 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
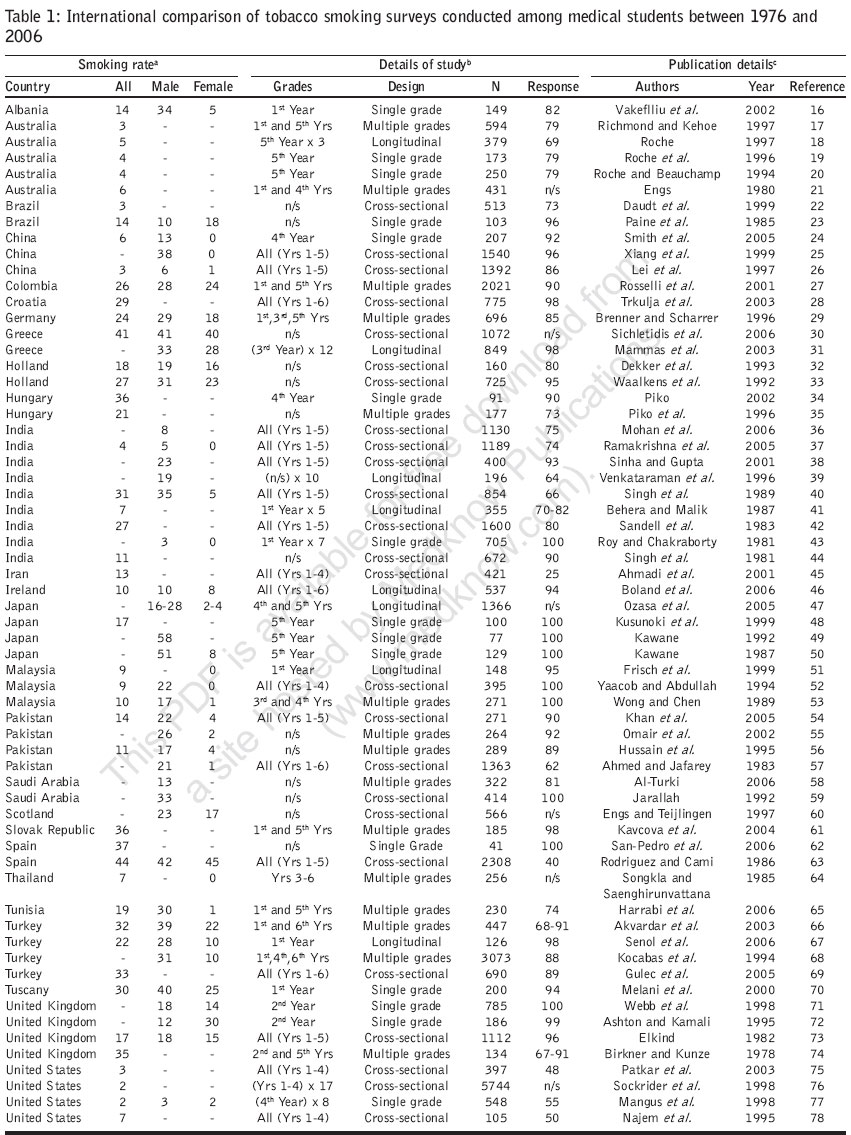
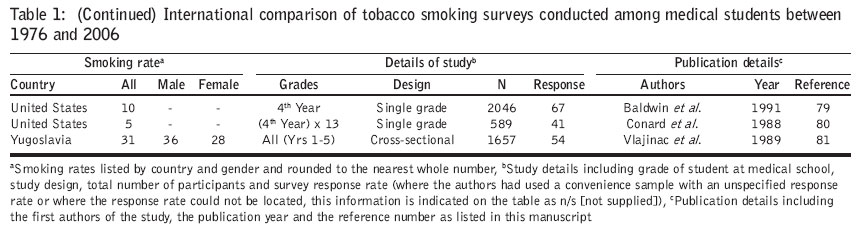
Journal of Postgraduate Medicine, Vol. 53, No. 1, January-March, 2007, pp. 55-62 Review Article An international review of tobacco smoking among medical students Smith DR, Leggat PA Japan National Institute of Occupational Safety and Health, Kawasaki, Japan; Anton Breinl Centre for Public Health and Tropical Medicine, James Cook University, Townsville, Australia Date of Submission: 12-Sep-2006 Code Number: jp07021 Abstract We conducted a systematic international review of tobacco smoking habits among medical students. Particular attention was paid to countries where smoking rates have been historically well-documented in local journals, but were less often included in larger international review articles. The methodology involved a search of relevant medical subject headings, after which the reference lists of journal papers were also examined to find additional publications. A total of 66 manuscripts met the inclusion criteria. The most common countries previously studied included India, the United States, Australia, Japan, Pakistan, Turkey and the United Kingdom. Overall, our review suggests that the prevalence of smoking among medical students varies widely amongst different countries and also between male and female students within the same areas. Consistently low smoking rates were found in Australia and the United States, while generally high rates were reported in Spain and Turkey. Given their important future role as exemplars, more effective measures to help reduce tobacco smoking among medical students are clearly needed worldwide.Keywords: Medical education, medical student, prevalence, smoking, tobacco Health professionals have an important role to play in the fight against tobacco. As individuals they can help educate the population, as community members they can support anti-smoking policies and at a societal level, they can influence national and global tobacco control efforts.[1] Physicians occupy a key position in this regard, as they are uniquely placed to lead smoking cessation programs in the community.[2] Patients expect information, help and guidance from their primary care physician on a number of health-related matters.[3] Physicians also play an important role in helping patients to stop smoking.[4] As future physicians who will witness the continued burden of smoking-related diseases among their patients, medical students represent a primary target for tobacco-prevention programs. The potential success of these strategies may be suboptimal however, if the true dangers of smoking are not adequately recognized. As medical students progress through medical school for example, their knowledge of smoking-related diseases naturally increases.[5] Nevertheless, substance use remains fairly common in this group[6] and a superior knowledge of smoking-related risks does not always correlate with a lower rate of smoking among senior medical students.[5] As such, many researchers have historically investigated tobacco smoking rates among this demographic group. The first step in understanding the problem was to find out what proportion actually smoked. In this regard, in 1966, Mausner[7] noted that around one-third of their American medical students were using tobacco products. Research from Australia in the early 1970s also suggested a similar prevalence rate.[8] In 1985, the tobacco and health committee of the international union against tuberculosis and lung disease began a large investigation on smoking habits among medical students in a variety of countries. The first publications focused on medical students in 14 European countries,[9] followed by research among 10 African and Middle Eastern countries[10] and nine Asian countries.[11] In 1993, Tessier et al .[12] published another large study of smoking behavior among medical students in Australia, Japan, the United States, Russia and Estonia. Smoking rates among students were shown to vary widely from country to country.