 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
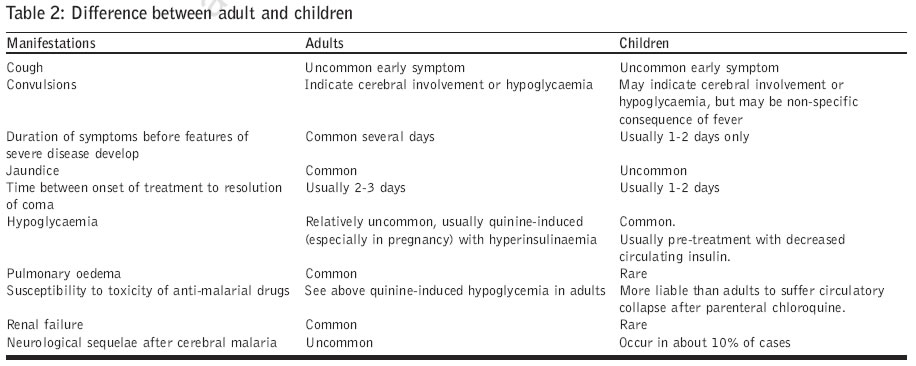
Journal of Postgraduate Medicine, Vol. 52, No. 4, October-December, 2006, pp. 281-287 Symposium Management of severe and complicated malaria Mishra SK, Mohanty S, Mohanty A, Das BS Internal Medicine and Critical Care Unit, Ispat General Hospital, Rourkela, Orissa Date of Submission: 19-May-2006 Code Number: jp06095 Abstract Severe malaria is invariably caused by Plasmodium falciparum. In India, both adults and children are affectedby severe malaria. However, children are more prone for developing anemia and convulsions as manifestationsof severe malaria, while acute renal failure and jaundice are more common among adults. Pregnant women arevulnerable to hypoglycemia, anemia and pulmonary complications. The case-fatality rate due to severe malariais 10-15% in spite of therapy but it increases in the presence of renal failure or respiratory distress (pulmonaryedema or ARDS). Of late, multi-organ failure and high mortality figures are being reported increasingly fromdifferent parts of India. Early diagnosis and prompt treatment will reduce the mortality due to malaria. Cerebral malaria should alwaysbe suspected in a patient with altered sensorium in a malaria-endemic area. However, other causes ofunconsciousness such as encephalitis, meningitis or hepatic coma should also be excluded. Parenteral quinineis the mainstay of therapy. A recent multi-centric study has demonstrated the efficacy of intravenous artesunatein reducing the mortality by 30%. The usefulness of adjunct therapy is still controversial. Keywords: Cerebral, malaria, renal failure, severe malaria Every year about 300-400 million people suffer from malaria around the globe, out of whom 2-3 million-- die due to its complications.[1] Throughout the history of mankind, malaria has claimed more lives than all the wars put together. Hence, the matter deserves urgent attention of the healthcare providers, especially of those who practice in the tropical countries. The management of severe malaria is a medical emergency and has to be promptly instituted. A delay in diagnosis and/ or in institution of therapy may result in an avoidable fatality. Malaria is a febrile illness and its clinical features are highly nonspecific. The diagnosis depends on a high degree of clinical suspicion and confirmation by detecting the asexual form of Plasmodium falciparum (Pf) in peripheral blood smear. Microscopy is the gold standard for the diagnosis of malaria due to its cost-effectiveness, sensitivity and high degree of specificity. It can estimate parasite density and identify the parasite species involved, provide clues about platelet and leukocyte counts and can help to differentiate malaria from many other conditions. However, it has certain disadvantages, too: False negative results may be encountered in patients with low parasitemia, maturation of sequestered parasites in broods, partial treatment with anti-malarial drugs or receipt of effective chemoprophylaxis. Technical factors such as poorly prepared slides, poorly stained slides, poor quality microscope, examination of only thin films and inexperienced technician can also contribute to an increase in the false negative rates. False positive results are encountered due to mistaking stain particles for malarial parasite by inexperienced microscopists. Technical problems with light microscopy have spawned interest in the test based on parasite-derived proteins like HRP-II (Histidine Rich protein-II). The test has become relatively popular due to its simplicity and high levels of sensitivity and specificity. In addition, it provides results in quick time and, does not require a great degree of expertise or sophisticated equipment or laboratory facilities for its performance. Thus, it can be used in peripheral hospitals and field conditions. It is particularly helpful in partially treated cases and those with low parasitemia; where microscopy is not available or likely to be negative. Its limitations are that HRP-II may continue to be positive up to two-four weeks even when parasites are no more detected in the peripheral blood. Monitoring parasite clearance, quantification of parasite load and stage identification are not possible with these immunological tests.