 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
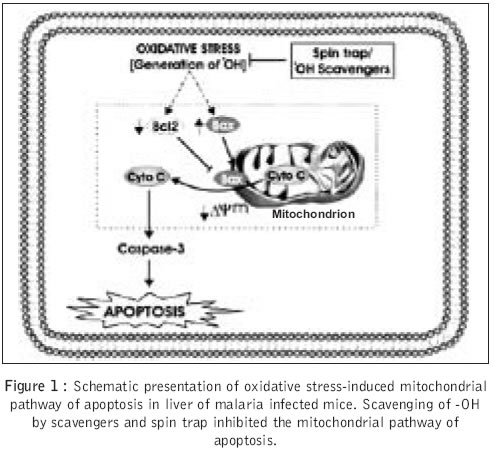
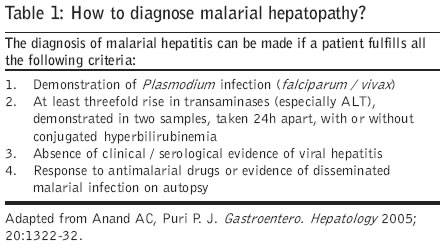
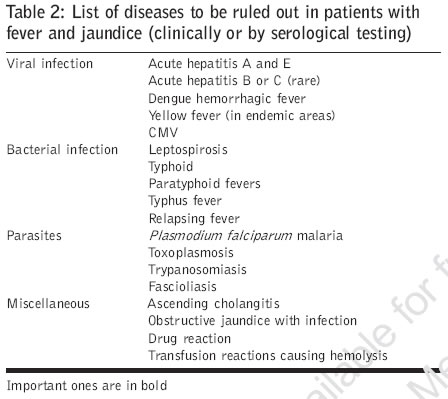
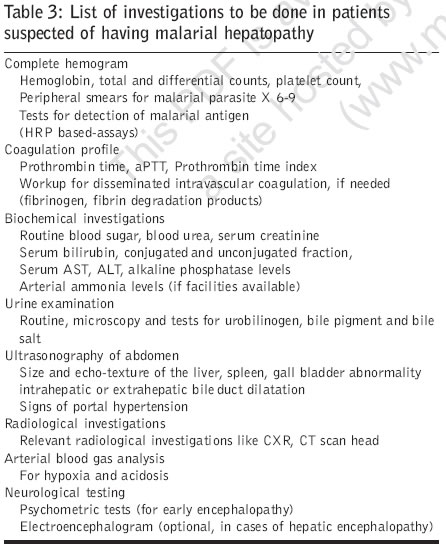
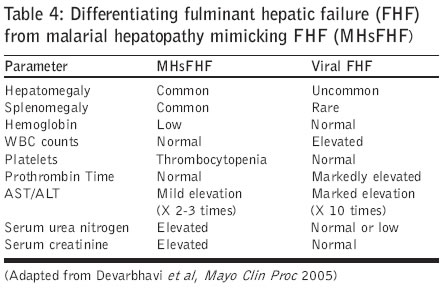
Journal of Postgraduate Medicine, Vol. 52, No. 4, October-December, 2006, pp. 315-320 Review Article Malarial hepatopathy Bhalla A, Suri V, Singh V Department of Internal Medicine, Post Graduate Institute of Medical Education and Research, Chandigarh - 160012 Date of Submission: 22-Nov-2005 Code Number: jp06108 Abstract Jaundice is a common clinical presentation in severe malaria, seen in approximately 2.5% patients with falciparuminfection but hepatitis is unusual. Although hepatic dysfunction is unusual and hepatic encephalopathy is almostnever seen in malaria, yet, cases of hepatic dysfunction are being increasingly reported in patients with P.falciparum infection, from different parts of world. The extent of hepatocellular dysfunction varies from mildabnormalities in liver function tests to hepatic failure. Patients with hepatocellular dysfunction in malaria aremore prone to develop complications, but have a favorable outcome if hepatic involvement is recognized earlyand managed properly. It is important to meticulously look for hepatic dysfunction in patients with severemalaria, distinguish it from fulminant hepatic failure and manage it aggressively.Keywords: Fulminant hepatic failure, malaria, malarial hepatitis, P. falciparum infection Hepatic dysfunction in malaria has been known since many years[1],[2] but hepatic encephalopathy is unusual. There has been tremendous increase in our knowledge of hepatocyte dysfunction occurring in malaria; hence more cases are being reported from different parts of world. A literature search was carried out on the Pubmed and all the relevant and recent literature on the subject was collected for a comprehensive review of the subject. According to world health organization (WHO), apart from jaundice, signs of hepatic dysfunction are unusual. In recent years, there has been increasing number of reports favoring existence of malarial hepatopathy, from Asian countries, especially form India.[3] The majority of the cases have either isolated infection with P. falciparum[4],[5],[6],[7],[8],[9],[10],[11],[12] or a mixed infection with both P. falciparum and P. vivax .[13] The extent of liver involvement varies from a minimal abnormality in liver function tests to hepatic encephalopathy.[13],[14],[15] Jaundice in Malaria In patients with severe malarial infection, the incidence of jaundice is reported to be 2.58% only.[16] Jaundice can result from either severe hemolysis or hepatic involvement. The rupture of hepatocytes during the primary schizogony results in cellular damage but this does not result in significant hepatic dysfunction.[17] Severe infestation of the red blood cells by P. falciparum and resultant hemolysis results in the rising bilirubin. Sequestration of the parasite-infested red blood cells in the capillaries causes clogging of the capillaries in the important organs and the resultant ischemia can lead to organ system dysfunction. When the same happens in the liver capillaries, hepatic dysfunction ensues. Hemolysis significantly contributes to the rising bilirubin in severe malarial infection. The parasite, especially P. falciparum, infects a large number of cells which are then destroyed in the spleen, resulting in hemolytic anemia. This is characterized by elevated serum bilirubin (dominant unconjugated fraction), without any significant elevation of the liver enzymes."Malarial hepatitis" is a term commonly used to describe hepatocytic dysfunction in severe and complicated malaria; however, actual inflammation of the liver parenchyma is almost never seen.[17] Malarial hepatitis is characterized by a rise in serum bilirubin along with the rise in serum glutamate pyruvate transaminase levels to more than three times the upper limit of normal.[10] This in the absence of evidence of exposure to hepatotoxic drugs and absence of clinical or serological evidence of viral hepatitis makes malarial hepatopathy a unique entity. Literature on the hepatic involvement in malaria has largely shown severe infection with P. falciparum infection. There have been occasional reports of mixed infection with P. vivax[13] and hepatitis E[18] along with P. falciparum , resulting in malarial hepatitis. The incidence of jaundice and hepatitis in patients with P. falciparum infection is variable. In a study of the 732 adult patients with falciparum malaria, only 39 (5.3%) were noted to have jaundice and only 18 (2.45%) had evidence of malarial hepatitis.