 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 52, No. 4, October-December, 2006, pp. 308-311 Grand Round Case A middle aged man with acute onset quadriparesis: A diagnostic exercise Kumar N, Choudhary N, Kaul B, Ahlawat SR Department of Medicine, Maulana Azad Medical College and Assoc LN Hospitals, New Delhi Date of Submission: 06-Jun-2006 Code Number: jp06105 A 50-year-old male farmer presented with the first episode of sudden onset weakness involving all four limbs simultaneously for the last 8 hours. There were no sensory symptoms. The patient was a chronic smoker (two cigarettes/d) for the past 20 years. There was no family history of similar episodes. His pulse rate was 88/min, blood pressure 150/90mm Hg and respiratory rate 20/min. General examination showed minimal bilateral pedal edema and grayish pigmentation over face, knuckles and palmar creases with no evidence of clubbing [Figure - 1][Figure - 2]. Abnormal findings on the nervous system examination included flaccid quadriparesis (power grade 2/5 in proximal muscles and 3/5 in distal muscles of the upper and lower limbs) with deep tendon reflexes and plantar reflexes being not elicitable. What are the possible differential diagnoses for this condition? The initial differential diagnosis of acute onset quadriparesis without alteration of sensorium or sensory or bladder-bowel affection would include:
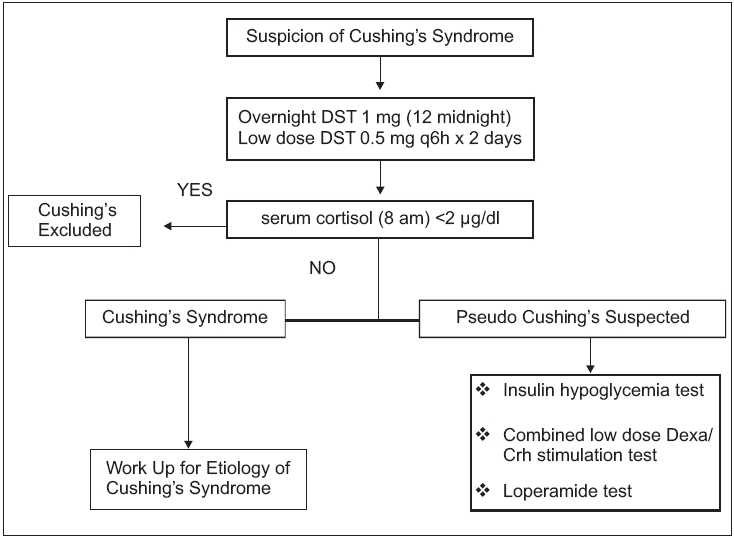
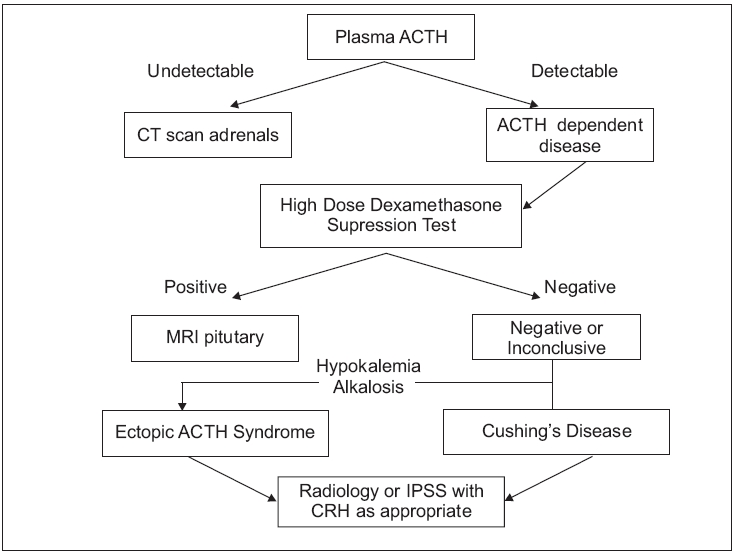
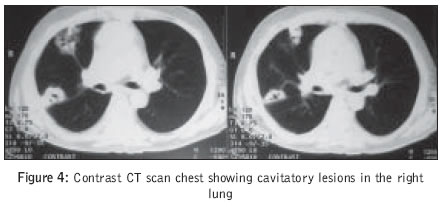
What would be the stepwise approach for management of this patient in the emergency? Respiratory pump failure indicated by a low arterial oxygen saturation and falling single breath counts (normal>30) should be determined on priority. It could occur suddenly even in apparently stable patients, hence close observation is necessary. Rapid respiratory paralysis is more commonly encountered in snake bite, GBS, ascending myelitis and hypokalemic periodic paralysis. In an alert patient with flaccid quadriparesis and no upper motor neuron signs, initial laboratory evaluation should include determination of serum electrolyte levels (Na, K, Ca, Mg, PO 4sub ), as these derangements are often readily correctable. Dyselectrolytemias can also produce ECG changes and cardiac rhythm abnormalities. If electrolytes are normal, further testing should be on the lines of the other diagnostic possibilities entertained: Electromyography (EMG) or nerve conduction velocity (NCV) study and lumbar puncture for suspected GBS; cervical cord MRI for lesions in the CNS, repetitive nerve conduction study for myasthenia and muscle enzymes for myopathy. Myasthenic weakness responds well to edrophonium/ neostigmine and this could be used as a diagnostic tool. In a stuporous patient, evaluation begins with brain imaging. It is pertinent to mention here that tests are not infallible. In its initial stages, GBS can have a normal EMG/ NCV report and no abnormal cerebrospinal fluid findings. Hence if suspicion is high, IV immunoglobulin should be started empirically. Hypokalemic periodic paralysis can occasionally present with near normal S. K+ levels. Hence this possibility should be kept high in adolescents presenting with recurrent episode of quadriparesis, especially precipitated by a high carbohydrate diet or strenuous exercise. Reports of other investigations were as follows: Hb 10.8 g/dl, Total leukocyte count 9400/mm 3sub with a differential count showing polymorphic predominance (P 76 L 20 M 2 E 2 ), ESR 23 mm at the end of 1 hr, Random Blood Sugar (RBS) level 198 mg/dl, S. creatinine 0.7 mg/dl, S. sodium 136 meq/L, S. potassium 