[13] In 2005, the World Health Organization (WHO), the US Centers for Disease Control and prevention and the Canadian Public Health Association developed what was termed the Global Health Professionals Survey to investigate tobacco smoking habits among medical, dental, nursing and pharmacy students in a variety of WHO member states. Results from their pilot study were published in 2005.[14] While a large number of researchers have now investigated the issue of tobacco smoking among medical students, few systematic international reviews appear to have been conducted on this topic. The purpose of the current paper therefore, was to undertake a systematic international review on the prevalence of tobacco usage among medical students. We also paid particular attention to countries where smoking rates among medical students have been well-documented in local studies and domestic journals, but where the results were less often included in larger international reviews on the topic. A further aim of this review was to investigate the epidemiological quality of smoking research articles which have targeted medical students. Methods Our current study began with an extensive literature review targeting manuscripts published in peer-reviewed journals relating to the topic of tobacco smoking among medical students. The review began with a search of relevant medical subject headings such as 'smoking', 'tobacco' and 'medical student' on PubMed, the National Library of Medicine in the United States.[15] After identifying some initial journal papers, the search was repeated using keyword variations such as 'smoke', 'medical education' and 'substance use'. To be sure that we did not miss any manuscripts from the underrepresented countries previously mentioned, further country-specific keywords such as 'India', 'Pakistan', 'Malaysia', 'Thailand' and so on, were also added to the search. Due to the wide variety of languages used for publishing scientific articles on PubMed, our review was limited to manuscripts written in English. As research becomes dated quickly, only articles published in the past 30 years (that is, between 1976 and 2006 were included in the current review. The reference lists of all journal papers located using these initial criteria were subsequently examined to find additional publications. Manuscripts were sorted by country of origin and then arranged in descending order on a single table, according to the year in which the study was published. All papers were assigned an ascending reference number based on the abovementioned criteria. For consistency, all smoking prevalence rates were rounded to the nearest whole number and listed as prevalence rates by gender and as total group prevalence rates, wherever possible. The study design for each manuscript was assigned into the following four epidemiological categories: Single grade (where only one grade of students was sampled), multiple grade (where multiple grades of students were sampled), cross-sectional (where a complete cross-section of students from the medical school had been sampled) and longitudinal (where at least one grade of students was sampled at more than one point in time). Where a single grade of medical students was sampled in multiple locations, the number of grades actually sampled was listed after the grade. Year of study in the medical course which the sampled students were attending, was also listed. Response rates for each study were examined and then rounded to the nearest whole number for standardization purposes. Where authors had used a convenience sample with an unspecified response rate or where the response rate could not be determined from the manuscript, a note on this missing information was also indicated on the table. Discussion A total of 66 manuscripts met the inclusion criteria for this review [16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32],[33],[34],[35],[36],[37],[38],[39],[40],[41],[42],[43],[44],[45],[46],[47],[48],[49],[50],[51],[52],[53],[54],[55],[56],[57],[58],[59],[60],[61],[62],[63],[64],[65],[66],[67],[68],[69],[70],[71],[72],[73],[74],[75],[76],[77],[78],[79],[80],[81] as indicated in [Table - 1a, b]. The most common countries in which they had been conducted included India, the United States, Australia, Japan, Pakistan, Turkey and the United Kingdom. The majority had been undertaken as questionnaire surveys among a complete cross-section of students within a single medical school. The next most common methodology involved surveying a single grade of medical students, usually comprising those in either the first grade or fifth grade at university. The number of participants in each study ranged from 41[62] to 5744[76] with a median of 407 students. Particularly large surveys of medical students' tobacco smoking habits (where over 2000 participants were sampled) appear to have been conducted in the United States,[76] Turkey,[68] Spain[63] and Colombia.