 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
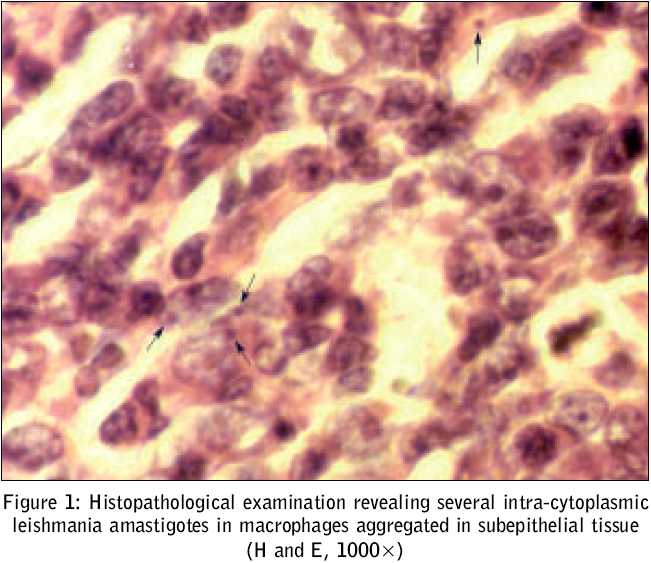
Journal of Postgraduate Medicine, Vol. 51, No. 3, July-September, 2005, pp. 218-219 Case Reports Isolated lingual leishmaniasis Habibzadeh F, Sajedianfard J*, Yadollahie M NIOC Medical Education and Research Center, *Department of Physicology, Faculty of Veterinary Medicine, Shiraz University, Shiraz, Iran Code Number: jp05078 Abstract Cutaneous leishmaniasis is endemic in Fars Province, southern Iran. However, mucosal leishmaniasis is extremely uncommon. Herein, we report a patient with isolated lingual leishmaniasis in an immunocompetent 40-year-old man. The lesion was totally excised. The patient was cured completely and is doing well after four years of follow-up, with no medical treatmentKeywords: Leishmania tropica - Leishmania major - Leishmaniasis, Mucocutaneous - Tongue - Tongue diseases - Iran Leishmaniasis is a zoonotic disease caused by Leishmania spp. Currently, it is a major global health problem, which is increasing in incidence.[1] Transmission of the disease occurs through the bite of a female sandfly infected with Leishmania parasites. Depending on complex host-parasite interactions, the clinical picture of leishmaniasis varies from a simple ulcer to a fatal systemic disease. Leishmaniasis may manifest itself in cutaneous, mucocutaneous, or visceral forms.[2] Cutaneous leishmaniasis is the most common form of the disease in Iran. There are also foci of visceral leishmaniasis. Nevertheless, reports of mucosal leishmaniasis from this region are scarce.[3] Herein, we report a very rare case of isolated lingual leishmaniasis in an immunocompetent man. Case History A 40-year-old male from Marvdasht, Fars Province, Southern Iran, presented with a lesion on his tongue that he had noted since three months. On physical examination, he was a well-developed, well-nourished man with no history of any systemic disease, or any associated mucocutaneous lesions. The patient had not travelled abroad. He had no prodromal signs or symptoms, nor hepatosplenomegaly. On inspection, there was a fleshy mass measuring 5 x 7 x 5 mm, on the right side of his tongue, just against the first lower molar tooth. On investigation, his complete blood count was normal. To determine the nature of the disease, the mass was totally excised. Histopathological examination revealed several intra-cytoplasmic leishmania amastigotes in macrophages aggregated in subepithelial tissue [Figure - 1]. Indirect immunofluorescence was negative for specific antibodies. No bone marrow aspiration, culture for the parasite, isoenzyme study or polymerase chain reaction test for diagnosis of the parasite was performed. The patient did not receive any anti-leishmanial medication and was cured spontaneously. After four years of follow-up, the patient has no sign or symptom of the disease by way of residual disease or recurrence.Discussion In 1903, Leishman and Donovan independently described the protozoan, now called Leishmania donovani in the splenic tissue from patients in India. The disease is called visceral leishmaniasis.[4] The term, ′leishmaniasis′covers a series of illnesses caused by the protozoan parasite, Leishmania spp . The disease is geographically and ecologically widespread, occurring in tropical and subtropical regions in all continents with the exception of Australia.[5] Depending on the patient′s immune response, and the particular species of the protozoan, leishmaniasis may manifest itself in cutaneous, mucocutaneous or visceral forms.[2] Cutaneous leishmaniasis presents as a skin ulcer and generally heals spontaneously within three to six months.[5] Mucocutaneous leishmaniasis (espundia) is a grave disease that is limited to the skin and mucous membranes. The chancrous sores heal after a time, but sometimes months or years later, fungating and eroding forms of ulceration may appear on the tongue and buccal or nasal mucosa. Visceral leishmaniasis presents with fever, weight loss, hepatosplenomegaly, and anaemia. It is always fatal if left untreated.[5] With the spread of the human immunodeficiency virus (HIV), visceral leishmaniasis has become increasingly prevalent and unusual presentations often occur. Mucosal leishmaniasis cases occur rarely in the Mediterranean area. The most common causes of leishmaniasis in Iran are L. tropica and L. major .[6],[7] In Fars Province, L. tropica is responsible for most of the cases of the anthroponotic form of the disease with dry lesions occurring frequently in urban areas, and L. major causes the zoonotic form with wet lesions, mostly occurring in rural areas.[8] Kala-azar is seen occasionally in Fars province. However, it is more common in the southern provinces. Mucocutaneous leishmaniasis is extremely rare in Iran.[3] The case of isolated lingual leishmaniasis in immunocompetent individuals is extremely rare. The two reported cases were transplant recipients, one with a kidney and another with a heart transplant.[9],[10] Cases of lingual leishmaniasis have also been reported in HIV-infected patients.[2],[11] Our patient, who came from an endemic area for leishmaniasis, had no sign of any immune system dysfunction, nor any history of previous infection. So far, only two cases of lingual leishmaniasis have been reported in immunocompetent persons.[12],[13] However, our patient differed from the two aforementioned cases, in the fact that he was diagnosed at an early stage of the disease, as was evident from the small-sized isolated lesion and that he had a spontaneous cure with no medical treatment. On account of the epidemiology of leishmaniasis in the region, we have to think about either L. tropica or L. major as the cause of the disease in our patient. Nevertheless, observation of local involvement of lingual mucosa by either L. tropica or L. major raises a question as to whether the lesion described represents the primary site of the parasite inoculation or is caused by the migration of the parasite from elsewhere. Absence of a systemic immune response, a localised clinical presentation and the fact that the patient developed a spontaneous cure with no recurrence after four years of follow-up, are all strongly in favour of the former hypothesis. References
Copyright 2005 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp05078f1.jpg] |
| |||||||||

{kind=link}