 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
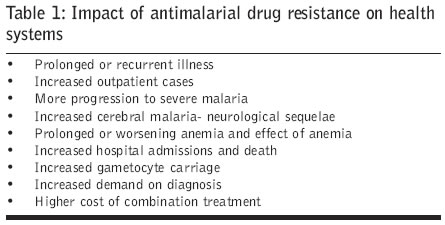
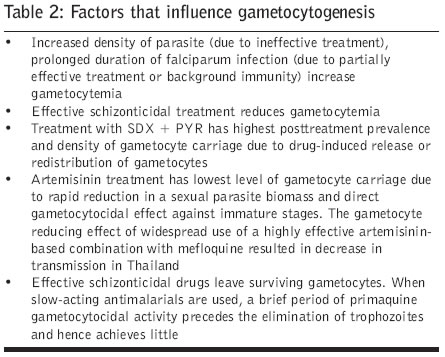
Journal of Postgraduate Medicine, Vol. 52, No. 4, October-December, 2006, pp. 291-293 Symposium Malaria: Antimalarial resistance and policy ramificationsand challenges Kshirsagar NA Department of Clinical Pharmacology, Seth G S Medical College and KEM Hospital, Parel Mumbai - 400012 Date of Submission: 31-Jul-2006 Code Number: jp06097 Abstract ′The National health Policy 2002" of India and the "Roll Back Malaria" policy makers have set up an ambitious goal of reducing malaria mortality and morbidity by 25% by 2007, and by 50% by 2010. To achieve these goals, problems should be identified, available evidence analyzed and policy should be changed early. Infection with drug resistant malarial parasites has a tremendous impact on health (prolonged recurrent illness, increased hospital admissions and death), health system (higher cost of treatment) and socioeconomics of the region. In view of the evidence of the economic burden of malaria, it has been suggested that second line treatment could be considered at 10% failure instead of 25%. Effective schizonticidal drugs will not only reduce morbidity and mortality but will also reduce transmission. Studies have shown that prevalence of viable (as tested by exflagellation test) gametocytes is considerably more after the Chloroquine or Chloroquine + Sulphadoxine-Pyrimethamine treatment compared to Quinine. Unfortunately, the only gametocytocidal drug for Plasmodium falciparum, primaquine, is also loosing its efficacy. 45 mg Primaquine reduces gametocyte prevalence by 50% while a new drug, 75 mg bulaquine or 60 mg primaquine reduces it by 90%. Plasmodium vivax forms 60-70% of malaria cases in India. Relapses which occur in 10-20% of cases adds to the burden. Efficacy, as confirmed by Polymerase Chain Reaction-Single Strand Conformational Polymorphism (PCRSSCP) to differentiate relapse and re-infection, of standard dose of primaquine (15 mg/day for 5 days, even 15 mg/day for 14 days) for vivax malaria is reducing. Fourteen day treatment is also impractical as compliance is poor. Newer drugs, newer drug delivery systems are thus needed. Slow release formulations with blood levels maintained for one week may be useful. Rationale of giving primaquine in higher doses and different timing need to be considered. The genome of Plasmodium falciparum and genome of Anopheles gambiae have been unraveled in last past 3 years. This has given us an opportunity to develop new tools. Whatever be the tool, educating health care workers as well as lay public and ensuring appropriate use of available drug are essential to achieve our goals of controlling malaria.Keywords: Tropical disease, Infection, Schizonticidal, Gametocytocidal, Antirelapse, Bulaquine, Mumbai, India Malaria is one of most ancient diseases of humans and has influenced human evolution and history. Though the malaria parasite cycle was discovered in 1897 and the concept of eradication was adopted by the WHO in 1955, malaria continues to remain a major health problem. Most estimates suggest the global annual estimate of 300-500 million clinical cases of malaria and mortality in the range of 1-2 million is reported.[1] Malaria infection in pregnancy accounts for 25% of all cases of severe maternal anemia and 10-20% of low birth weights. Malaria reduces attendance at school, productivity at work, impairs intellectual development. Cerebral malaria can result in persisting developmental abnormalities. The economic effect of malaria is immense and the disease is estimated to cost US $12 billion in Africa alone. There have been several international initiatives to combat malaria. Roll Back Malaria was launched in 1998 by WHO, UNICEF, UNDP and the World Bank to provide and coordinate an international approach with a goal of halving the burden by 2010. Its strategy includes prompt treatment with effective drugs, effective use of insecticides-treated material, other vector control methods, intermittent preventive treatment in pregnancy and emergency epidemic preparedness and response. Unfortunately, at the halfway mark in 2005, in fact malaria morbidity and mortality increased significantly globally. The situation has deteriorated, especially in sub Saharan Africa,[2] due to many reasons, such as global