 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 52, No. 2, April-June, 2006, pp. 134-135 Case Report Isolated breast mucormycosis Thapar VinayKumar, Deshpande A, Jain VK, Bhowate P, Madiwale C* Departments of Surgery
and Pathology*,
Seth G.S. Medical
College & K.E.M.
Hospital, Parel,
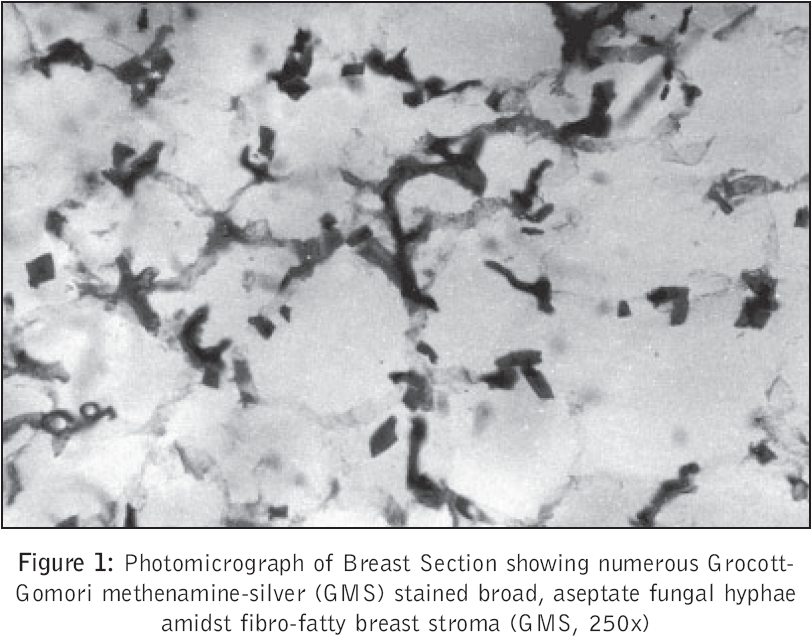
Mumbai – 400012, India Code Number: jp06040 Abstract Mucormycosis is unusual in surgical practice. Awareness of the classical findings leads to early detection. Excisional therapy whenever possible along with systemic antifungal treatment is the key to successful outcome. A 70 year old female, a known case of diabetes mellitus and chronic obstructive pulmonary disease, on inhalational steroids and oral hypoglycemic agents, presented to us with complaints of sudden onset pain, redness and swelling of left breast. A diagnosis of severe mastitis was made and a release incision was taken. The entire breast became gangrenous in next 24 hours and simple mastectomy had to be performed as a life saving measure. Histopathology revealed mucormycosis of breast. To the best of our knowledge this is the first reported case of mucormycosis of breast in the English literature.Keywords: Mucormycosis, breast gangrene, mastectomy Mucormycosis is the common name given to several different diseases caused by fungi of the order Mucorales.[1] Rhizopus species are the most commonly isolated agents of mucormycosis, followed by Rhizomucor .[1] These fungi, which are widely distributed in nature usually, affect patients who are severely immunocompromised or those with diabetes mellitus or trauma.[1] Solid organ transplant recipients represent a growing population at risk.[2] More than half of patients have rhinocerebral disease; approximately 10% have pulmonary, cutaneous, or disseminated disease; and 2% have kidney or gastrointestinal involvement.[1] Breast involvement has not been described to date in the English literature reviewed by the authors. Case History A 70 - year - old female presented with sudden onset of pain, redness and swelling of the left breast of 2 days duration. There was no history of trauma. She was a known case of diabetes mellitus on irregular treatment with oral hypoglycemic agents. She was also receiving inhaled corticosteroids for chronic obstructive pulmonary disease. On examination, patient was toxic, febrile and had pulse rate of 110 beats/minute. Her left breast was swollen, red, tender and warm. Investigations revealed a hemoglobin concentration of 10 gm% with a white cell count of 15,500/cu.mm. Renal and liver function tests were within normal limits as was the chest radiograph. A working diagnosis of severe mastitis with probable abscess was made. A release incision was taken over the breast to reduce the tissue tension and drain underlying pus collections if any. The entire breast tissue was edematous and there were no localized pus pockets. However, within 24 hours the underlying breast tissue showed necrosis with black eschar formation and gangrenous changes. A simple mastectomy was required to control the spread of necrosis. Histopathological examination revealed extensive necrosis of the breast parenchyma with polymorphonuclear infiltration, hemorrhage and thrombosed blood vessels. Seen amidst this inflammation were many broad aseptate hyaline fungal hyphae branching at 90o suggestive of mucormycosis. [Figure - 1] Patient was started on intravenous Amphotericin-B (dose of 1 mg/kg/day in the form of infusion in 5% dextrose) for a total of seven days and had an uneventful recovery. The open wound was grafted with split thickness skin graft after 4 weeks. She is asymptomatic at 2 month follow up.Discussion Mucormycosis (phycomycosis, zygomycosis) as an infection is uncommon and is largely confined to severely immunocompromised patients such as diabetics, solid organ transplant recipients and trauma.