
|
Journal of Postgraduate Medicine
Medknow Publications and Staff Society of Seth GS Medical College and KEM Hospital, Mumbai, India
ISSN: 0022-3859 EISSN: 0972-2823
Vol. 51, Num. 3, 2005, pp. 234-235
|
Journal of Postgraduate Medicine, Vol. 51, No. 3, July-September, 2005, pp. 234-235
Grand Round Case
A man with recurrent abdominal pain and hypotension
Mathew J, Menon PS, Shah NS, Supe AN*
Department of Endocrinology and *Surgery, Seth G. S. Medical College
and K. E. M. Hospital, Parel, Mumbai-400012
Correspondence Address:Department of Endocrinology Seth G. S. Medical
College and K. E. M. Hospital, Parel, Mumbai-400012 ,nalinishah@gsmc.edu
Code Number: jp05085
A thirty-year-old gentleman presented with worsening right hypochondrial pain followed by vomiting of three days duration. On examination, he was afebrile, had a pulse rate of 120/ minute and blood pressure of 80/60 mm Hg. He was pale, sweating and had diffuse tenderness in the right hypochondrial region. Bowel sounds were normal. Cardiovascular and respiratory systems were normal.
What are the possible causes of this presentation?
The presentation of abdominal pain and hypotension is usually
suggestive of vascular process, septic process or perforation of a hollow
viscus. Vascular processes can involve a leaking abdominal aortic aneurysm,
splenic artery aneurysm rupture, splenic rupture, haemorrhage into a tumour
and acute mesenteric ischemia. Septic processes include toxic shock syndrome,
recurrent pyogenic cholangitis and intraabdominal abscess. Miscellaneous
causes include acute pancreatitis, acute adrenal crisis, diabetic ketoacidosis
and ruptured tubal pregnancy in women.
Investigation results were as follows: Haemoglobin: 10.2 gm/dL (11.0
- 14.5); white cell count: 17,700/mm 3sub (4000-11,000),
Neutrophils: 76 %, Lymphocytes: 34%. Platelets: 1,20,000/mm 3sub
(1,30,000 - 4,00,000) Electrolytes, calcium parameters and blood sugars
were normal. The chest x-ray failed to show any gas under the diaphragm.
The central venous pressure was low and he was resuscitated with intravenous
fluids. An ultrasonography of the abdomen showed a right adrenal mass with
central necrosis. During fluid resuscitation, the patient experienced hypertension
and palpitations (BP: 160/100 mm Hg, pulse rate: 140/minute).
How will you investigate the adrenal mass further?
The investigation of an adrenal mass involves establishing its functional
status and anatomical extent. For establishing its functional status, the
following tests can be done: 24-hour urinary metanephrines, vanylly (check
spelling)mandelic acid (VMA) and cortisol, overnight dexamethasone suppression
cortisol, serum potassium and an aldosterone /plasma renin activity ratio.
Imaging should be done with contrast enhanced CT scan or MRI to know the
size and density of the mass, a critical step that decides whether the
mass is benign or malignant. [1]
In view of normal electrolytes and absence of any obvious features of hypercortisolism,
we did a 24 urine VMA and metanephrine as the first investigation. Twenty-four
hour urine VMA was 79 mg/day (Normal levels: 1-7 mg/day) and 24 hour urinary
metanephrines was 1.85 mg /day (Normal level: less than 1.1 mg/day). CT
scan showed a right adrenal neoplasm of 32 HU density with a size of 5.5
x 5 x 4.5cm and central necrosis.
