 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 51, No. 3, July-September, 2005, pp. 225-227 CPC Congestive cardiac failure and anemia in a 15-year-old boy Shenoy VV, Patil PV, Nagar VS, Deshpande AK, Shedge RT*, Badiye AP**, Saigaonkar R** Departments of Medicine,*Pathology, and **
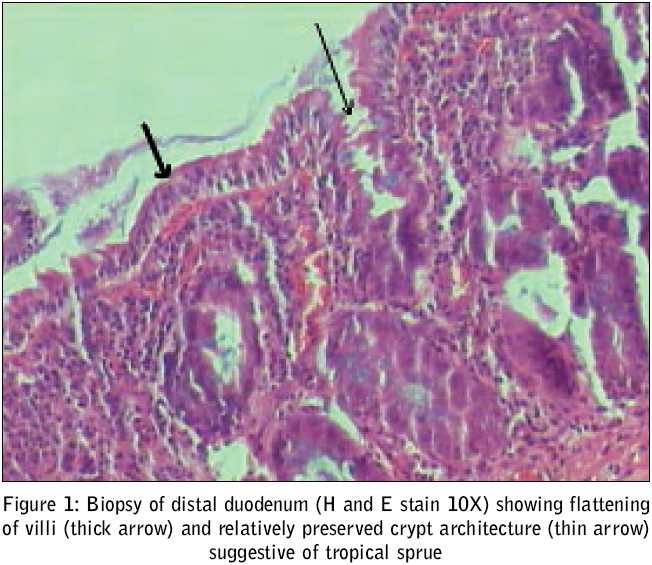
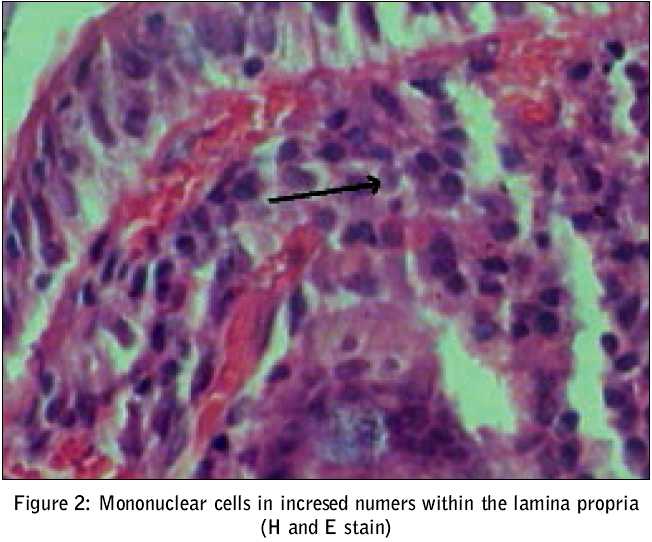
Gastroenterology,Grant Medical College & Sir J. J. Group of Hospitals, Mumbai 400008 Code Number: jp05081 A 15-year-old boy was referred to us with bilateral edema feet for the past four weeks. The edema had progressively increased to involve the thighs and was followed by facial puffiness. This was preceded by a history of easy fatigability, decreased appetite, and mild exertional dyspnea. It was not associated with orthopnea, paroxysmal nocturnal dyspnea, fever or any history suggestive of rheumatic fever. There was no history of blood loss from any site nor any bladder and bowel disturbances. There was no history of any major illness in the past. His primary care physician treated him symptomatically with loop diuretics without any benefit. In fact this had resulted in hypokalemia twice, for which the patient was referred to our institute. On general examination, he had a pulse rate of 120 beats/min and blood pressure of 120/60 mm Hg. There was pallor and pitting edema up to the tibial shins. The jugular venous pressure column was three centimeters above the sternal angle in the 45° reclining position. The lower border of the liver was palpable three centimeters below the costal margin with a liver span of 18 cm suggesting a mild hepatomegaly. Cardiac examination revealed an S3 gallop and a soft systolic murmur of grade II intensity. There were no sensory motor deficits, but bilateral ankle reflexes were absent. A clinical diagnosis of high output congestive heart failure, possibly due to anemia was considered. On investigation, a complete blood count was suggestive of anemia [Table - 1]. The red cell indices revealed an increase in the mean corpuscular volume (MCV) and the peripheral smear showed macrocytosis with anisocytosis and poikilocytosis. All biochemical parameters including thyroid function tests were normal. Investigations carried out for the diagnosis of megaloblastic anemia revealed normal vitamin B12 level, but the serum folate level was low. The chest radiograph suggested cardiomegaly (cardio-thoracic ratio > 0.5) and ECG had T wave inversion in anterior leads. A 2D Echo revealed global hypokinesia with dilated chambers, and the ejection fraction (EF) was 40%. Mild tricuspid regurgitation and minimal pericardial effusion were also detected. Signs of hyperdynamic circulation with low ejection fraction in the absence of severe anemia or hyperthyroidism suggested the presence of reversible cardiomyopathy. In view of depressed tendon jerks, a possibility of thiamine deficiency was considered. Therefore a therapeutic trial of 50 mg of intravenous thiamine daily was given for one week followed by oral therapy of 25 mg per day thereafter. Loop diuretics were stopped. The signs of heart failure disappeared rapidly and the ejection fraction improved to 55% within two weeks. Due to absence of obvious dietary deficiency or predisposing factors for beriberi, and repeated stool examinations being normal, an upper GI endoscopy with biopsy from the farthest point of the second part of the duodenum was carried out. Clinical Discussion One of the causes of high output heart failure is wet beriberi due to thiamine deficiency. [1] However, this diagnosis is often not suspected as a cause of high output heart failure at the bedside, due to the rarity of its classical manifestations and the free empirical use of vitamin B complex. Beriberi results from deficiency of thiamine (vitamin B1), an essential cofactor for the decarboxylating enzymes of carbohydrate metabolism and myelin synthesis. Predominant cardiovascular symptoms (wet beriberi), occur in patients with adequate calorie intake and increased physical activity. [2] Dry beriberi which presents with neurological manifestations: diminished tendon jerks, paresthesiae and large fiber sensory neuropathy. This patient presented with signs of hyperdynamic circulation fulfilling all the clinical criteria of wet beriberi mentioned in [Table - 2].[3] The best way to confirm beriberi would have been to demonstrate a decrease in erythrocyte transketolase level, which is known to correlate well with thiamine deficiency even in asymptomatic patients or those with non-specific symptoms. [4] However a subsequent increase in thiamine pyrophosphate (TPP) activity after addition of TPP by at least 15% is more specific to the diagnosis.