 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
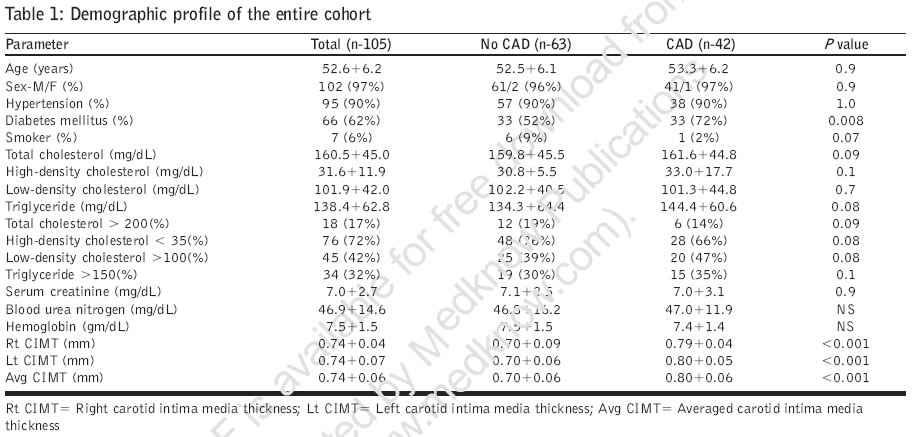
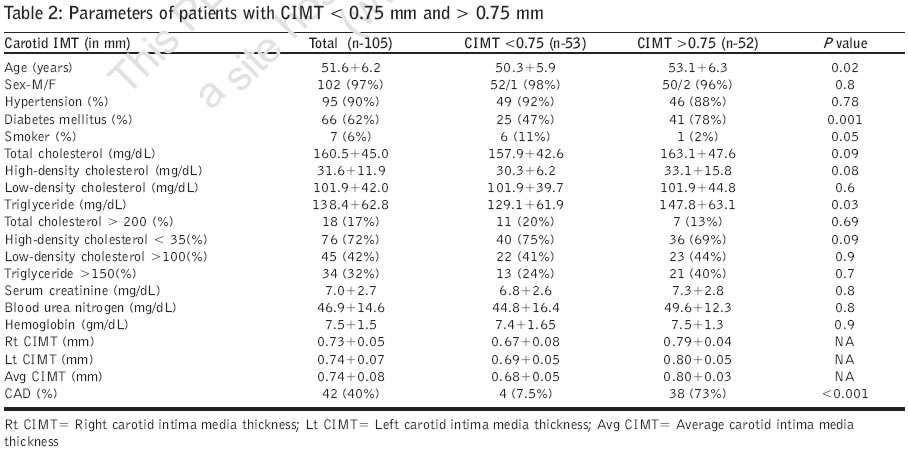
Journal of Postgraduate Medicine, Vol. 52, No. 4, October-December, 2006, pp. 266-270 Original Article Utility of carotid intimal medial thickness as a screening tool for evaluation of coronary artery disease in pre-transplant end stage renal disease Modi N, Kapoor A, Kumar S, Tewari S, Garg N, Sinha N Department of Cardiology and Nephrology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow Date of Submission: 28-Oct-2005 Code Number: jp06092 Abstract Background : Coronary artery disease (CAD) is associated with a higher incidence of allograft failure and mortalityin patients with end-stage renal disease (ESRD) following renal transplant.Aim : To evaluate the efficacy of using carotid intimal medial thickness (CIMT) to predict the presence of CADin patients with ESRD, using coronary angiography (CAG) as the gold standard. Materials and Methods : This prospective study enrolled consecutive patients with ESRD who underwent CAGas a part of pretransplant evaluation to rule out the presence of atherosclerotic CAD. An operator who wasblinded with respect to the results of the CAG, measured carotid IMT in all patients prior to CAG and recordedit on videotape. Two independent observers blinded to the results of CAG measured carotid IMT offline tovalidate its predictive accuracy as a noninvasive test in predicting the presence or absence of CAD. Measurementof carotid IMT was done on USG B mode 7.5 MHZ probe [HP 5500 andover, Massachusetts]. Student's t-testwas used for inter-group comparisons. Pearson correlation coefficient test was used to assess the relationbetween CAD and various risk factors and carotid IMT. Linear regression analysis was applied to identifyindependent factors determining presence of CAD. A P value < 0.05 was considered statistically significant. Results : Mean CIMT was significantly higher in those with CAD as compared to those without [0.80± 0.06 vs.0.70±0.06 mm, P< 0.0001). Patients with CIMT> 0.75 mm were older and had more incidence of diabetes(78% vs. 47%; P=0.001). Only 4/53 (7%) of patients with CIMT< 0.75 mm had CAD, vs. 38/52 (73%) in thosewith CIMT >0.75 mm. The sensitivity and specificity of using CIMT > 0.75 as a predictor of CAD was 90.47%and 73% and its positive and negative predictive values were 0.73 and 0.92. On multivariate analysis, onlyCIMT was a significant predictor of CAD. Conclusion : Carotid IMT can be used to predict CAD in patients with ESRD. In the absence of other risk factors,patients with IMT< 0.75 mm may not need a pretransplant CAG. Keywords: Carotid intima media thickness, coronary artery disease, prerenal transplant The mortality rate from cardiovascular disease in patients with end-stage renal disease (ESRD) varies from 40-50%.[1],[2] The increased prevalence of atherosclerotic cardiovascular disease (CVD) is also influenced by the fact that conventional risk factors like diabetes mellitus, hypertension and hypercholesterolemia are more prevalent in this patient population. Since coronary artery disease (CAD) (whether symptomatic or asymptomatic) is associated with a higher incidence of allograft failure and subsequent mortality,[3],[4] careful evaluation for the presence of CAD is critical in patients awaiting renal transplant. Although coronary angiography (CAG) is considered the gold standard for diagnosing CAD, it is an invasive procedure. Though several noninvasive tests are available (including exercise ECG,[5],[6] thallium dipyridamole scintigraphy[7],[8] and dobutamine stress echocardiography),[9] conflicting results have been reported in various studies in patients with ESRD.[5],[6],[7],[8],[9] B mode ultrasonographic imaging of distal common carotid artery with measurement of intimal medial thickness (IMT) has been shown to be a reliable marker of early atherosclerosis and several studies have shown that increased carotid IMT is an independent risk factor for ischemic heart disease and stroke.