 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
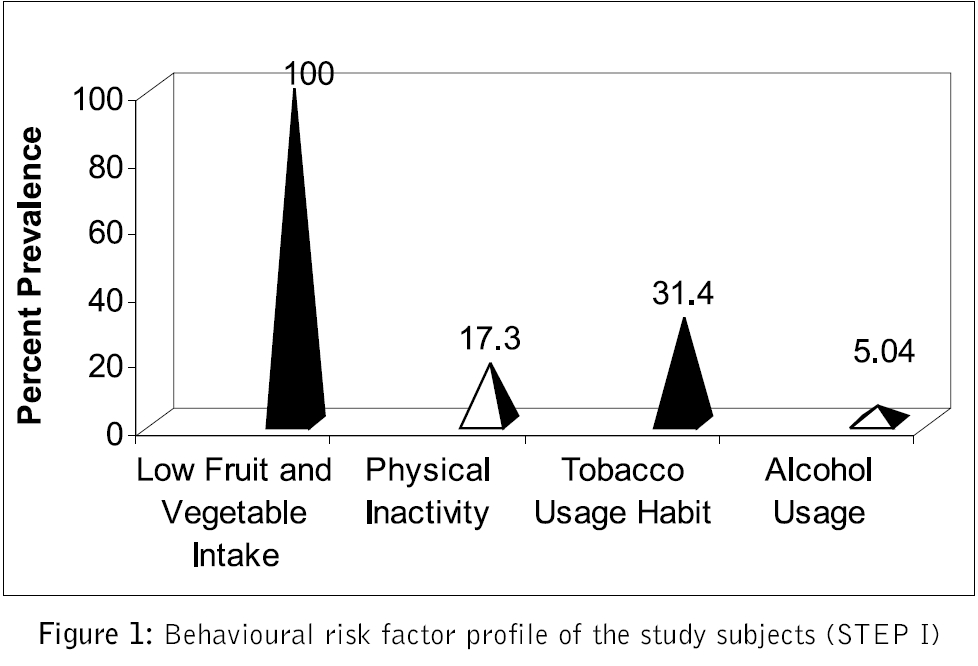
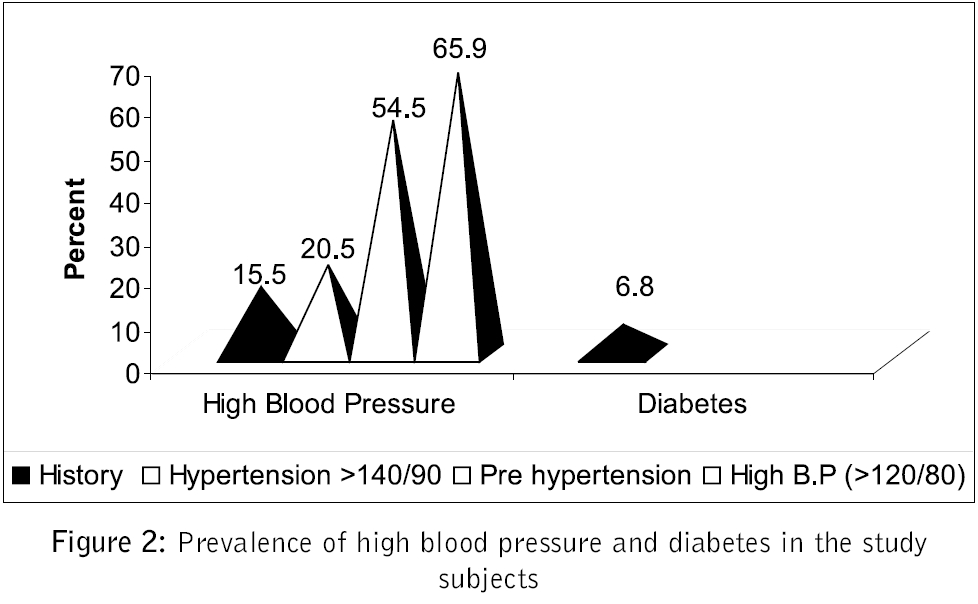
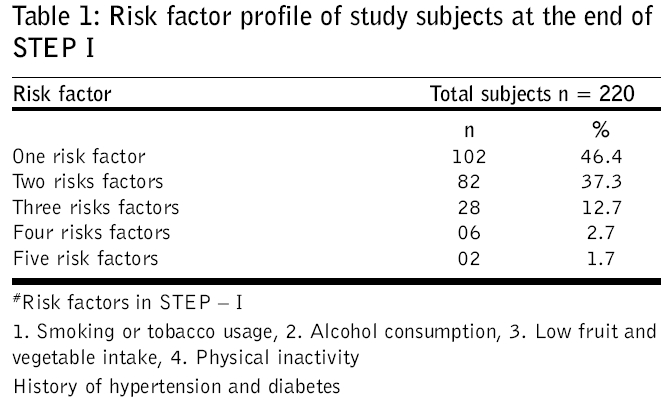
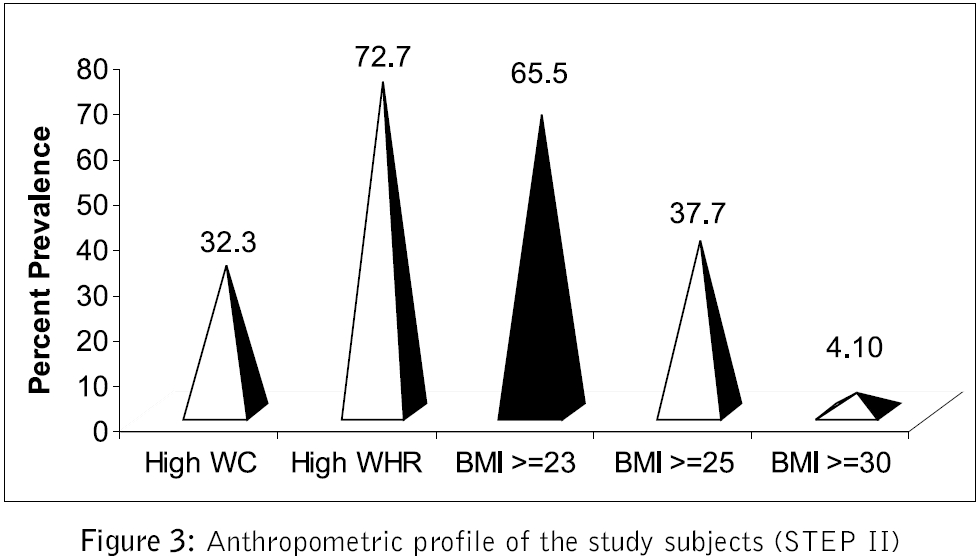
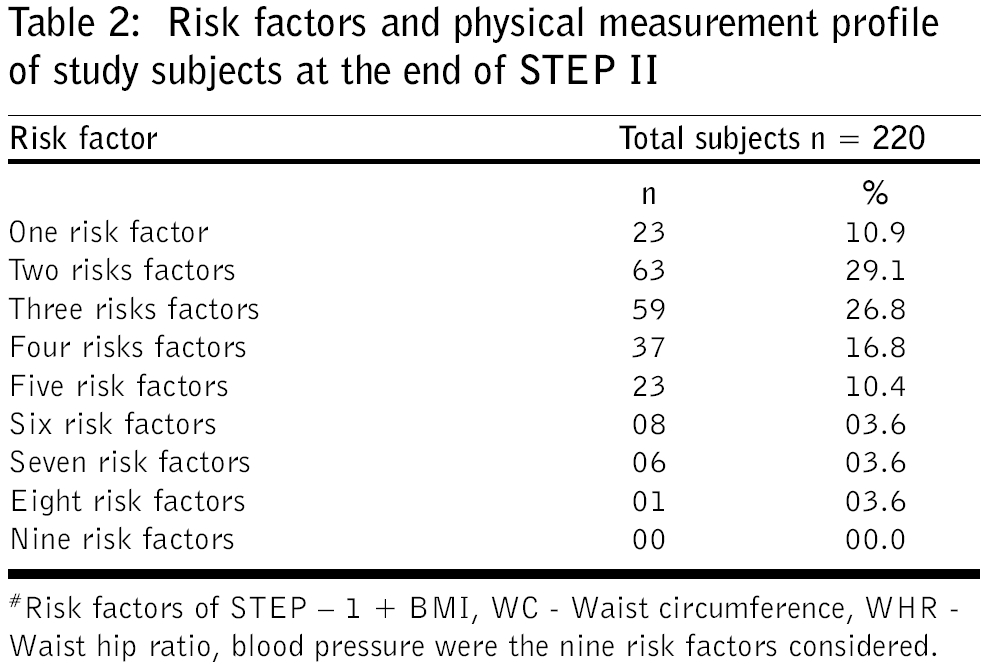
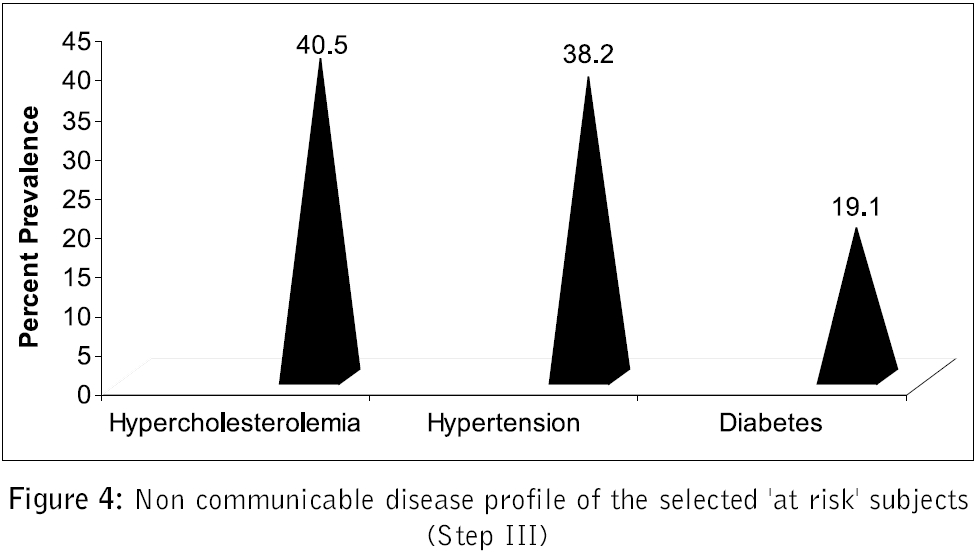
Journal of Postgraduate Medicine, Vol. 52, No. 3, July-September, 2006, pp. 167-171 Original Article Profile of non communicable disease risk factors in an industrial setting Mehan MeenakshiBakshi, Srivastava N, Pandya H Department of Foods & Nutrition, MS University of Baroda, Baroda, Gujarat Code Number: jp06056 Related articles: jp06057, jp06058 Abstract Aim: The profile of non communicable diseases (NCD) risk factors was identified in an industry by pre tested WHO's STEPS questionnaire.Settings and Design : A cross - sectional survey of all employment categories of an Industry (2000 employees) was done after randomly selecting subjects (220) from worker (52%) and non worker categories (47.4%), after informed consent. Materials and Methods: Information was collected on behavioural risk factors (STEP I), followed by anthropometric and blood pressure measurements by a trained investigator (STEP II). STEP III constituted biochemical assessment of "at risk" subjects (> 3 risk factors). Statistical Analysis : Percentage of subjects having NCD risk factors and the odds ratios were calculated. Results : Overall risk factor profile of the study subjects revealed universal prevalence of < 500 gms daily intakes of vegetables and fruits, followed by 65.9% and 65.5% prevalence of high blood pressure and high BMI respectively. Central obesity was present in 72.7% of subjects (high waist hip ratio) and 32.3% (high waist circumference) respectively. Tobacco usage, inactivity and alcohol usage habit was prevalent in 31.4, 17.3% and 5% of the study subjects respectively. A total of 34.1% of the subjects were identified as being "at risk" (> 3 risk factors) with prevalence of hypercholesterolemia, hypertension and diabetes of 40.5, 38.2 and 19.1% respectively. Conclusions : A high prevalence of NCD risk factors in industrial setting was seen; therefore public health approaches are required at workplace settings to curtail the rising epidemic in the productive populations. Keywords: Non communicable diseases, risk factors profile, industrial/productive population, STEPS methodology. Non communicable diseases (NCDs), especially cardiovascular disease, cancer and Type 2 diabetes mellitus, account for 53 and 44% of all deaths and disability adjusted life years (DALYs) respectively in India.[1] CVD deaths are more seen in working people aged 35-64 years, in whom 35% of CVD deaths occur.[2] Prevalence of diabetes and its adverse health effects have risen more rapidly in South Asia, including India. By 2030, while most people with diabetes in developed countries will be aged 65 years or more, in the developing countries the majority will be in the 45-64 years age category and afflicted in their most productive years.