warming, droughts, floods, travel, civil disturbances and HIV infection. HIV increases malaria fevers and interacts adversely with malaria during pregnancy. However, the main cause of the worsened malaria situation has been the spread of the drug-resistant parasite which has led to increasing malaria-associated morbidity and mortality. Antimalarial Drug Resistance - Impact on Health Antimalarial resistance results in enormous public health burden because of prolonged or recurrent illness and progression to severe malaria which is associated with increased hospitalization and death. Even lower levels of resistance which cause recrudescence of infection are associated with return of illness, prolonged or worsening anemia and increased gametocyte carriage which fuels transmission, particularly of the resistant parasite and a higher risk of treatment failure in subsequent infections. Impact of drug resistance is more in areas of low transmission where diagnostic facilities and infrastructure are inadequate and resources not allocated to respond to a sudden increase in treatment needs. [Table - 1] gives the impact of antimalarial drug resistance on health.Malaria in Mumbai In Mumbai (a metropolitan city on the west coast of India), malaria was well controlled until 1990. However from 1991, there has been a resurgence. Increase in mosquito breeding sites, high-rise buildings, migrant population are important reasons. However, resistance to drugs and treatment failure are also important contributing factors. P. falciparum asexual stage resistance to drugs In 1993, a single dose of chloroquine (CQ) was ineffective in 35% P. falciparum cases. By 1996, chloroquine resistance increased to alarming proportions in the city as also resistance to sulphadoxine + pyrimethamine (SDX +PYR). In vitro testing also demonstrated CQ resistance.[3] The result of all this is continued malaria cases in Mumbai. In low transmission areas, as in Mumbai, the effect of resistance (ineffective or partially effective treatment) is an increase in acute manifestations and resistance is rapidly propagated due to high drug pressure on the existing parasite population. In high transmission areas, the clinical effects are prolonged / chronic infections with increasing risk of severe anemia. A two to eleven-fold increase in malaria-associated mortality among children in Africa is seen when resistance develops and spreads. It is therefore, now felt that change in treatment policy should be considered after 10% failure rate. Previously this was 25%. In our study comparing the efficacy of treatment with CQ, Mefloquine (Mf) and Co-artemether, we compared the cost of treatment. The difference in the cost of treating with chloroquine or mefloquine was Rs. 100 per patient. While the cost of treatment of RII, RIII was over Rs. 1000 per patient. Thus the cost of treating 10 RII, RIII cases was more than treating all 100 patient with 2nd line drug.[4] Thus change to 2nd line seems appropriate when RII, RIII resistance is more than 10% rather than the currently recommended 25% (on the basis of even cost of treatment). Artemisinin-based combination therapies (ACT) are currently the best antimalarials available. While 43 countries have adopted ACT, there are difficulties and challenges of cost, inappropriate drug use, limited knowledge on safety, lack of pharmacovigilance and lack of suitable drug formulations. Operational research is needed for the implementation or for delivery of ACT beyond the formal health facility setting, case management and use of diagnostics, monitoring and evaluation. Thus the policy for P. falciparum in Mumbai should include continuous surveillance for drug resistance; presumptive treatment, if given, should be full dose Chloroquine (25 mg/kg over three days) and early diagnosis should be ensured. Sexual stage (P. falciparum gametocyte) drug resistance Although the elimination of the asexual stages of P. falciparum is the focus of treatment of individual symptomatic patients, at the population level, reducing the carriage of gametocytes is necessary to limit transmission. Gametocyte biology The process of sexual differentiation and development can be subdivided into steps of induction, commitment and progression through various maturation stages, but its molecular basis is unknown (how merozoites after invading red cells develop into gametocytes is unclear). In