[10],[11],[12] The aim of this study was to prospectively study the efficacy of carotid IMT in predicting the prevalence of CAD in a patient population of ESRD, using CAG as the gold standard and assess if this noninvasive technique can be used in patients with ESRD to predict the presence of CAD. Materials and Methods The prospective study that conformed to the institute′s ethical protocol enrolled consecutive patients presenting at the Departments of Nephrology and Cardiology with ESRD, after obtaining informed consent. These patients, who were prospective candidates for receiving renal transplant, underwent CAG as per the institutional protocol if they were aged over 40 years; so as to rule out atherosclerotic CAD. An operator, who was blinded with respect to the results of the CAG, measured carotid IMT in all patients prior to CAG and recorded it on videotape. Two independent observers who were blinded to the result of CAG, measured carotid IMT offline to validate its predictive accuracy as a noninvasive test in predicting the presence or absence of CAD. Their inter-observer difference was less than 5%. Carotid IMT measurement Measurement of carotid IMT was done on USG B mode 7.5 MHZ probe [HP 5500 andover, Massachusetts]. On a longitudinal, two-dimensional ultrasound image of the carotid artery, the anterior [near] and posterior [far] walls of the carotid artery are displayed as two bright white lines separated by a hypoechogenic space. The distance between the leading edge of the first bright line of the far wall [lumen-intimal interface] and the leading edge of the second bright line [media-adventia interface] indicates the intima-media thickness.[13] In this study, when an optimal longitudinal image was obtained, it was frozen on the R wave of ECG and stored on videotape. This procedure was repeated on both sides. The actual measurements were performed offline. The interfaces of the distal common carotid artery were marked across a length of 10mm. The beginning of dilation of the distal common carotid artery served as the reference point for start of the measurement. At least three readings were taken and the average of three readings of carotid IMT was taken for evaluation. The intimal-medial thickness on both (right and left) sides was calculated and an average of the two values was also taken. Plaques were defined as focal widening relative to the adjacent segments, with protrusion into the lumen, composed either of only calcified deposits or a combination of calcification and noncalcified material. The site and extent of lesions were not quantified. Coronary angiography was performed by the percutaneous Judkins technique and CAD was considered significant when there was more than 50% diameter loss in coronary lumen. Statistical analysis Data are expressed as mean ± SD. Student′s t test was used for inter-group comparisons. Pearson correlation coefficient test was used to assess the relation between CAD and various risk factors and carotid IMT. Linear regression analysis was applied to identify independent factors determining presence of CAD. Factors which were found to have significant association were tested by multivariate analysis to look for their independent association. A P value < 0.05 was considered statistically significant. Results Of a total of 232 consecutive patients of ESRD who underwent renal transplants, 105 were subjected to pretransplant CAG as per the protocol of the institution. These patients were on maintenance dialysis and were waiting for transplant. The mean age of these patients was 51.6±6.2 years (range 38-64 years) and of these 102 (97.1%) were males. The mean length of time from diagnosis of ESRD to transplant was 14.3±9.4 months. Overall, diabetic nephropathy was the commonest cause of ESRD in the patient population, being present in 61/105 (58%) cases, while other causes included chronic interstitial nephritis (16/105) and chronic glomerulonephritis (12/105). Echocardiographic studies performed prior to CAG revealed a mean ejection fraction (EF) of 49.5±5.3% (range 37.5-64.4%). Resting regional wall motion abnormalities (RWMA) were present in 19 (18%) patients. On CAG, 42/105 (40.0%, Group 1) patients had CAD, while 63/105 [60%, Group 2] had normal coronaries. Of the 42 patients with CAD, 34 (80.9%) had single vessel disease, 5(11.9%) had double vessel disease and 3(7.1%) had triple vessel disease. Demographic and risk factor profile in patients with and without CAD [Table - 1] The mean age, gender distribution, lipid levels and the incidence of hypertension and smoking were comparable between these two groups. The overall incidence of ESRD patients (n= 105) having total cholesterol (TC)> 200 mg/dl was 18(17%), triglyceride (TG)> 150 mg/dl was 34(32%), high-density cholesterol (HDL) < 35 mg/dl was 76(72%) and low-density cholesterol (LDL) > 100 mg/dl was 44(42%). The only risk factor whose incidence was significantly different between the two groups was diabetes mellitus; present in 30 (72%) of those with CAD and in 13 (52%) of those without CAD, ( P =0.008). The mean hemoglobin, serum creatinine and BUN levels were also similar between the two groups. History of exertional angina or ECG were not of much help in categorizing whether or not the patient had CAD, since symptomatic angina was present in only 10/42 (24%) patients with CAD. Only four patients had a past history suggestive of acute coronary syndrome or myocardial infarction. The baseline ECG was normal in 61/105 (58%) while 44/105 patients (42%) had an abnormal ECG. The commonest abnormality noted was presence of LVH (in 37, 35%), left bundle branch block (in 5, 5%) and pathological Q waves (in 2, 2%). On echocardiography, LV dimensions, ventricle wall thickness and LVEF were similar in both the groups (with/without CAD). Presence of RWMA was slightly more common in those with CAD (n=12/42; 28%) than those without CAD (n=7/63; 11%, P = 0.02). Carotid IMT The mean carotid IMT of the entire group (n= 105) was 0.74±0.06 mm. When the mean carotid IMT of ESRD patients with CAD (Gp 1, n= 42) was compared to those without CAD (Gp 2, n= 63), significant differences were observed. The mean right carotid IMT was significantly higher in those with CAD than those without CAD (0.79±0.04 mm vs. 0.70±0.09 mm, P < 0.0001). A similar trend was observed for the mean left carotid IMT (0.80±0.05 mm vs. 0.70±0.03 mm, P < 0.0001) and for the average carotid IMT (bilaterally) (0.80±0.06 mm vs. 0.70±0.06 mm, P < 0.0001) [Table - 1]. Categorization of patients according to mean carotid IMT [Table - 2] Patients were further divided into two groups according to average carotid IMT (average IMT> 0.75 mm and those with IMT< 0.75 mm). The incidence of hypertension, smoking and lipid levels was comparable between the two groups. Patients with IMT> 0.75 mm were slightly older (53.1±6.3 vs. 50.3±5.9 years; P =0.02) and had a more frequent incidence of diabetes (78% vs. 47%; P =0.001). Only 4/53 (7%) of patients with IMT< 0.75mm had angiographically proven CAD, while the corresponding number for those with IMT> 0.75 mm was 38/52 (73%, P < 0.0001). The sensitivity of using carotid IMT as a test to predict the likelihood of CAD (using CAG as a gold standard) was 90.47%, while its specificity was 73%. The positive and negative predictive values of using carotid IMT as a noninvasive marker to detect CAD in ESRD was found to be 0.73 and 0.92 respectively. On univariate analysis age ( P = 0.02), diabetes ( P = 0.01), echocardiographic RWMA ( P = 0.01) and carotid IMT ( P = 0.0001) were found to be significant predictors of the presence of CAD. However, on multivariate analysis, only carotid IMT ( P = 0.0001) was a significant predictor of the presence of CAD. Discussion Cardiac disease is the leading cause of death among patients with ESRD. Coronary artery disease is especially common among patients with ESRD, with prevalence rates 5-20 times more than that in the general population.[1],[2],[14] Even after stratification for age, sex, race, diabetes mellitus and hypercholesterolemia, the mortality rate from CVD in patients with ESRD is 10-20 times greater than that in the general population, lending credence to the fact that atherogenesis may be accelerated in patients with renal impairment.