[1],[4] Cancer alone contributed to 14% mortality in the SEA region in 2002[5],[6] and in India alone in the year 2005, 7% deaths were attributed to cancers.[3] Unhealthy diet and physical inactivity are the leading causes of the major non communicable diseases. The important risk factors identified are high blood pressure, high serum cholesterol, inadequate intake of fruits and vegetables, excess weight, physical inactivity and tobacco use. Smoking also increases the risk for these diseases, although largely through independent mechanisms.[6],[7],[8] These factors are interrelated to each other so much so that appearance/occurrence of one factor paves the way for the other, thereby leading to the development of NCDs.[6] Risk operates in continuum with adverse events in persons with modest elevation of many risk factors, having a multiplicative effect.[8] Therefore, primary prevention of occurrence of risk factors along with their early identification and management can help delay the progress to NCDs. Similarly, since the underlying (risk) factors for all the NCDs are common, identifying and modifying these risk factors have been recommended as a strategy for their prevention and control in various settings.[8],[9] WHO′s STEPS methodology, provides a framework for the surveillance of risk factors of NCDs.[10],[11] Settings approach has been recommended as a strategy by WHO, for targeting large groups of population at a time.[12] Workplaces having productive populations need special attention owing to their higher vulnerability for NCD. Thus the present study was planned with an objective to identify the risk factors of NCDs in all employment categories of the industry. Materials and Methods One chemical industry of 2000 employees was selected to study the profile of risk factors for NCDs by using WHO STEPS pre tested questionnaire.[10] WHO STEPS questionnaire was pre tested in adults between 25-58 years in 5 industries other than sample for study and was adapted for local terms and translated in local language for better understanding. A total of 220 employees from all employment categories, willing to provide written, informed consent were randomly selected from the industry. Ethical clearance was obtained from both the institutions before conducting the study. STEP I: Socio-economic and behavioural risk profile The information on the socio-economic status and behavioural risk factors of the subjects was collected with the help of STEPS questionnaire, by interview. This step focused on self-reported information on risk factors like tobacco usage (cigarette/beedi smoking, oral and snuff tobacco), alcohol consumption and average amount consumed in a day. A standard measure of 60 ml was used to take information on amount of alcohol consumed. Dietary and physical activity pattern and past history of hypertension and diabetes was also obtained. Information on the total fruits