[1],[2] The Mucoraceae are ubiquitous fungi that are common inhabitants of decaying matter. In contrast to the widespread distribution of these fungi, the infrequency of disease caused by these organisms attests to their low virulence potential in the human host.[1] The exact mechanisms responsible for the increased susceptibility to mucormycosis in various patient groups are not clear. Undefined defects of macrophages and neutrophils, present in diabetics and steroid-treated patients, may be important in allowing the replication of the Mucorales as was seen in this patient.[1],[3] Once the fungus begins to grow, the hyphae invade tissue and have a special affinity for blood vessels. Direct penetration and growth through the blood vessel wall explain the propensity for thrombosis and tissue necrosis, two major hallmarks of the histopathology of mucormycosis.[1] There are six different manifestations of mucormycosis based on clinical presentation and involvement of a particular body site: (1) rhinocerebral, (2) pulmonary, (3) cutaneous, (4) gastrointestinal, (5) central nervous system, and (6) miscellaneous.[4] In general, the predilection for type of presentation varies with the underlying or predisposing condition. For example, patients with diabetes most often develop rhinocerebral mucormycosis, leukemic patients who have neutropenia or patients who become neutropenic during bone marrow transplantation for other diseases develop rhinocerebral or pulmonary mucormycosis, and those with protein-calorie malnutrition most often present with gastrointestinal disease. Disseminated disease results from progression from any of the primary anatomic location and is particularly troublesome in patients with severe immunologic deficits, such as those with bone marrow transplants or acute leukemia.[4],[5] The hallmark of disease caused by the Mucorales are vascular invasion and tissue necrosis which results in black eschar and discharges. Diagnosis depends on demonstration of the organism in the tissue of a biopsy specimen. Grocott-Gomori methenamine-silver (GMS) stain is the best stain to use, but hematoxylin and eosin and periodic acid-Schiff are also useful.[1] The classical finding is that of necrotic and edematous tissue with neutrophilic infiltrate and presence of broad, nonseptate hyphae with branching at 90°.[1] Growth of this fungus occurs best in brain-heart infusion agar, potato dextrose agar, or Sabouraud dextrose agar.[1] Systemic Amphotericin-B is the mainstay of treatment.[1] Liposomal Amphotericin-B may be more efficacious; it is less toxic, allowing higher dose of medications to be given.[1] Complete treatment of underlying medical disease is required. Any steroid medication, antimetabolites or immunosuppressants that the patient is on should be addressed and discontinued if necessary.[1] Aggressive surgical debridement of all necrotic tissue is necessary, sometimes requiring multiple debridements. Frozen section-guided debridement has been advocated as a method for operative intervention and as an alternative to the extensive debridement that has traditionally been performed in patients with invasive mucormycosis.[6] Adjunctive hyperbaric oxygen therapy has been considered beneficial in a small number of patients.[7] Overall, the earlier the diagnosis of mucormycosis is made, the better is the outcome. Survival of patients with pulmonary or disseminated mucormycosis is rare.[1] In our patient, spores are likely to have gained entry to breast through unknown trivial trauma and multiplied and invaded the breast tissue with uncontrolled diabetes, old age and inhalational steroid acting as predisposing factors. Cases of cutaneous mucormycosis have been described after minor trauma; some of these patients had diabetes.[8],[9] Prompt excisional therapy complemented with systemic Amphotericin B led to a favorable response. References
Copyright 2006 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp06040f1.jpg] |
| |||||||||

{kind=link}