1.9 meq/L. ABG showed mixed metabolic and respiratory alkalosis (pH 7.53, serum bicarbonate 29.7, pCO 2 38, sPO 2 96.8%). ECG showed T wave flattening. Patient was managed with intravenous potassium replacement with near complete recovery of muscle power by the next day. Despite providing oral potassium supplementation subsequently, patient′s serum potassium levels remained depressed even after 3-4 days of therapy. Alkalosis persisted, too. The appropriate response to renal K+ secretion is to excrete less than 15 mmol/d of K+ in the urine. A rapid and simple test designed to evaluate the driving force for net K+ secretion is the transtubular K+ concentration gradient (TTKG). The TTKG is the ratio of the K+ concentration in the lumen of the collecting duct to that in peri-tubular capillaries or plasma. Hypokalemia with a TTKG greater than 4 suggests renal K+ loss due to increased distal K+ secretion. Are there any clues to explain the persistent hypokalemia in this patient? Persistent hypokalemia despite adequate oral potassium supplementation is indicative of GI/ renal loss of potassium. This is especially true in a if patient without pre-existing renal disease, who is not receiving diuretics or drugs like amphotericin. Persistent renal potassium loss is seen with hyperaldosteronism (primary/ secondary) or Cushing′s syndrome. Other rare causes include renal tubular acidosis (type 1 and 2), metabolic acidosis, Liddle′s syndrome and Bartter′s syndrome. It would be noticed that the patient has peripheral edema, diabetes, hypertension, metabolic acidosis and skin pigmentation in a peculiar distribution. In endocrinological causes of hyperpigmentation, the darkening of the skin may be of equal intensity over the entire body or may be accentuated in sun-exposed areas, palmar creases, sites of friction, scars and oral mucosa. Hence, Cushing′s syndrome could be considered as a likely cause of hypokalemia. Edema is not seen in Conn′s syndrome. Secondary hyperaldosteronism from a high renin state is another possibility. How do we prove the presence of Cushing′s syndrome? A simplified flow chart depicts the steps in investigating for the presence of Cushing′s syndrome [Chart 1]. The appropriate screening test is an overnight dexamethasone suppression test (DST) or low dose DST. Serum cortisol level less than 2 µg/dl virtually excludes Cushing′s.[1] Pseudo-Cushing′s syndrome is seen in depressed patients and if strongly suspected should be worked up as depicted in the flowchart. Demonstrating loss of circadian rhythm of plasma cortisol and elevated urinary free cortisol levels are alternate screening tests but have no specific advantage over the dexamethasone suppression tests.[2] In our patient, an overnight dexamethasone suppression test (with 1 mg dexamethasone) showed a serum cortisol level (8 AM) of 58 µg/dl. How would you determine the etiology for Cushing′s syndrome in the patient? The work up is indicated in the flowchart [Chart 2]. ACTH levels are the starting point in detecting etiology of Cushing′s. The best time to measure ACTH is between 11 PM and 1 AM.[3] High dose DST involves administering 2 mg dexamethasone q6h for 48 hours; a> 50% reduction in plasma cortisol defines a positive response. An important caveat here is that a positive test occurs in 10% of patients with ectopic ACTH syndrome (so called occult ectopic corticotrophin syndrome). Plasma ACTH level was 350 pg/ml (normal< 46 pg/ml). Serum cortisol level after dexamethasone suppression (2 mg dexamethasone 6 hourly for 2 days) was 49 µd/dl. The very high levels of serum cortisol, non suppressibility by steroids and associated hypokalemia and metabolic alkalosis suggested an ectopic ACTH producing neoplasm. What could be the possible primary tumor in this patient? Etiologies for ectopic ACTH tumors include small cell cancer lung 45%, thymic carcinoid 15%, bronchial carcinoid 10%, islet cell tumors 10%, other carcinoids 5%, pheochromocytomas 2% and ovarian adenocarcinomas 1%.