and vegetables consumed daily, excluding tubers was obtained by asking the serving size (100 gms of fruits and vegetable consumed was taken as one serving) of consumed vegetables and fruits in the last 24 hours, with the help of standard cups (200 ml), also crossed checked by obtaining information about the amount of fresh fruits and vegetables purchased by the family every day and the portion of consumption by the target subject. Similarly an assessment of per capita amount of fat, vegetables and fruits served was obtained by taking information on the number of employees served lunch, snacks daily and the amount of foods (fresh fruits and vegetables, cooking oil) used daily to assess the gross per capita consumption. Cooking practices at workplace were also assessed by interviewing canteen personnel. Type of physical activity undertaken by the subjects was assessed by guidelines provided by the centre for disease control (CDC).[13] Based on the guidelines, a list of activities undertaken as part of work, travel and leisure were measured and classified as mild, moderate and heavy intensity. The subjects undertaking at least 30 minutes of moderate intensity activity daily, in any sphere of their daily routine (activities during working hours, for travelling and leisure time) were considered active. For assessing physical activity while travelling, information was obtained on usage of motorized vehicle, cycle or walking. The usage of motorized vehicle was considered as light activity. Usage of bicycle (< 30 minutes) and walking (< 20 minutes) was considered to be moderate activity, while if more time (>20-30 minutes) was spent on each activity, it was considered heavy. STEP II: Anthropometry Anthropometric measurements like weight, height, waist circumference and hip girth were taken. Blood pressure measurements of all the study subjects were also undertaken using standard procedures by trained (certified by industry doctor) investigator. Sub optimal high blood pressure (>120/80 mmHg) is the leading risk factor for non communicable diseases and is therefore included as a risk factor in WHO STEPs methodology. However, overall prevalence of diabetes was based on history only. The indices of body mass index (BMI) and waist circumference (WC), waist hip ratio (WHR) were calculated from recorded measurements. Classification of over weight and obesity by global and Asia Pacific classifications was done. Central/ truncal obesity was determined, based on WHO recommendations.[14] STEP III: Biochemical estimations of the "at risk" individuals The subjects having more than 3 behavioural and/or anthropometric risk factors from STEP I and II were identified as being "at risk". Those consenting to give blood sample, were assessed biochemically for parameters like fasting blood glucose, fasting total cholesterol and triglycerides and HDL cholesterol levels by using standard methods.