[27] Overall survey response rates ranged from 40%[63] to 100%[43],[48],[49],[50],[52],[53],[59],[62],[71] with a median response rate of 90%. Few manuscripts had response rates below 50%[63],[75],[80] while the participation rate in seven other studies was not specified. While these demographic findings were encouraging, some confounding factors were also evident among some articles located during our review. One particularly important confounder was a lack of standardization regarding the definition of 'smoker'. Although most researchers classified their subjects dichotomously, as being either smokers or nonsmokers, some other recall periods were occasionally used, such as daily smoker, occasional smoker and so on. This shortfall is not only limited to tobacco smoking surveys of medical students however, having been previously noted as a methodological issue in other review articles conducted among different populations.[82] The problem possibly arises when studying medical students due to the inherent difficulties in determining tobacco usage habits over time and the fact that most investigations investigate the point-prevalence of smoking among the surveyed group. Medical students, as indeed all university students, represent a widely dispersed population who are often away from campus while undertaking practical training. This methodological limitation suggests that surveys conducted among single grades of students during lecture periods, have probably been the most practical manner for investigating smoking. Whatever the cause of these methodological shortfalls, the issue of what exactly comprises a 'currently smoking' medical student clearly represents an area on which some international agreement should be reached, in order to allow greater comparability between future investigations. Furthermore, from an epidemiological perspective, some fundamental issues should also be considered. For smoking surveys to report any meaningful data on the population as a whole, it is important that a large proportion of the total group is captured and that a large proportion of those who are contacted, actually respond. In our current review, despite the existence of the aforementioned confounding factors, we were encouraged to find that a large proportion of all manuscripts had reasonably large sample sizes (in the hundreds) and sufficiently high response rates to allow confidence in the published data. In this regard, 75% of the studies we reviewed had obtained survey response rates between 74% and 97%. Aside from response rates, results from surveys conducted among a cross-section of students at a single medical school also permit some analysis of the changing nature of smoking as students progress through their course of study. The prevalence of smoking among medical students appears to vary widely from country to country. From the current review it appears that smoking rates among male medical students range between 3% in the United States[77] and 58% in Japan.[49] The lowest overall prevalence rates of 2-3% were documented in American medical schools during the late 1990s,[75],[76],[77] with similar low levels also reported in Australia (3%),[17] China (3%)[26] and India (4%).[37] Smoking prevalence rates below 10% of the medical student population were shown to occur in Australia (4-6%),[18],[19],[20],[21] China (6%),[24] India (7%),[41] Thailand (7%),[64] the US (7%)[78] and Malaysia (9%).[51],[52] Marked differences in smoking rates were found by gender in almost all studies, with male students generally having the higher rates. Other relatively high prevalence rates among male medical students were also reported in Greece (41%)[30] and Spain (42%).