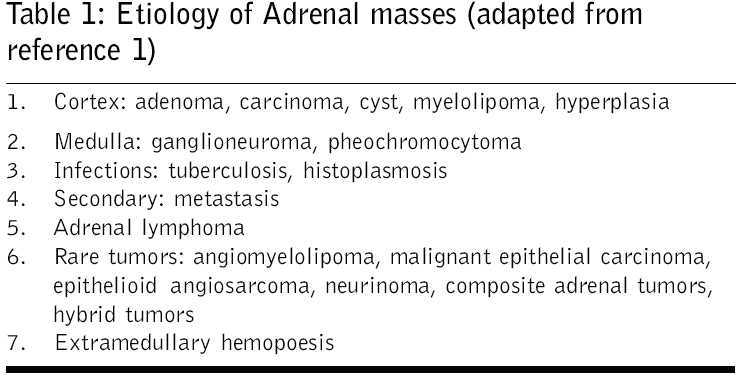
Significantly elevated levels of urinary metanephrines and vanylly
mandelic acid (VMA) in the absence of any interfering drugs in the presence
of an
adrenal mass is diagnostic of pheochromocytoma. The other common causes
of adrenal mass are shown in [Table -
1].
How can this patient be managed further?
The diagnosis can be confirmed with an MIBG (iodine-131-meta-iodobenzylguanidine)
scintiscan. Patients being prepared for surgery are started on α blockers.
After adequate a blockade for 10 -14 days, a beta-blocker is added.
The patients are hydrated with adequate salt and fluid for volume expansion.
The patient was started on Doxasozin which was titrated to 8 mg/day
over 14 days and was then given Propranolol 60 mg daily. The patient
was discharged
due to technical reasons and was given instructions to get admitted for
surgery He was lost to follow-up until he returned to us one year later
with paroxysms of vomiting, palpitation and hypertension. He was reinstated
on a blocker? Doxazosin, dose? The next day, he developed a paroxysm
of hypertension (BP: 180/120 mm Hg) associated with severe abdominal pain,
palpitation and sweating. The patient collapsed when he stood up, following
which he developed altered sensorium and laboured breathing. His blood
pressure was unrecordable and had a heart rate of 160 /minute. He was intubated
and resuscitated with intravenous fluids and was started on dopamine support.
Within 30 minutes, his blood pressure was recordable and he improved in
his sensorium. He was pale, and had tenderness and guarding in the right
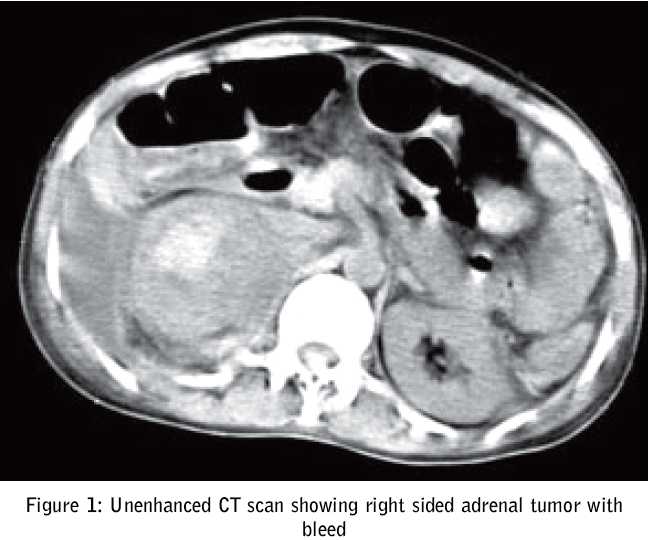
lumbar and hypochondrial region. An unenhanced CT scan of the abdomen was
taken. [Figure - 1]
What does the CT scan show?
The CT scan shows a right adrenal mass with an area of hemorrhage. Hemorrhage
into a pheochromocytoma can present with severe hypertension followed by
hypotension. The reason for the shock is related to sudden release of epinephrine
from the pheochromocytomas due to ischemia to normal adrenal tissue or
due to arterial and venous dilatation due to sudden withdrawal of catecholamines. [2], [3], [4]
What are the other possible causes of hypotension in a patient with pheochromocytoma?
Epinephrine secreting pheochromocytomas can present with cardiogenic shock.
Chronic elevation of epinephrine levels causes a compensatory downregulation
of β receptors of the heart, which decreases cardiac contractility.