[15] All the study subjects were individually counselled on methods to reduce risk factors and all the nutrition and health concerns of the employees were addressed. At the end of the study, copy of the report of the study was submitted to the Industry and sensitization of the human resources personnel was also done to initiate nutrition health promotion program in their setting. However, no further intervention was done. Statistical analysis Data were analyzed using Epi-info version-6.04d computer package (developed by Center for Disease Control and Prevention (CDC), U.S.A. and WHO, Geneva). All values were expressed as percentages for qualitative variables, Mean ± SD was calculated for quantitative variables. Odds ratios were calculated between risk factors and NCD. Results Socio-economic and behavioural risk factor profile of the selected study subjects (STEP I) A total of 220 male subjects comprised of 21 executives, 41 executive assistants, 40 administrative staff and 118 workers. Almost 53.6% (118/220) of the study sample was from worker category, while 46.4% (102/220) of the study subjects were those engaged in desk jobs. Initially all the executives of the industry (43) consented to participate in the study but dropped out subsequently and only 21 (49%) executives completed the study. All other subjects completed the study up to STEP II. About 65.5% (144/220) of the study subjects were in the age group of 45-54 years, followed by 18.6% (41/220) in the age group of 35-44 years and 15.5% (34/220) in the age group of > 55 years. All the subjects were in their productive years with almost all subjects (99.5%) between the age of 35-58 years, with only one (0.5%) subject (1/220) in the age group of 25-34 years. 58.2% (128/220) had monthly income ≤ Rs. 6000, followed by 28.6% (63/220) having income between Rs. 6001-12000 per month. Also 38.2% (84/220) had educational level till 10th standard. The habit of smoking (cigarette or beedi) and chewing/snuff tobacco was present in 13.6% (30/220) and 15.9% (35/220) of the study population respectively. Total tobacco usage habit (any form) was 31.4% (69/220). Majority (53.3%, 16/30) of the smokers, took ≤ 10 cigarettes, while 30% (9/30) and 16.6% (5/30) of smokers smoked 11-20 cigarettes and 21-30 cigarettes daily respectively. More than half 54.3% (19/35) of oral tobacco users consumed ≤ 5 packets daily, while 42.9% (15/35) of oral tobacco users consumed 6-10 packets daily. Alcohol consumption habit was in 5.0% (11/ 220) in the study subjects. Gujarat being a dry state, details about frequency and amount of consumption were not revealed by the subjects. A possibility of underreporting cannot be ruled out. Majority (91%) of the subjects (200/220) were vegetarians. All the study subjects had low intakes of fruits and vegetables (< 500 gms/day). The mean (± SD) daily vegetable and fruit consumption was 190.0 ± 51.1 g/day. The per capita consumption of fat was 75 gms of PUFA rich oil (cotton seed) with refrying of oil routinely done. There was virtual