 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
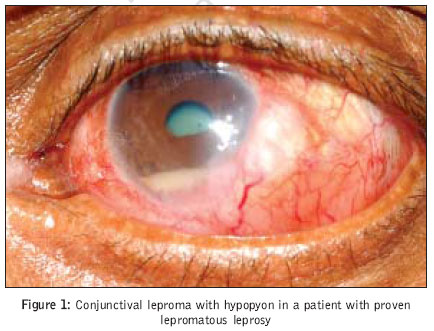
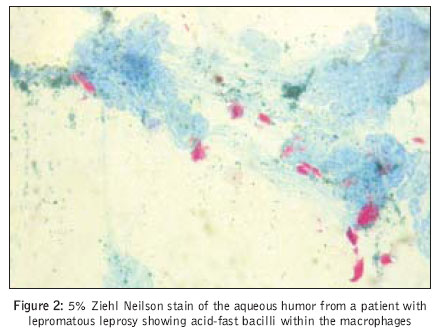
Journal of Postgraduate Medicine, Vol. 53, No. 1, January-March, 2007, pp. 46-47 Images In Medicine Hypopyon in leprosy uveitis Rathinam S, Prajna L Department of Uvea, Aravind Eye Hospital, Madurai Date of Submission: 19-Aug-2006 Code Number: jp07017 A 42-year-old male patient presented with pain and redness in his left eye for two months. The patient presented to an ophthalmologist 15 years after his initial diagnosis of histopathologically confirmed polar lepromatous (LL) leprosy. The treatment history revealed discontinuation of the drugs prescribed for leprosy after one month of initiation because of recurrent episodes of erythema nodosum leprosum (ENL) and he was lost to follow-up from leprosorium. On general examination, the patient had malformation of fingers and toes with multiple tropic ulcers and hypopigmented skin lesions. Ocular examination revealed madarosis in both eyebrows. Right eye was normal with a visual acuity of 20/20 and intraocular pressure was 17 mm of Hg. Left eye had a subconjunctival leproma, peripheral vascularization around the cornea and a leprosy granuloma over the iris. A 2 mm hypopyon and inflammatory cells were present in the anterior chamber [Figure - 1]. His vision was 20/200 in the left eye and the intraocular tension was 17 mm of Hg. Endogenous endophthalmitis, HLA B27-related uveitis, tuberculosis, Behcet's syndrome and leptospirosis were considered in the differential diagnosis of this hypopyon uveitis. A thorough systemic, ocular examination, complete blood count, biochemical, serological and radiological workup ruled out the possibility of the above conditions. X-ray orbits revealed no intraocular foreign bodies. X ray chest was clear. Ultrasonographic examination of the left eye revealed an acoustically clear vitreous cavity. However, to rule out early endogenous endophthalmitis, a diagnostics paracentesis was carried out and the aspirate was subjected to Gram's stain, 10% potassium hydroxide and 5% Ziehl Neilson stain. The anterior chamber aspirate was negative for bacteria and for fungus, however, on Ziehl Neilson staining, plenty of acid-fast bacilli within the macrophages were seen in the aqueous humor [Figure - 2]. As the patient underwent invasive investigatory procedure, steroids were avoided and topical 0.3% ofloxacin eye drops were given. The patient was referred to a dermatologist for leprosy treatment. Discussion Leprosy , is a chronic granulomatous disease of the skin, nerves, eyes and internal organs. Several studies have been done on the ocular manifestations of leprosy.[1],[2],[3],[4] Ocular involvement in leprosy is either due to primary infection of the eye or secondary neural involvement. Lagophthalmos, ectropion, trichiasis, conjunctival leproma, prominent corneal nerves, impaired corneal sensation, exposure keratitis, scleritis and chronic uveitis are commonly noted clinical signs in ocular leprosy.[2] India, has the world's largest leprosy population. In spite of large number of leprosy uveitis cases, hypopyon has never been recognized as a clinical finding in ocular leprosy. However there are two independent reports from countries with low prevalence. We present the microscopy proven case of hypopyon uveitis in a lepromatous leprosy patient. Histopathological analysis of iris tissues obtained during cataract surgery revealed evidence of silent uveitis in 61% of specimens.[3] The present patient had evidence of chronic uveitis in both eyes. Ocular leproma is a granulomatous nodule in the eye, usually near the limbus or deep in the iris and ciliary body. Lepromas are usually yellowish and fleshy and may resemble a conjunctival tumor. Unlike scleritis, a leproma is completely painless.[2] Ocular lepromas occur in MB patients treated irregularly by dapsone monotherapy and are usually a sign of dapsone resistance. Treatment negligence could be the cause for leproma in our patient. Hypopyon, an inflammatory cell collection in the anterior chamber, is seen commonly is HLA B27-related uveitis, Behcet's syndrome, leptospirosis, retained foreign body, tuberculosis, lens protein uveitis, and traumatic endophthalmitis. In western literature HLA B27-related uveitis is reported as the most common type that presents with hypopyon in contrast to the tropical uveitic subtypes that are due to leptospirosis and tuberculosis. However, Robertson and Voisin independently reported presence of hypopyon and Mycobacterium leprae from the anterior chamber from leprosy patients.[5],[6] In spite of the high prevalence of leprosy uveitis in India, hypopyon has neither been identified nor microbiologically proved in leprosy. Cell-mediated immunity is greatly impaired in lepromatous patients. Without the assistance of T cells, the macrophages cannot digest M. leprae but only ingest them. Erythema nodosum leprosum is an exaggerated immunological reaction in lepromatous leprosy and it is not protective in nature. Hence in spite of recurrent ENL reaction the patient had, the anterior chamber aspirate showed a high bacillary load. This report depicts a case of confirmed polar LL leprosy with a rare ocular clinical sign, hypopyon. References
Copyright 2007 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp07017f2.jpg] [jp07017f1.jpg] |
| |||||||||

{kind=link}
{kind=link}