Stages 1-3, the sexual parasites are sequestered in capillaries and are potentially susceptible to drugs acting on the asexual stage. In Stage 4 parasite re-enters circulation. (Artemisinin derivatives act on this stage also.) Stage 5 gametocytes circulate and only 8 aminoquinolines (Primaquine) are effective on this stage. A wave of gametocytes appear 6-10 days after the appearance of the asexual stage and symptoms. In a patient with inadequate / ineffective schizonticidal drugs, gametocytes reappear in the blood at a later stage and cause transmission. [Table - 2] gives the factors which influence gametocytogenesis. Gametocytocidal effect of primaquine (PQ) and Bulaquine / Elubaquine (BQ) Our studies in Mumbai showed that over 25% patients had gametocytes on admission. Without Primaquine, patients treated with CQ or CQ+SP (parasites sensitive to CQ or CQ + SP) had viable gametocytes up to Day 29.[5] Treatment with single dose of 45 mg PQ, given on Day 4, reduced the prevalence of gametocytes by approximately 70%. Bulaquine (Elubaquine) is a new drug (formerly called CDRI 80/53) developed by the Central Drug Research Institute (CDRI), Lucknow, India and marketed in India by Nicholas Piramal.[6] In a study comparing the gametocytocidal effect of BQ (75 mg single dose) vs. PQ (45 mg single dose), in uncomplicated falciparum malaria patients receiving combination of quinine (30 mg/kg/day) + doxycycline (100 mg/day) x seven days, of the patients who received PQ (45 mg single dose on day 4) 77% were found gametocytemic on day 8, while among patients receiving BQ (single, 75 mg dose on day 4) only 11% were found gametocytaemic on day 8.[7] The current ongoing study comparing higher dose of PQ (single dose 60 mg) with that of BQ (single dose 75 mg) and standard 45 mg PQ dose, given on day 4, has shown that the prevalence of gametocytemia reduced by 90% in both uncomplicated and severe malaria on day 8 in two of the groups treated with 75 mg BQ and 60 mg PQ while with 45 mg primaquine, it reduced only by 55%. Thus, the present recommendation of 45 mg primaquine is only 50-70% effective, there is a need to review the gametocytocidal policy. Drug resistance in P. vivax P. vivax is pantropical but is largely absent from Africa (Black Africans lack the erythrocyte surface protein called Duffy factor that P. vivax merozoites require for invasion). P. vivax pattern and probability of relapse varies by geographic region. In temperate regions relapses occur at long intervals (> six months) with the tropical chesson strain, relapses occur sooner, are typically multiple. In India 60-70% of cases of malaria are P. vivax . Chloroquine resistance has been identified in P. vivax worldwide. Recurrence with presumptive single dose chloroquine treatment is 5% while with total dose 25 mg/kg it is 1-2%.[8] Thus monitoring of P. vivax for chloroquine resistance should be done at a few centers. For preventing relapse, the National Anti Malaria Program (NAMP) recommends five-day primaquine therapy. However, in our studies in Mumbai, we noted that the response to five-day therapy has declined.[9],[10] Similar results are seen in various parts of the India. In Pakistan too, the efficacy of five-day primaquine has declined.[11],[12],[13],[14],[15] Alarmingly, we found decline in the efficacy of 14-day PQ treatment as well, as confirmed by the polymerase chain reaction -single strand conformational polymorphism analysis (genotyping technique used to distinguish relapse and re-infection).[16] Unfortunately, due to G6PD deficiency prevalence, 14-day treatment is not recommended for widespread use. Thus, in vivax malaria, the antirelapse policy needs to be revised. Without primaquine, over a six month-follow-up, relapses occur in 10-20% cases. Thus, we could consider no antirelapse treatment after the initial attack, followed by 14 days primaquine in case of recurrence of vivax malaria using simple G6PD tools. Conclusion To combat and control malaria, in addition to vector control measures, surveillance for drug resistance and a drug policy that is based on surveillance data, development of simple, inexpensive diagnostic tests, new drugs, drug combinations and drug delivery systems and operational research are needed.References
Copyright 2006 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp06097t2.jpg] [jp06097t1.jpg] |
| |||||||||

{kind=link}
{kind=link}