absence of fruits served in the canteen with only 30 gm/capita availability of vegetables (excluding potatoes). None of the subjects, including workers, were found to be engaged in heavy activities at workplace. Majority (61.4%) of the subjects (135/220) were engaged in light activities, like table work, sitting in front of the computer, packing, paperwork and others. About 38.6% (85/220) reported to perform moderate activities at work like using stairs for climbing or moving down, walking as a break from work, brisk walking at the workplace, carrying a load and others. The most frequent mode of transportation for reaching workplace by executives (21/21) and their assistants (32/41) was by motorized vehicle, while majority (65.2%) of the workers (77/118) used bicycles as their mode of transportation. About 53.2% of the subjects (117/220) engaged in light activities such as T.V. viewing, reading newspaper and walking in the house. Only 14.3% of executives (3/21) were engaged in moderate activities, with 85.7%, (18/21) being sedentary. About 17.3% (38/220) of the subjects were categorized as physically inactive (sedentary workers at all the spheres of daily activity). [Figure - 1] demonstrates the highlights of the behavioural risk factor profile of the study subjects. History of hypertension and diabetes was reported in 15.5% (34/220) and 6.8% (15/220) of the subjects respectively [Figure - 2]. A large percentage (41.4-55.0%) of the study subjects never went for a health check up. On screening for hypertension, about 5% new asymptomatic cases were identified. [Figure - 2] shows that the overall prevalence of hypertension (History + newly diagnosed hypertensive after screening at the end of STEP II) in the study population was 20.5% (45/220). More than half (54.5%) of the study subjects (120/220) were in pre hypertension stage [16]. A total of 65.9% (145/220) of the study subjects had sub optimal high blood pressures (>120/80 mmHg). At the end of STEP I, none of the subjects were free from any risk factor and most of the subjects had either one (46.4%, 102/220) or two (37.3%, 82/220) risk factors [Table - 1]. Physical/ anthropometric measurements of the study subjects (STEP II) The mean BMI of the subjects was 24.11 kg/m 2. [Figure - 3] gives the physical measurements profile of the study subjects. The prevalence of obesity as defined by WHO criteria (BMI ≥ 30 kg/m 2) was 4.1% (9/220), which increased dramatically to 37.7% (83/220) on taking the criteria (BMI ≥25 kg/m 2) as recommended for Asia Pacific population.