[5],[15] Not only is atherosclerotic CAD associated with an increased incidence of allograft failure and mortality in patients with ESRD, the pooled incidence of fatal and nonfatal cardiovascular events remains high even following the transplant.[3],[4],[16] Hence if CAD is suspected clinically or due to an excessive clustering of risk factors, reliable diagnostic procedures are indicated. We noted a prevalence of 40% of angiographically documented CAD in our patient population of ESRD awaiting renal transplant, which is in agreement with the incidence of 25-55% reported by other studies.[3],[4],[17] The relative insensitivity of a resting ECG or history of exertional or rest angina to predict CAD in patients with ESRD has been reported previously[5],[18],[19],[20],[21] and has been corroborated by us. Only 25% of our patients were symptomatic while the resting ECG was normal in 58% cases. Though many centers now recommend pretransplant CAG for most transplant candidates with diabetes,[6],[22] it is a costly, invasive and non-risk free procedure, especially in a sick patient-population like ESRD. There is a need for an ideal noninvasive screening procedure for ESRD patients to diagnose CAD. Several noninvasive tests are available and used frequently including exercise ECG, thallium dipyridamole scintigraphy and Dobutamine stress echocardiography. However, the low sensitivity of these tests in diabetic patients with ESRD is known.[5],[6],[7],[8],[9],[23] Atherosclerosis is a diffuse process involving the coronary arteries, carotids and the peripheral vasculature and since Pignoli et al[24] demonstrated that ultrasound can be used to measure carotid IMT, studies have documented that increased carotid IMT correlates well with coronary atherosclerosis and its risk factors.[10],[11],[12],[25] In our study, we found that mean carotid IMT was significantly higher in patients with angiographically documented CAD. A cut-off of 0.75 mm was useful in predicting CAD in patients with ESRD awaiting renal transplant. To the best of our knowledge no previous study has assessed the role of carotid IMT as a screening test to predict occurrence of CAD in patients with ESRD awaiting renal transplant, using CAG as the gold standard. Though Pascazio et al[26] performed echo Doppler imaging of carotid vessels in hemodialysis patients and studied the prevalence of atherosclerotic plaques in the carotid vessels; they did not validate it with CAG. However, even in their study, the degree of carotid disease was significantly higher in dialysis patients than in control subjects with cardiovascular events. Patients with ESRD have a reduced life expectancy, due in large part to increased mortality and morbidity from atherosclerotic cardiovascular disease. Identification of CAD in such patients, who are often asymptomatic, is problematic. Coronary angiography, which is considered the gold standard for diagnosing CAD is an invasive technique and a noninvasive modality to assess CAD in such patients is desirable. We observed that CIMT> 0.75 mm was a strong predictor for CAD in ESRD patients and can be used as a noninvasive screening test for these patients for pretransplant cardiac evaluation with high sensitivity, specificity and positive predictive value. The study had its share of limitations. The numbers in the study are relatively small. (Of the 105 patients undergoing CAG, 42 had documented CAD.) Since CIMT is easily measurable, its role in predicting the presence of CAD in such patients awaiting renal transplant needs to be studied in a larger number of patients. It would be interesting to see if CIMT has a correlation with the severity of angiographic CAD in these patients. Since out of 42 patients, 34 had single vessel disease, and only 8 had double or triple vessel disease, to make valid comparisons large number of patients need to be studied. References
Copyright 2006 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp06092t2.jpg] [jp06092t1.jpg] |
| |||||||||

{kind=link}
{kind=link}