[2] The WHO defines severe malaria by the following criteria, along with the asexual form of P. falciparum in the peripheral blood smear.[3] Though for research and publication purposes, cerebral malaria is defined as unarousable coma, appropriate treatment can be initiated even in patients having milder grades of altered sensorium or in those with neuro-psychiatric manifestations with asexual parasitaemia in the peripheral blood smear or a positive rapid diagnostic test. In an endemic area, a person having febrile illness and altered sensorium should be treated as a case of cerebral malaria even though parasitemia has not been demonstrated. As shown in [Table - 2], the manifestations of severe malaria may differ in children. Common manifestations of severe malaria in children include severe anemia, cerebral malaria and acidosis. Acute renal failure, respiratory distress (ARDS) and jaundice are rarely encountered in children.[3] The frequency of manifestations of severe malaria varies with the intensity of transmission: In Africa, where the transmission of malaria is intense and stable, severe malaria is mainly a disease of children from the first few months of life till the age of five years. It is less common in older children and adults because of acquisition of partial immunity. Infants and young children suffer from manifestations of severe malaria cited above and bear the brunt of high mortality. In areas of low to moderate transmission (South-East Asia) people of all age groups are vulnerable to severe malaria. However, adults suffer from multi-organ involvement like acute renal failure, respiratory distress apart from cerebral malaria.[2],[3] There has been a paradigm shift in the clinical manifestations of malaria in the last two decades. Multi-organ failure is encountered much more frequently than before and this changing scenario could be ascribed to high transmission of falciparum malaria and drug-resistance to commonly used anti-malarial agents.[4],[5],[6] Management of Severe Malaria General management
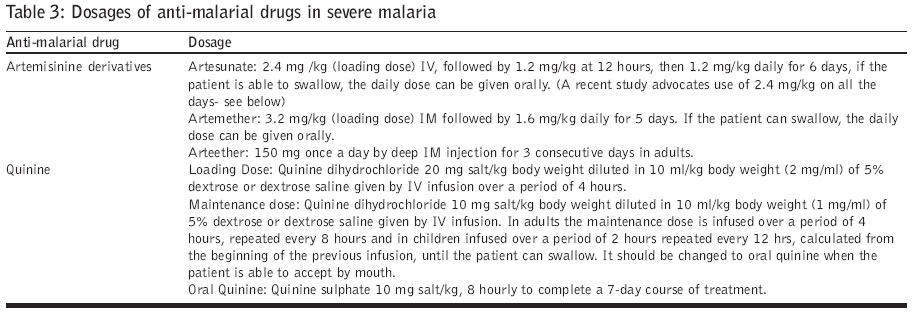
If parasitological confirmation is likely to be delayed, specific anti-malarial therapy should be started based on the clinical diagnosis. Antibiotics in appropriate doses should be given to cover for the possibility of bacterial meningitis if CSF is inconclusive or for control of other unrecognized infections. Specific anti-malarial chemotherapy All patients of severe malaria should be treated with parenteral quinine or artemisinin derivatives due to presence of widespread chloroquine (CQ) resistance in South East Asia. Quinine is used as first-line drug in severe malaria because resistance to CQ has been widely reported from most parts of the world. However, recent evidence hints at the decline in the efficacy of the drug in South-east Asia in terms of parasite and fever-clearance in uncomplicated malaria and prolongation of coma-recovery-time in severe malaria. Quinine also has a narrow therapeutic range and when given very rapidly, could result in severe hypotension that could prove lethal. Artemisinin compounds (viz. atremether, artesunate and arteether) are highly effective and rapid scizonticidal drugs. Many clinicians use one of these compounds as the first-line drug in the treatment of severe malaria. In a study from India that enrolled a small number of patients, the mortality rate was lesser with a-b-arteether in comparison to quinine. However, the differences were not statistically significant.[7] Studies from Bangladesh and Vietnam have demonstrated advantages of using artemether and its closely related compound artemotil over quinine.[8],[9] The results of this trial showed that artemether was safe and easier to use than quinine, although the overall survival rate was not significantly different.(Arteemether- Quinine Meta Analysis study Group). A large multi-center randomized placebo-control trial carried out in South-east Asia has reported 35% reduction in the mortality with parenteral (IV) artesunate as compared to IV quinine. Artesunate use was associated with very few adverse events in this study.