[14] Similarly, a large proportion (72.7%, 160/220) of the study subjects had high waist: hip ratios (> 0.9), with 32.3% (71/220) having high (≥ 94 cms) waist circumference [Figure - 3]. At the end of STEP-II, [Table - 2] majority of the subjects had the presence of either 2 (29.1%, 63/220) or 3 risk factors (26.8%, 59/220). Bio-chemical estimations of the at risk study subjects (STEP III) A total of 75 subjects (34.1%) had more than three risk factors and were thus identified as "at risk" subjects. Only 56% (42/75) of the identified subjects agreed for biochemical estimations. About 40.5% (89/220) of the identified "at risk" subjects were hypercholesterolemic (>190 mg/dl),[19] with the mean cholesterol levels of 183.4 ± 31.2 mg/dl. It was surprising to note that none of the subjects had low (< 35 mg/dl) HDL-C, with the mean HDL-C levels of 46.2 ± 06.2 mg/dl. The prevalence of hypertension in "at risk" population was 38.2% (84/220) followed by diabetes (fasting blood sugar levels greater than 125 mg/dl) 19.1% (42/220), as shown in [Figure - 4]. The mean fasting blood sugar level was 101.9 ± 39.7 mg/dl. Relationship of various risk factors with NCDs Significant relationship of hypertension was observed with tobacco usage (OR: 2.83; 95% CI=1.20-6.62; P =0.007), high WC (OR: 2.46; 95%CI=1.21-5.02; P =0.006) and high WHR (OR: 2.46; 95% CI=1.21-5.02; P =0.006). No significant relationship could be observed for diabetes or hypercholesterolemia. Discussion Profile of NCD risk factors in an industrial setup showed similar trends as were reported earlier by WHO SEARO figures and the studies in free living and industrial Indian populations.[6],[18],[19],[20],[21],[22] The mean (± SD) daily vegetable and fruit consumption was 190.0 ± 51.1 g/day, which is more than 50-60% lower than 400-500 gms of intake recommended by WHO.[6],[23] Also since the leading risk factor for NCDs is high blood pressure globally as well as in SEA region, a diet high in fruits and vegetables (8-10 servings/day) is recommended to control hypertension.[24],[25] Therefore, in populations with high suboptimal blood pressures as in the present study (65.9%), it is prudent to recommend at least 500 gms of vegetables and fruits. The universal sub optimal intakes of fruits and vegetables (£ 500 gms /day) by the study population could be attributed to their high cost, or the low priority given to protective foods in Indian diets. Unhealthy behaviour like physical inactivity and tobacco usage was observed in 17.3 and 31.4% of the study population, also supported by WHO study for South East Asia region and studies from industrial populations in India.[6],[18],[19],[20],[21],[22] The prevalence of physical inactivity amongst the subjects in the industrial population (17.3%) was similar to that reported in the free living population (16.6%) in SEAR,[6] suggesting that industrial workers who were traditionally considered heavy workers were now becoming sedentary, possibly due to automation at various plant sites. Recently, a BMI of ≥ 23 kg/m 2 has been suggested to determine risk for Asia Pacific population[14] and by these criteria 65.5% of the study population had higher BMI values (BMI ≥ 23 kg/m 2). Similarly 51.4% of population with BMI ≥ 23 kg/m 2 has been reported in industrial populations across India.