[10] In another study by Murthy et al, out of the 95 patients admitted with falciparum malaria, 62% had jaundice but only 21% had evidence of malarial hepatitis.[8] In a study of 121 cases of malarial infection from Poland, about 37% of the patients demonstrated symptoms of hepatic parenchymal dysfunction.[19] In adults, the reported incidence of hyperbilirubinemia in severe malaria varies from 32-37%. In the majority of the cases it is predominantly unconjugated hyperbilirubinemia.[9],[20] Malarial hepatitis is also common in children during the course of severe infection and the incidence is reported to vary from 8%[21] to as high as 32%.[6] Although jaundice is commonly seen with falciparum infection, it is also reported with P. vivax infection and the incidence ranges from 0-9%;[22],[23],[24] however, hepatic involvement has not been described with it. The wide variation in reports of jaundice and hepatocellular dysfunctions in severe malarial infection may be due to the geographic conditions, endemicity of malaria in the region from where the reports have originated, the age groups studied, the epidemic form of infections reported and coexistent viral hepatitis or helmenthic infections endemic to that particular area.[17] The centers having tertiary care facilities are likely to see more sick patients and hence report higher incidence of organ dysfunction in severe and complicated malaria. Pathophysiology P. falciparum can invade red cells of all ages, thus enabling high levels of parasitemia to develop. The parasite index (number of parasitized RBCs / total number of RBCs) at times can be greater than 50%, in very severe infections. The risk of severe disease is highest among nonimmune individuals, among children less than five years old and among pregnant women. Clearance of a large number of parasitized red cells by spleen, rupture of the parasitized RBCs to release merozoites can lead to severe anemia and hyperbilirubinemia. P. falciparum has additional unique characteristics; as the parasites mature within red blood cells they induce the formation of sticky knobs on the surface of the erythrocytes.[25],[26] These knobs bind to receptors on endothelial cells in capillaries and venules. The cytoadherence and sequestration of red cells within these small vessels leads to microvascular pathology and obstruction to blood flow. Infected red cells also stick to uninfected red cells and form rosettes which clog the microcirculation. Ultimately, secondary liver cell dysfunction occurs due to resultant ischemia due to microcirculatory changes. This is also responsible for other severe complications, manifesting as organ system dysfunction, in the host. Micro occlusion of portal venous branches by parasitized red blood cells,[27] endotoxemia due to severe systemic infection,[28] intrahepatic cholestatsis due to reticuloendothelial blockage and hepatic microvillus dysfunction[29] could also contribute to the hepatocellular damage seen in severe malarial infection. Recently, the role of apoptosis and oxidative stress in hepatic damage due to malarial infection has been highlighted in an Indian study. Apoptosis in the hepatocyte has been demonstrated by TUNEL assay and Capsase-3 activation in this study. The authors have demonstrated a significant downregulation of Bcl -2 and upregulation of Bax expression (RT-PCR and confocal microscopy). It has been proposed that malarial infection in the liver induces generation of hydroxyl radical (OH) which triggers oxidative stress-induced mitochondrial pathway of apoptosis[30] [Figure - 1]. Finally, we can conclude that a host of factors are responsible for the hepatic dysfunction in severe malarial infection. This does not appear to be due to direct inflammation of hepatocytes but due to failure of bilirubin excretion due to heavy parasitemia, endotoxemia, ischemia, acidosis or a combination of some or all of these factors.[17] Other causes of jaundice in malaria could be coexistent viral hepatitis, especially infection with hepatitis E virus[31],[32] or hepatitis A virus.[33] Underlying chronic liver disease due to hepatitis B virus has been reported to be a risk factor for severe malarial infection and their coexistence may result in exaggerated hepatocyte dysfunction.[17] Disseminated intravascular coagulation may also contribute to hepatocellular dysfunction seen in severe malarial infection.