[10] In this study IV artesunate 2.4mg/kg was used in all the doses. These studies have shown a definite beneficial effect of artesunate when compared with quinine, probably because artesunate is water-soluble and can be given intravenously in comparison to artemether or arteether which are oil-based compounds can only be given intramuscularly, resulting in an inadequate absorption from the site. Pharmaco-kinetics study with artesunate has shown that its conversion to dehydro-artemisinin, which is the active compound, is earlier than arteemether or arteether. Apart from being highly effective, artemisinin derivatives are devoid of major side-affects and their use does not warrant sophisticated or intensive monitoring. The last attribute makes these drugs highly attractive as they can be used even in remote-peripheral centers, where the need for rapid schizonticidal drugs is the greatest. In contrast, intravenous quinine infusion is difficult to institute, needs constant monitoring (for arrhythmia and hypoglycemia). However, due to greater experience with quinine, it still retains its place as the mainstay of therapy for severe malaria in most parts of the world. A loading dose of 20mg/kg is infused in 5% dextrose or dextrose saline over a period of four hours to be followed by 10mg/kg eight-hourly for the first 48h. If there is no clinical improvement after 48h of parenteral therapy, the maintenance dose of parenteral quinine should be reduced by one-third to one half (i.e., 5-7mg quinine dihydrochloride).[3] Total daily dose of quinine in patients requiring parenteral therapy beyond 48h is as follows: Day 0: (first day of treatment) 30-40mg salt/kg of body weight Some physicians prefer to use a continuous infusion and prepare the day′s quinine in a single graduated infusion bag or bottle. For smaller children one should use a micro-drop chamber or infusion pump for administering quinine infusion. As soon as the patient is able to take orally oral quinine therapy (10 mg/kg body weight three times a day) should be instituted. The total duration of therapy is for seven days. Intravenous quinine should be administered at recommended dosage for first 48h even if acute renal failure (ARF) or severe jaundice is present, but subsequent doses should be reduced to half if IV infusion is necessary.[3] Quinine is not contraindicated in pregnancy. The apprehension of premature labor is ill founded. The fetal loss or distress is related to the disease rather than to quinine (in therapeutic dosage). A loading dose of quinine should not be given if (1) the patient has received quinine, quinidine or mefloquine within the preceding 12h or if prior drug intake cannot be ascertained; (2) the weight of the patient cannot be taken; (3) facilities for administering quinine infusion at a controlled rate are not available (4) facilities to treat complications of quinine therapy, if they develop, do not exist. The following parameters must be monitored when the patient is on Quinine-infusion:
Quinine can be given by IM injections in the same dosages, if it is not possible to administer IV infusion. It should be diluted in normal saline to a concentration of 60-100mg salt/ml, the dose divided equally and administered in the two anterior thighs (not in the buttocks as it could lead to development of abscess and damage the sciatic nerve).[11] Measures in the management of specific manifestations and complications of cerebral malaria Cerebral malaria is the most dreaded complication of P. falciparum malaria and is responsible for most of the malaria-related deaths. Mortality increases significantly when it is associated with other complications such as ARF, jaundice or ARDS. The components of management consist of Care of the unconscious patient Maintenance of airway, breathing and circulation (ABC), and meticulous nursing care are the basic constituents of caring for unconscious patients. Symptomatic management Fever: Anti-pyretic drugs (paracetamol), tepid sponging and fanning are employed for the management of fever. A study conducted in children from Gabon demonstrated that paracetamol was not as efficient as sponging or fanning in reducing fever in patients with prolonged parasitemia.[12] NSAIDs should be avoided as they can cause gastrointestinal bleeding. Ice-cold water should never be used for sponging as it would lead to vaso-constriction on the skin surface and the body core temperature may still remain high. Convulsions: Convulsions are seen more commonly in children. Presence of convulsions in children with malaria could be due to febrile seizures or related to more sinister cerebral malaria. Although administration of a single dose of phenobarbitone was shown to prevent seizures in these patients, it was associated with a higher mortality in Kenyan children.