneoplastic leucocytoclastic vasculitis preceding the manifestation of adenocarcinoma rectum. The vasculitis subsided on resection of the rectal malignancy and the patient did not require steroid therapy thereafter.Keywords: Leucocytoclastic vasculitis, Adenocarcinoma rectum Vasculitis is characterized by inflammatory changes and necrosis of blood vessels. Vasculitis has been linked to several processes, like infections, drugs and allergic, rheumatologic and neoplastic diseases. The existence of malignancies in patients with vasculitis has been estimated to be about 4.5-8%.[1] Neoplasm-associated vasculitis described in the medical literature has mostly been reported in association with haemotological neoplasms.[2] Adenocarcinoma of rectum presenting, as leucocytoclastic vasculitis is rare. We describe a case, in which leucocytoclastic vasculitis (LCV) which preceded the presentation of adenocarcinoma of rectum. Case Report A 43-year-old male, presented with skin rash over legs, buttocks and lower abdomen of 6 days duration along with history of low-grade fever. There was no history of altered bowel and bladder habits nor was there any history of abdominal or joint pains. There was no history of bleeding from any site or any known allergies. There was no history of any new drug intake, insect bite or seafood consumption in the days preceding this rash. He had a past history of diabetes mellitus and chronic obstructive airway disease for last 6 years and was on oral Glibenclamide 5mg twice daily and bronchodilators. On admission, he was febrile and had a maculopapular rash over the lower limbs, buttocks and lower abdomen. Rest of the general and systemic examinations were unremarkable. Investigation revealed Haemoglobin 12.4 gm/dl, Total leucocyte count 5400/cumm, platelets 3.51 lakhs/cumm, and ESR 48 mm in first hour. Urine examination showed protein +, RBCs 8-10/hpf. Random blood sugar was 144 mg/dl. Ultrasound abdomen was normal. Skin biopsy showed leucocytoclastic vasculitis [Figure - 1] and the patient was begun on oral steroids (40 mg/day). He responded to the treatment initially but the rash recurred after a week′s therapy. The dose of steroids was increased to 60 mg/day. The patient was then lost to follow up. He was readmitted after 7 months; he was on a tapering dose of steroids. The skin rash was there and along with it, he also had blood in the stools, which was dark red and appeared on straining. There was history of loss of weight (7 kgs) over the last 7-8 months. He had no history of fever, upper gastrointestinal bleed or joint pains. He was pale and had a maculopapular rash on the lower limbs and abdomen. Per rectal examination revealed an ulcerative growth (3 cm x 3 cm) 6 cm from the anal verge; there was no bleeding or discharge. On investigations, at this time, his haemoglobin was 10.2 gm/dl, Total leucocyte count of 4700/cumm, platelets 2.51 lakhs, ESR 82 mm in first hour. Random blood sugar was 269 mg/dl. Routine examination of urine showed protein + with RBCs 8-9/hpf. 24 hour urinary protein excretion was 870 mg. Examination of the stools showed RBC +++, no bacteria. Blood Urea Nitrogen was 10.2 mg/dl, Serum Creatinine was 1.9 mg/dl and Creatinine Clearance was 64 ml/min. His liver function tests were normal. Colonoscopy showed the growth as described above, at 6 cm from the anal verge and multiple punch biopsies were taken. Histopathological examination showed adenocarcinoma of rectum [Figure - 2]. CT scan of the abdomen showed localized growth on the posterior aspect of the rectal wall. No lymph nodes were seen. Laparoscopic low anterior resection [Figure - 3] and cavero-ileostomy was done . At 6 months of follow up, the patient was stable, there was no skin rash and he was not requiring any steroids.Discussion Paraneoplastic syndromes may sometimes herald the presence of the tumour and therefore, have important diagnostic implications. The vasculitides may be among the paraneoplastic syndromes; they may either appear after the malignancy, antedate the discovery of the neoplasm or give a clue to a recurrence.[3] Leucocytoclastic vasculitis is a part of the systemic disorder which often has been linked pathogenetically to circulating immune complexes. LCV has only rarely been the initial sign of any malignancy.[4] In most of the reports of vasculitis, the neoplasms have been lymphoproliferative; most frequently hairy-cell leukemia.[2] Only rarely has the presence of the cutaneous disease led to the discovery of an underlying malignancy. The first case of vasculitis in a patient with a solid tumor (i.e. Renal cell carcinoma) was reported by Torrrik and Berntzen in 1968.[2] Since this initial case report, an additional 35 cases of solid tumors have been reported in the world literature. When a vasculitis is associated with a solid tumor it is usually a small vessel vasculitis, predominantly both cutaneous and leucocytoclastic as was in our patient.[5] The most frequently seen non-haematologic neoplasms in patients with vasculitis are lung (small and non-small cell), prostate (adenocarcinoma), colon (adenocarcinoma), renal (renal cell carcinoma), breast (ductal carcinoma), head and neck (epidermoid carcinoma) and endometrial cancer.[2],[3] LCV is the most frequently encountered type of cutaneous vasculitis in general and in association with malignancies. The body parts most frequently affected are the lower extremities, similar to our case. Involvement of the mucous membranes, head and neck, trunk and upper extremities may also occur. Systemic manifestations like fever, arthralgias, as well as pulmonary and gastrointestinal compromise may occur. The other forms of vasculitis that may be paraneoplastic in origin include granulomatous changes, nerve and muscle microvasculitis, lymphocytic vascular changes, Henoch-Schonlein, Churg-Strauss, Polyarteritis nodosa; lymphomatoid, necrotizing and temporal arteritic forms are also described in association with neoplasms.[2],[3] Laboratory tests which may be abnormal include an elevated ESR, circulating immune complexes, positive antinuclear antibodies, rheumatoid arthritis factor and depressed total haemolytic complement. The elevation of ESR is the most common finding in most of the series on LCV. The frequency of rheumatoid factor in the majority of studies was 16-18%. Pathological urinary findings have been seen in 35% and 42% in the Mayo Clinic study and Mackel and Jordon study respectively.[6] Histological features of LCV include leucocytoclasis, neutrophils in the vessel wall, fibrinoid necrosis and extravasation of red blood cells.[3] Paraneoplastic vasculitides do not necessarily have a bad prognosis. In majority of the cases death is due to metastasis or recurrent tumour rather than to vasculitic complications.[3] Patient with unexplainable vasculitis should always be examined for the possibility of the vasculitis being paraneoplastic, particularly since the vasculitis may long antedate any evidence of tumor as was in our case. References
Copyright 2005 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp05077f1.jpg] [jp05077f2.jpg] [jp05077f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}