[34] Although glucose 6 phosphatase deficiency (G6PD) may be protective against the development of severe malarial infection[35] malarial infection pre se[36] and / or antimalarial drugs used in these G6PD deficient patients may precipitate hemolysis and result in jaundice in these patients. In addition, liver function abnormalities have been reported with administration of mefloquine,[37] chloroguanide,[38] amodiaquine[39],[40] and pyrimethamine sulfadoxine combination.[41] Most of the literature available on hepatic dysfunction due to antimalarial drugs is with long-term prophylactic administration of these drugs but their contribution to hepatocyte dysfunction in active malarial infection is not yet established. Clinical features These patients usually present with acute onset fever along with jaundice. The jaundice can vary from being mild to severe, depending on the severity of infection. A milder form of disease manifests with fever, headache and vomiting, whereas a severe disease presents with coma, deep jaundice and renal failure and mimics fulminant hepatic failure.[10] Severe hemolysis can lead to significant anemia but in the presence of jaundice, clinical examination may be misleading and one can miss significant pallor. Systemic examination reveals hepatomegaly and significant splenomegaly. In a study on 50 cases of P. falciparum malaria with jaundice 70% presented with pallor, 56% had splenomegaly, 48% had hepatomegaly and 24% of cases presented with coma.[5] Other clinical manifestations of severe falciparum infection, like severe anemia, uremia due to renal failure, altered sensorium or coma due to hypoglycemia or severe central nervous system infestation may also be present in these patients. The clinical presentation may vary depending on the type and severity of the organ system dysfunction. Hepatic encephalopathy in severe malaria According to WHO, clinical signs of liver failure such as asterixis are almost never seen unless there is concomitant viral hepatitis.[3] Hepatic encephalopathy usually starts with alteration in sleep pattern. Milder form may manifest as altered behavior or may be detectable only on psychometric testing. Severe impairment of the sensorium is not unusual in severe malaria, however this may be multifactorial. Cerebral malaria, hypoglycemia, hypoxia and/or uremia due to renal involvement may also contribute to the altered mental status or encephalopathy in severe falciparum infection. This fact should always be borne in mind while managing patients with severe malarial infection. Although hepatic encephalopathy is considered a rare presentation of malaria, in a study of 86 adult patients having malaria with jaundice (serum bilirubin > 3 mg%), hypersomnia and inversion of the sleep rhythm and delirium were the initial manifestations. Overt evidence of hepatic encephalopathy was seen in only 15 patients. Arterial blood ammonia levels were raised in all the patients (range 120-427 meq/l) but asterixis were observed in only nine patients. However, psychometric tests were abnormal in 12 and altered mental state was seen in 13 patients.[7] Electroencephalogram (EEG) in these patients may reveal delta waves, pseudo periodic burst suppression and triphasic waves.[10] In one study, triphasic waves, which are considered characteristic of hepatic encephalopathy, were seen in three out of 15 patients having malarial hepatitis.[7] Since the EEG findings are very nonspecific and are seen in only a small number of patients, it may not be advisable to perform this investigation in all the patients suspected of having malarial hepatopathy. Laboratory findings Serum bilirubin is elevated and it is the conjugated fraction which is dominant in patients with hepatopathy.[5] Liver enzymes are elevated 2-3 times the normal but may be elevated much beyond this.[4],[5] In a study of 50 peripheral blood film confirmed cases of Plasmodium falciparum malaria with jaundice, 18 patients had serum bilirubin < 3 mg%, 20 patients had serum bilirubin between 3-10 mg% and only 12 patients had serum bilirubin values of> 10 mg%.[5] Prothrombin time is usually normal, even in patients with marked elevation of enzymes.