[13] Hence, prophylactic use of phenobarbitone is no longer advocated. Convulsions can be controlled with the use of diazepam, dilantin or paraldehyde. Slow administration of IV diazepam in a dose of 10 mg can control seizures. It can be repeated every 15 min if convulsion persists. But the total dose should not exceed 100mg in 24h. It has to be given very slowly to prevent respiratory depression. Diazepam can be given as rectal-suppository in children, as a dose of 0.5mg/kg body weight. Specific anti-malarial agents The anti-malarial drugs should be administered parenterally for decreasing and ultimately eliminating parasitemia. Quinine or Artemisinin compounds are considered the drug of choice [Table - 3]. Management of associated complications Hypoglycemia: It is an important complication of falciparum malaria. Patients most vulnerable for this complication include pregnant women (at admission or following quinine treatment), patients with severe disease (especially young children) and patients on quinine therapy. In a cerebral malaria setting, it is at times clinically difficult to differentiate between hypoglycemic coma and coma due to cerebral malaria. Intravenous infusion of 25 or 50% dextrose should be given if hypoglycemia is suspected. Plasma glucose levels should be monitored frequently in patients on quinine therapy and it should always be given with dextrose or dextrose saline.[14] Severe Anemia: Anemia of varying degree is a common accompaniment in severe malaria. Severe anemia is defined as hemoglobin concentration below 5g/dl or hematocrit below 15%. Severe life-threatening anemia is less common in adults residing in low transmission areas, though it may be seen in children. Preexistent iron deficiency may be present in many malaria patients. The signs and symptoms of anemia are dependent on the rate of fall of hemoglobin concentration. A sudden fall in hemoglobin concentration may lead to cerebral anoxia and heart failure. Indications for packed RBC transfusion include: presence of severe anemia irrespective of the presence or absence of manifestations, presence of signs of cardiac decompensation or fall of hemoglobin concentration by 20% of the within 24h. Metabolic Acidosis: Metabolic acidosis results from loss of bicarbonate and increased generation of lactic acid. Tissue hypoxia, increased body metabolism and failure of the hepatic clearance also contribute to the development of this complication. Severe metabolic acidosis may present with hyperventilation, Kussmaul′s breathing and acidotic breathing. Presence of chest signs (crepitations and/or rhonchi) is indicative of pulmonary edema/ ARDS or associated pneumonia. Estimation of blood pH and bicarbonate levels in blood will help confirm the diagnosis. Rehydrating the patient is of great value and if possible, a central venous pressure-monitoring device (CVP) should be used for guiding fluid management. Appropriate treatment of associated complications such as severe anemia and acute renal failure also help combat metabolic acidosis. Sodium bicarbonate should be administered if plasma bicarbonate level is less than 15mM/litre and blood pH is less than 7.2. Maintenance of fluid and electrolyte balance: Both hypovolemia and circulatory overload are extremely dangerous and therefore correct assessment of hydration status and management of fluid and electrolyte balance is of enormous importance. Hypovolemia is a common accompaniment in severe malaria. It may be caused by persistent fever, profuse sweating, inadequate fluid intake and in some cases due to accompanying symptoms of vomiting and loose motion. If left untreated, hypovolemia can lead to hypotension, shock and under-perfusion of vital organs: the kidneys, the brain and other vulnerable organs. It can also lead to tissue hypoxia resulting in lactic acidosis. Dehydration should be corrected with 0.9% saline or 5% dextrose saline by IV infusion. Excessive administration of isotonic dextrose solutions can induce hypo-osmolality and hyponatremia. Severe