Hypocalcaemia, due to calcium sequestration by pheochromocytoma or deposition
in bone is proposed as the second mechanism by which epinephrine-secreting
pheochromocytomas reduce cardiac contractility. Adrenomedullin, a hypotensive
peptide secreted by pheochromocytoma may be another culprit. [5]
Dopamine secreting pheochromocytomas can paradoxically have normal blood
pressure, which increases on removing the pheochromocytoma. It is due to
vasodilatation caused by stimulation of postsynaptic D1 like receptors
or presynaptic D2 receptors. [6] Catecholamine
cardiomyopathy is another cause of impaired myocardial function in these
patients. [7], [8], [9]
What are the drugs that can precipitate hypotension in pheochromocytomas?
Nifedipine can precipitate hypotension in patients with pheochromocytoma.
The possible causes described were hypovolemia and negative inotropism. [10] Dexamethasone
induced cardiogenic shock in a patient with pheochromocytoma was described
by Takagi et al. The potential mechanisms proposed are glucocorticoid stimulation
of phenylethanolamine-N-methyl-transferase, which converts norepinephrine
to epinephrine and steroid augmented sensitivity of cardiomyocytes to catecholamines. [8] Cardiogenic
shock triggered by phenothiazines, α blockers and β blockers has been
reported in literature. [8]
The temporal relation of events is suggestive of adrenal bleed as a
cause of this presentation and was confirmed by imaging. The rapid recovery
of
shock in our patient is suggestive of "myocardial stunning" due to diffuse
coronary vasospasm due to catecholamine crisis. [4]
After adequate α and β blockade, he underwent a right adrenalectomy
through intraperitoneal route. It was a 6 x 5 x 6 cm tumor with cut section
showing clotted blood. Histopathology was classical of pheochromocytoma
with large areas of hemorrhage and necrosis. Patient follow up subsequently?
References
| 1. | Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev 2004;25:309-40. Back to cited text no. 1 |
| 2. | Jacobs LM, Williams LF, Hinrichs HR. Hemorrhage into a pheochromocytoma. JAMA 1978;239:1156. Back to cited text no. 2 |
| 3. | Mishra AK, Agarwal G, Agarwal A, Mishra SK. Cystic phaeochromocytoma presenting as an acute abdomen with shock. Eur J Surg 2001;167:863-5. Back to cited text no. 3 |
| 4. | Mohamed HA, Aldakar MO, Habib N. Cardiogenic shock due to acute hemorrhagic necrosis of a pheochromocytoma: a case report and review of the literature. Can J Cardiol 2003;19:573-6. Back to cited text no. 4 |
| 5. | Olson SW, Deal LE, Piesman M. Epinephrine-secreting pheochromocytoma presenting with cardiogenic shock and profound hypocalcaemia. Ann Intern Med 2004;140:849-51. Back to cited text no. 5 |
| 6. | Yasunari K, Kohno M, Yoshikawa J. A dopamine-secreting pheochromocytoma. Am J Med 1999;106:599-600. Back to cited text no. 6 |
| 7. | De Wilde D, Velkeniers B, Huyghens L, Diltoer M. The paradox of hypotension and pheochromocytoma: a case report. Eur J Emerg Med 2004;11:237-9. Back to cited text no. 7 |
| 8. | Takagi S, Miyazaki S, Fujii T, Daikoku S, Sutani Y, Morii I, et al . Dexamethasone-induced cardiogenic shock rescued by percutaneous cardiopulmonary support (PCPS) in a patient with pheochromocytoma. Jpn Circ J 2000;64:785-8. Back to cited text no. 8 |
| 9. | Shaw TR, Rafferty P, Tait GW. Transient shock and myocardial impairment caused by phaeochromocytoma crisis. Br Heart J 1987;57:194-8. Back to cited text no. 9 |
| 10. | Tantawanichpisal D, Rujiwanichkul K, Yipintsoi T. Precipitous hypotension after nifedipine in pheochromocytoma: report of 2 cases. J Med Assoc Thai 1993;76:56-9. Back to cited text no. 10 |
Copyright 2005 - Journal of Postgraduate Medicine
The following images related to this document are available:
Photo images
[jp05085t1.jpg]
[jp05085f1.jpg]
|

{kind=link}
{kind=link}