[4] The most common primary site of such a tumor is the chest, hence imaging of the chest is the appropriate initial approach. A chest radiograph showed right lower zone consolidation with widening of superior mediastinum. CT scan chest and abdomen showed a heterogeneously enhancing mass (7.6 x 4.5 x 8.4 cm) in the anterior mediastinum with multiple cavitatory lesions in right upper lobe and posterior basal segment of right lower lobe with bilateral enlarged adrenals [Figure - 3][Figure - 4]. CT head showed normal pituitary fossa and brain parenchyma. CT guided biopsy showed a round cell tumor expressing epithelial membrane antigen and cytokeratin and negative for leukocyte common antigen, chromogranin and S-100 [Figure - 5][Figure - 6]; suggestive of small cell carcinoma lung (WHO intermediate type). A final diagnosis of small cell carcinoma lung (SCLC) with ectopic corticotropin syndrome presenting as hypokalemic paralysis was made. Patient was treated with combination chemotherapy with cyclophosphamide, doxorubicin and vincristine while ketoconazole 400 mg twice daily was added for his endocrine manifestations. However, two weeks later he developed massive hemoptysis and expired thereafter. What is the usual presentation of the ectopic ACTH syndrome? The ectopic corticotropin syndrome (tumor producing ACTH) accounts for 10-20% cases of Cushing′s syndrome.[5] The typical presentation is as a sudden onset and rapidly progressing Cushing′s. Generally hypertension, hypokalemia, glucose intolerance and edema the presenting features. The classic Cushing′s habitus, hirsutism etc are usually not seen with rapidly growing tumors.[4] Hypokalemia is probably the most consistent finding in ectopic Cushing′s syndrome (80-100% cases). Hypokalemia is due to the very high cortisol levels that overwhelm the 11β hydroxysteroid dehydrogenase enzyme in renal tubules which is responsible for inactivation of cortisol.[6] In a patient with malignancy and clinical features suggestive of ectopic corticotropin syndrome, demonstration of non-suppressible hypercortisolism by dexamethasone suppression tests usually suffices to make the diagnosis. [4]Non suppressibility is due to the reduced sensitivity of the pre-opio melanocortin gene (POMC) ex-pression to inhibition by glucocorticoids in these cell lines. Rarely, some tumors may show suppression of corticotropin secretion by dexamethasone administration. In such cases, the definitive study for distinguishing pituitary from non-pi-tuitary forms of hypercortisolism is inferior petrosal sinus sam-pling with administration of CRH.[7] Does the development of Cushing′s syndrome influence the prognosis of these patients? The development of Cushing′s syndrome in SCLC is correlated with poor treatment response and shortened survival.[8] Increased serum levels of ACTH can be detected in up to 50% of patients with lung cancer, but Cushing′s syndrome develops in only 5% of patients with SCLC.[9] What are the learning points derived from this case?
References
Copyright 2006 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp06105c2.jpg] [jp06105c1.jpg] [jp06105f4.jpg] [jp06105f7.jpg] [jp06105f1.jpg] [jp06105f5.jpg] [jp06105f3.jpg] [jp06105f6.jpg] [jp06105f2.jpg] [jp06105f8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}