hyponatremia may lead to cerebral edema and neurological abnormalities, including seizures. Monitoring of blood pressure, urine volume and JVP should be undertaken for assessing the hydration status. Circulatory overload is extremely dangerous, as it may rapidly precipitate fatal pulmonary edema. It can result from renal failure or excessive administration of intra-venous fluids or packed cells. The usual manifestations include weight gain, bilateral basilar rales, raised JVP, dependent edema and features of pulmonary edema. Fluid intake should be drastically restricted and fluid input output chart maintained. Furosemide 40-250mg should be administered intravenously. Electrolyte Disturbances: In patients with severe malaria, hyponatremia has been attributed to inappropriate secretion of anti-diuretic hormone (SIADH). In addition, excessive losses of sodium in sweat, vomitus and diarrhea (sodium depletion) and administration of plain water orally or hypotonic solutions intravenously (′dilutional′) also contribute to the occurrence of this complication. Hyperkalemia: Impaired renal function is the major cause of hyperkalemia in patients with severe malaria and requires urgent attention. These cases should be referred to a dialysis center for further treatment. Circulatory collapse: It occurs in association with severe dehydration, algid malaria, massive gastrointestinal hemorrhage, ruptured spleen and gram-negative septicemia. The possible sites of infection could be urinary tract (especially if there is an indwelling catheter) intravenous lines, meninges and lungs. Circulatory collapse can be diagnosed when one or more of the following features are present: systolic blood pressure less than 70mmHg in supine position; cold, clammy, cyanotic skin, constricted peripheral veins and rapid and feeble pulse. Correction of hypovolemia is of utmost importance with an appropriate fluid e. g. normal saline or 5% dextrose saline. One should look meticulously for the possible sites of infection (lung, urinary tract, IV injection sites) to rule out sepsis. Appropriate specimens should be collected for culture and sensitivity test. If infection is suspected, a broad-spectrum antibiotic (3rd/4th generation Cephalosporins and amino-glycosides) can be given provided renal functions are normal. Jaundice: Mild Jaundice in malaria is mostly due to hemolysis. However, moderate to severe jaundice could result from hepatic dysfunction.[15],[16] Usually, unconjugated hyperbilirubinemia is seen without a significant (more than threefold) rise in the serum levels of hepatic transaminases. However, when hepatic dysfunction occurs, these could reach high levels. However, hepatic encephalopathy due to hepatocellular failure is rare. When jaundice is associated with cerebral malaria, it may be misdiagnosed and treated as viral hepatitis. Distinction from acute viral hepatitis is difficult if parasitemia has not been demonstrated on examination of peripheral blood smear. In endemic areas, severe malaria should be considered as a diagnostic possibility in patients presenting with altered sensorium and jaundice. Jaundice in malaria does not require any specific therapy; indirect hyperbilirubinemia due to severe hemolysis needs to be treated with packed RBC transfusion. Acute renal failure Prerenal azotemia is the most common form of acute renal failure (ARF) resulting from mild to moderate renal hypoperfusion. It is rapidly reversible upon restoration of renal blood flow. More severe hypoperfusion may lead to ischemic injury of renal parenchyma and intrinsic renal azotemia. Thus, prerenal azotemia and ischemic ARF are a part of the spectrum of manifestations of renal hypoperfusion. Acute renal failure as a complication of malaria is more common in adults than in children. Acute renal failure when present alone is less severe than when associated with other complications (cerebral malaria, jaundice, pulmonary edema/ ARDS). Malarial ARF is catabolic in type characterized by rapid rise of plasma urea and creatinine. The cause of established ARF is usually due to acute tubular necrosis. Acute renal failure is diagnosed when urine output falls below 400 ml in 24 h or 20 ml/hr and fails to respond even after rehydration. It is usually oliguric in nature. The diagnosis is confirmed by estimation