[4],[5] Since severe coagulopathy is almost never seen in isolation with severe malaria, its presence should alert the physicians to look for an underlying infection with a hepatotropic virus or disseminated intravascular coagulation associated with sepsis. Associated abnormalities in laboratory parameters are the presence of anemia due to ongoing hemolysis, abnormal renal functions due to hemoglobinuria and respiratory distress due to capillary endothelial dysfunction. Since the patients with hepatic involvement are more prone to these complications, renal function (blood urea and serum creatinine), arterial blood gases (for hypoxia and acidosis) and coagulation parameters (to look for disseminated intravascular coagulation) should be strictly monitored, preferably daily or on a more frequent basis if required. Ultrasonography may detect hepatomegaly with or without splenic enlargement; however, there is no specific feature on sonography, except for low echogenicity, which would suggest a diagnosis of malarial hepatopathy [Table - 1]. Enlarged liver with normal architecture is the commonest finding and splenomegaly can be seen in up to 82% of patients.[7] Other findings on Ultrasonography are nonspecific with up to 16% patients having gall bladder wall thickness and 20% having renal enlargement and free fluid in peritoneum [Table - 1].[7] An effort should be made to rule out the diseases mimicking malarial hepatopathy (fever with jaundice), either clinically or by serological tests [Table - 2]. The list of investigations to look for all the complications of severe malaria is exhaustive, however, a minimum set of investigations is mandatory for working up the patients suspected of having malarial hepatopathy [Table - 3]. Histopathology The histological hallmark of malarial hepatopathy is the presence of acute injury to hepatocytes and deposition of "Malarial pigment" also known as "Hemozoin". In a study of 50 patients with proven Plasmodium falciparum malaria with jaundice, histo-pathological examination was done in 20 patients with serum bilirubin level 3-10 mg%. It showed evidence of swollen hepatocytes in 100%, malarial pigment deposition in 75%, inflammatory infiltrates in 60%, congestion of hepatocytes in 50% and associated centrizonal necrosis in 25% of cases.[5] In another study of 121 cases of malaria, histopathological examination of the liver revealed the activation of cells of the mononuclear phagocyte system, Kupffer′s cells in particular, with the presence of granules of browny-black "malarial pigment" and iron deposits.[19] The most consistent histological findings are reticuloendothelial cell hyperplasia.[42] Pigmentation in Kupffer′s cells, sinusoidal and portal infiltration, fatty change and cholestatsis are other prominent features. On electron microscopy hepatocyte swelling, Kupffer′s cell hypertrophy, sinusoidal macrophage hypertrophy along with changes in endoplasmic reticulum/mitochondria, loss of microvilli and damage to canalicular membranes is seen.[43] Parasites are demonstrated on histology in less than 50% patients. The centrizonal necrosis seen in some cases may be due to the malarial infection or accompanying sepsis / hypotension.[5] Differentiating from fulminant hepatic failure In endemic areas, severe malaria will always feature as a differential of fulminant hepatic failure. It is important to differentiate the two since the prognosis in patients with severe hepatic injury due to malarial infection is better than fulminant hepatic failure (FHF) due to other causes.[4] The pointers towards malarial etiology are persistent fever, disproportionate anemia, oligoanuria and normal or increased liver span. Laboratory parameters may also help in differentiating severe malaria from fulminant hepatic failure. The liver enzymes are mildly elevated and severe dysfunction in coagulation parameters is absent in severe malaria.[4],[10] In a study from Bangalore, 25 patients with FHF were compared with 25 patients with severe malarial hepatopathy simulating as FHF. There was no statistically significant difference in duration of jaundice, altered consciousness and the interval between onset of jaundice and altered consciousness between them. But hepatomegaly was more common with malarial infection and abnormal prothrombin time more common in patients with FHF. In endemic areas, the presence of hepatomegaly and normal prothrombin time in the setting of FHF should be considered as suggestive of malaria and a peripheral blood smear should be obtained for diagnostic confirmation[4] [Table - 4]. Management The management of malarial hepatitis is not different from the management of severe malarial infection. In endemic areas, it is important to have a high degree of suspicion of severe infection with malarial parasite presenting as acute febrile illness with hepatic dysfunction. The other conditions prevalent in tropical countries like acute viral infections leading to hepatitis, enteric fever and leptospirosis should figure in the differential diagnosis. Since the clinical presentation may not differ much, laboratory help may be needed to establish the etiology of malarial hepatitis.