[3] These, however, could not be done due to constraints in laboratory facilities. Diuretics are known to result in increased urinary excretion of thiamine and hence they were stopped.[1] A therapeutic trial, which is the best test in suspected thiamine deficiency,[2] was given and the improvement proved it to be a case of thiamine deficiency beyond doubt. Since this patient had an adequate diet with unpolished rice as an important constituent and no signs of parasitic infection, a possibility of malabsorption was considered. Pathological Findings Sections through the small bowel biopsy revealed a moderate degree of shortening and flattening of villi [Figure - 1] thick arrow, but preserved villous and crypt architecture [Figure - 1] thin arrow with infiltration in the intraepithelial region and the lamina propria by increased number of mononuclear cells, predominantly lymphocytes [Figure - 2]. Plasma cells were also seen. There was lymphoid hyperplasia in the lamina propria and submucosa. As this suggested a diagnosis of tropical sprue, the patient was started on cotrimoxazole and folate supplements for 6 months resulting in correction of his anemia. He remains asymptomatic till date. Pathological Differential Diagnosis The normal small intestinal histology shows a ratio of villous to crypt length of 3:1 to 5:1, with occasional inflammatory cells in the lamina propria and intraepithelial lymphocytes in the ratio of one lymphocyte per five enterocytes.[5] The above histological appearance was most suggestive of tropical sprue. [6] A close differential is celiac sprue, which shows an increased mononuclear infiltrate and severe or total villous atrophy with a flat mucosa in most cases.[7] Other lesions with histological picture similar to tropical sprue i.e. nonspecific variable villous atrophy without flattening of mucosa, include: Dermatitis Herpetiformis which is associated with skin lesions;[8] infectious gastroenteritis, which shows non-specific variable villous atrophy but with acute inflammatory infiltrate;[9] and autoimmune enteropathy which affects infants presenting clinically with intractable watery diarrhea.[10] In the clinical scenario of a young boy with beriberi, tropical sprue was the most likely histopathological correlate. Clinico-pathological Correlation Tropical sprue is one of the commonest causes of malabsorption in tropical countries like India.[11] It most commonly presents with chronic diarrhea or rarely as nutrient deficiency, usually a megaloblastic anemia due to folate deficiency or occasionally also with vitamin B12 deficiency.[12] The etiology of tropical sprue remains obscure, though the role of bacterial infection in initiating or sustaining the process has been hypothesized[1],[12] The closest clinical and histo-pathological differential to tropical sprue is celiac disease, which is identified on the basis of severity of villous atrophy and response to a gluten free diet.[13] Thiamine is predominantly absorbed in the proximal bowel via human Thiamine Transporters 1 & 2 (hTHTR 1 & 2).[14] In addition to poor diet, chronic illness, alcoholism, and diseases like celiac disease and tropical sprue can also cause thiamine deficiency leading to beriberi.[1] Interestingly the folate and thiamine transporter channels share a 40% homology. Although the folate transporter channels cannot transport thiamine, [14],[15] they have a high affinity for the phosphorylated form of thiamine (thiamine pyrophosphate -TPP) and cause active efflux of thiamine from the cell. [15] Thus folate is essential to maintain the intracellular active form of thiamine (TPP). Folate deficiency increases the folate absorbing transporters on the cell membrane, resulting in efflux of TPP, and consequent intracellular thiamine depletion. The response to folates and antibiotics over a period of six months also supports tropical sprue as the cause of megaloblastic anemia and beriberi in this patient. [12] To conclude, malabsorption due to tropical sprue, secondary folate deficiency resulting in intracellular thiamine depletion and hasty diuretic use increasing thiamine excretion, all contributed to thiamine deficiency and wet beriberi. References
Copyright 2005 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp05081f1.jpg] [jp05081t1.jpg] [jp05081t2.jpg] [jp05081f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}