of serum-creatinine. Prerenal azotemia is usually present with the signs of dehydration. Extreme caution must be taken to avoid administration of fluid, which may lead to volume overload and pulmonary edema. It is extremely difficult to distinguish between prerenal azotemia and established ARF on clinical grounds alone . It is important to differentiate between the two, from the management point of view. Measurement of urine-specific gravity (which exceeds 1020 in patients with prerenal azotemia, but is below 1010 in those with ARF) helps in making this important differentiation. The importance of monitoring and maintenance of fluid and electrolyte balance can not be overemphasized (vide supra) . Peritoneal dialysis (PD) or hemodialysis should be undertaken under the following conditions: Volume overload leading to acute pulmonary edema, severe acidosis, hyperkalemia, uremic-encephalopathy, progressive oliguria or anuria and pericarditis. In recent times, hemo-filtration has been shown to be more effective than peritoneal dialysis. It corrects acidosis and azotemia more rapidly and more completely than PD and is associated with shorter duration of treatment. Unfortunately, facilities for hemo-filtration are not available in most centers in developing countries, where malaria is highly prevalent. Pulmonary edema and ARDS Pulmonary edema is a grave complication of severe malaria with a high mortality rate. It can appear anytime during therapy. Fluid overload is an important contributory factor for the development of pulmonary edema. Adult Respiratory Distress Syndrome (ARDS) has been known to occur with normal or negative fluid balance. Increased capillary permeability is supposedly responsible for the occurrence of ARDS. Presence of ARF, severe anemia and pregnancy predispose to this complication. Increase in the respiratory rate in the absence of metabolic acidosis and anemia, is usually the first clinical manifestation pointing towards presence of pulmonary edema. Bilateral basal crepitations, raised JVP and chest radiograph demonstrating hilar congestion, bilateral diffuse infiltrations and reduced arterial pO- 2 are other obvious manifestations of pulmonary edema. Convulsions and deterioration in the level of consciousness. In most cases, it is difficult to differentiate between pulmonary edema and ARDS. Monitoring the central venous pressure helps prevent pulmonary edema. Once it occurs the patient should be propped up at 45 0sub and should receive high concentration of oxygen. Injection furesamide in incremental doses should be given. The most effective way to reduce volume overload is to venesect the patient and remove about 250ml of blood into a blood transfusion donor bag.[3] Patients with ARDS should be mechanically ventilated with PEEP (Positive End Expiratory Pressure), which results in adequate oxygenation and resolution of ARDS. Contributory factors like ARF and severe anemia should also be tackled by employing appropriate therapeutic measures. Corticosteroids have no role in the management of ARDS. Ancillary therapy in severe malaria Corticosteroids Recommended in the past, dexamethasone and other corticosteroids fell into disrepute, following trials that showed no benefits in terms of improved survival of patients with cerebral malaria.[17],[18] Steroid use is also associated with side-effects such as GI bleed and increased susceptibility to infection. Corticosteroids could make a comeback following the results of recent studies from Kenya that showed the presence of raised intracranial pressure (ICP) in African children with malaria.[19] This evidence may give fillip to the use of corticosteroids in patients with cerebral edema.[20] Flemming et al showed that corticosteroids control hemolysis in Black-water Fever.[21] However, the study suffered from a few drawbacks: the subjects were not adequately defined and the study did not have a control group for comparison. The role of high-dose corticosteroid therapy (Methylprednisolone 30mg/kg) in the management of gram-negative bacterial sepsis and ARDS is still controversial.