[18] Subjects with BMI> 25 kg/m 2 (obese by Asia Pacific and overweight by WHO classification) were 37.7%. Similarly abdominal obesity, particularly implicated for cardio-vascular morbidity and mortality was present in 32.3% (High WC). High waist hip ratios were prevalent in the study subjects (72.7%). Similar results have been previously reported in urban free living and industrial populations.[18],[19],[20],[21],[22] Long duration of working hours and a sedentary lifestyle could be responsible for this. The consumption of fat in the industrial setting comprising of one meal and snack was very high (75 gms), which may also be responsible for high obesity (generalized and abdominal) and thus, the type of food served in the industry and physical activity patterns of the population require changes. Health policy of the industries needs to focus on screening all subjects for simple parameters to determine employee′s risk status, as the study demonstrated 65.9% of population with suboptimal blood pressures (>120/80), while history of hypertension in the study was only 15.5%, thereby suggesting that 50.4% of the study population was unaware of their risk; this was mainly because many of the study subjects (41.4-55%) had never gone for a health check up. Large sums of money spent by industries for the treatment of complications of these diseases can be saved, if the public health approaches of primary prevention, recommended by WHO are adopted early and regularly by the industries. About 6.8% of study subjects had history of diabetes, which increased to 19.1% in those having more than 3 risk factors (′′at risk′′ subjects). A high prevalence (11-15%) of diabetes in free living and industrial populations of India has been reported earlier.[18],[19],[21] More than one third (34.1%) of the study subjects were identified "at risk" and hypercholesterolemia was a leading factor followed by hypertension and diabetes, which together as well as individually can contribute significantly to cardiovascular morbidity and mortality.[16],[17] The study clearly demonstrated that the significant predictors for all the above mentioned conditions were amenable to dietary and lifestyle modifications and therefore modifying these factors may be helpful in curtailing this unhealthy trend. Since the sample constituted of equal numbers of workers and non workers, the data clearly demonstrates that all the employment categories of employees were vulnerable to NCD. Therefore there is a need to plan health policies focussing on behaviour change, and communication to promote healthy diets and lifestyles amongst all employment categories. Acknowledgement We acknowledge the management of Sarabhai chemicals for permitting us to conduct the study and the empoloyees from each employment category who willingly consented to participate in the study.References
Copyright 2006 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp06056f3.jpg] [jp06056f2.jpg] [jp06056t2.jpg] [jp06056t1.jpg] [jp06056f4.jpg] [jp06056f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}