[4] Routine, single peripheral smear examination may not be sufficient, so repeated smears are required to pick up the diagnosis. In one study the first smear examination was able to clinch the diagnosis of severe malaria in 95% patients.[44] However, in another study of 150 patients with severe malaria, three consecutive smears done yielded diagnosis in 92.5% cases.[45] WHO recommends at least six to nine peripheral smears (thick and thin) to be examined before declaring it negative for falciparum infection.[46] Malarial antigen detection kits (Histidine rich protein II based kits) have a very high sensitivity (77-90%) and specificity (82-94%) for picking up falciparum infections.[47],[48],[49],[50] These tests are safe, cheap, reliable and can be performed bedside. Polymerase chain reaction-based techniques for identification of species is for investigative purpose and should be used only for research.[51],[52] Since the list of differential diagnoses is long, appropriate tests should be done to rule them out. Liver function tests and ultrasonography are important but liver biopsy is not indicated. Prolonged unexplained jaundice should prompt one to undertake liver biopsy.[10] Quinine is the drug of choice for management of severe falciparum malaria, however, in endemic areas, where resistance is suspected, a combination therapy may be better than single drug.[44] The hepatitis usually resolves on its own after the subsidence of fever and clearing of the parasite from the body. Since these patients are more prone to complications a careful watch is needed to identify the early signs of pulmonary edema, respiratory failure or sepsis.[8],[9] Serum bilirubin normally starts receding by 72h of starting treatment, however, it may be delayed in patients having coexisting renal dysfunction.[7] Hepatic encephalopathy, if present should be differentiated from cerebral malaria and should be managed by appropriate supportive management. Since these patients usually do not develop severe coagulation abnormalities, routine supplementation of coagulation factors is not usually needed. Presence of severe coagulation abnormalities should alert a physician for the possibility of a coexistent viral hepatitis or disseminated intravascular coagulation. Outcome in malarial hepatopathy The presence of hepatitis in patients with falciparum malaria indicates a more severe illness with a higher incidence of complications and a poor prognosis. In a study of 95 patients admitted with falciparum malaria, 20 had evidence of malarial hepatitis. The clinical presentation of these patients was not different from those without hepatitis. However, the incidence of complications such as renal failure (60% vs. 25%), Adult Respiratory Distress syndrome (35% vs. 3%) and septicemia (20% vs. 6%) was significantly higher. The mortality too was higher in patients with malarial hepatitis (40% vs. 17%).[8] In another study from Thailand, 390 patients with acute falciparum malaria were studied. One hundred and twenty-four patients were jaundiced and had more complications in the form of cerebral malaria, acute renal failure, pulmonary edema and shock.[9] Hepatic dysfunction is reversible in all the patients developing malarial hepatopathy who respond favorably to antimalarial therapy and no residual effects have been documented in survivors.[53],[10] Conclusion Deranged liver functions are commonly seen as a complication of severe malarial infection; however, histologically severe hepatic inflammation has never been documented. The term "malarial hepatitis" may be a misnomer and "malarial hepatopathy" may aptly describe our current knowledge of hepatic dysfunction in severe malarial infection.[17] P . falciparum infection is the commonest etiology. Presence of raised hepatic enzymes with near normal coagulation parameters, in presence of documented malarial infection should suggest presence of malarial hepatopathy. Severe hepatic dysfunction in malaria is usually associated with coexisting viral hepatitis or underlying chronic liver disease. Patients with malarial hepatopathy are more prone to complications; hence it should be promptly recognized. Since patients with malarial hepatopathy have a better outcome than those with other causes of hepatic failure, it should be aggressively treated.References
Copyright 2006 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp06108t4.jpg] [jp06108t1.jpg] [jp06108t3.jpg] [jp06108t2.jpg] [jp06108f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}