[22],[23] In view of these findings, corticosteroids probably do not have a role in the management of ARDS associated with severe malaria. Till large controlled randomized trials confirm their role, corticosteroids do not constitute a recommended therapy for cerebral malaria, ARDS and massive hemolysis (Black-water Fever). Osmotic diuretics Mannitol and urea have been used in the treatment of so-called cerebral edema in cerebral malaria. But the results are unconvincing and the drugs could lead to dilutional hyponatremia and volume overload.[24],[25] Many authors, in fact, question the notion of occurrence of cerebral edema in patients with cerebral malaria.[26] Newton et al monitored intracranial pressure in patients with cerebral malaria and demonstrated that mannitol was able to reduce moderate rise in ICP, but was ineffective in severe raised ICP.[27] The WHO does not approve of mannitol therapy in cerebral malaria.[3] Its use is contraindicated in patients with ARF or pulmonary edema. Pentoxyfylline Pentoxyfylline, a phospho-diesterase inhibitor, inhibits TNF synthesis and increases intracellular Cyclic-AMP (Adenosine mono-phosphate). It has been shown to reduce circulating TNF and IL-6 and produce clinical improvement in severe falciparum malaria.[27],[28],[29],[30],[31] There are conflicting reports about its role in cerebral malaria. In a small randomized trial in children in Burundi, Pentoxyfylline appeared to reduce the duration of coma from a median 48h to six hours.[29] While a study from Thailand didn′t prove to be effective,[30] a recent trial of this drug was reported to be effective in Indian adults with cerebral malaria.[31] At present the drug is not recommended for use.[3] Dextran It was postulated that Dextran, through its effects of reducing the blood viscosity, would help improve blood flow through the small cerebral vessels. However, patients of severe malaria are mostly anemic and have reduced blood viscosity, anyway. Dextran sometimes causes anaphylactic reactions and can predispose to severe bleeding diathesis.[32] Hence it is not recommended in patients with severe malaria.[3] Iron chelators An iron chelator like desferrioxamine B could be expected to have an anti-malarial activity through its action of withholding iron from the parasite, an element crucial for its metabolic pathways. In addition, it inhibits iron-induced peroxidant damage to cells and subcellular structures.[33] This could be another beneficial effect for patients with severe falciparum malaria. Results of a study done in Zambian children suggest that desferrioxamine B produced a significant reduction in the duration of coma (from a median 68.2h to a median of 24.1h).[33] However, a subsequent study carried out in children failed to show any beneficial effect of desferrioxamine B on the duration of coma recovery but was, in fact, associated with increased mortality rate (P=0.05).[34] A study from India has also showed that use of oral iron chelator deferiprone was associated with a beneficial effect (reduction in coma recovery time) in patients of cerebral malaria.[35] At present there is no sufficient evidence to indicate the usefulness of iron chelators in the management of severe malaria.[3] Exchange transfusion Patients with high malarial parasitemia have increased risk of developing complications.[36] Therefore, it has been suggested that exchange blood transfusion may benefit some patients with heavy parasitemia. The rationale for exchange transfusion is obvious: it would remove infected red cells from the circulation and reduce the parasitemia; it would provide healthy un-parasitized RBCs with normal mechanical properties and would also correct anemia. It has been used in many centers but there is no consensus about its beneficial effects. Although a study demonstrated that exchange transfusion was associated with reduction of parasitemia to the tune of 50% when 70% of the circulating volume was exchanged,[37] many ascribed this reduction to the use of potent anti-malarial drugs like quinine, which reduce parasitemia by 50% in 24h. The infrastructure of blood banking and safe blood (hepatitis- and HIV-free) are not widely available in areas where malaria is rampant. At present time, data from powerful, adequately designed randomized control studies is not available to recommend this modality as an ancillary therapy.[38] References
Copyright 2006 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp06095t3.jpg] [jp06095t2.jpg] [jp06095t1.jpg] |
| |||||||||

{kind=link}
{kind=link}