[63] When considering the prevalence of smoking among medical students in a particular country, it is worthwhile considering to what extent their habits mirror those of the society in which they live. In the current review, as mentioned earlier, medical students in the United States, Australia, China and India were the least likely to smoke. This finding is consistent with population data from the WHO,[1] where it is reported that only 18-21% of Australian adults and 21-26% of American adults consume tobacco. On the other hand, the seemingly low rate of smoking among Chinese medical students is contrary to recent population data from the WHO, details of which are published elsewhere.[1] The high proportion of tobacco users that we identified among medical students in Japan, Greece and Spain, appears to reflect current population estimates for these countries, where it is reported that 39-47% of adult males and 12-29% of adult females still smoke tobacco. While the smoking prevalence rate among female medical students was generally lower than their male counterparts at the same medical school across a range of studies, at least seven investigations reported not having any female smokers at all. This particular phenomenon was evident in China,[24],[25] India,[37],[43] Malaysia[51],[52] and Thailand.[64] It has been previously suggested that smoking may be regarded as inappropriate behavior for women in certain countries,[5],[83] a cultural consideration which may have led to the situation observed among female medical students in the current review. Nevertheless, it is also possible that some females who did actually smoke in certain countries may not have admitted their smoking habit during the survey, for these cultural reasons. Aside from countries where the smoking prevalence among female medical students was reported to be either zero or was not recorded at all, very low smoking prevalence rates of only 1% were also documented among female students in China,[26] Malaysia,[53] Pakistan[57] and Tunisia.[65] Again, these low results seem to suggest a cultural reluctance for women to smoke in certain countries. Such hypotheses are supported by marked gender differences in population smoking rates in India, where 30% of males but only 3% of females smoke and in China, where the WHO estimates that smoking ranges from 4% in adult Chinese females to 53% among adult Chinese males.[1] Aside from gender issues, the results of cross-sectional tobacco smoking studies are also interesting to consider, as they help elucidate changes in smoking behavior as a student progresses through medical school. As previously mentioned, our current review located numerous studies which had been conducted among a cross-section of students at the same medical school. Almost all of them found that tobacco smoking rates among medical students tend to increase between the year of entry and the final year. In India for example, Ramakrishna et al .[37] reported that the tobacco smoking prevalence ranged from 7% among the male first-year students to 16% among the fifth-year students. Also in India, Singh et al .[40] found that smoking rates increased from 17% to 43% between the first and fifth years, while Sandell et al .[42] observed a similar trend, albeit with lower overall prevalence rates (ranging from 4% in the first year to 10% in the fourth and fifth years). An earlier Indian study from the late 1970s conducted by Singh et al .[44] suggested that smoking prevalence rates in the 1970s also followed a similar trend (ranging from 27% in the first year to 49% by the intern period). Research conducted in Manchester by Elkind[73] documented the prevalence rate rising from 16% in the first year to 20% in the fifth year. Similarly, in Yugoslavia, Vlajinac et al .[81] demonstrated that smoking rates increased from 27% to 36% during the five years of medical school. Not all studies of tobacco usage among medical students demonstrated a linear trend of increasing prevalence, however. In the United States for example, Patkar et al[75] found that tobacco smoking rates fluctuated from 3.3% in the first year, to 2.5% in the second year and then back up to 3.8% in the third and fourth years. In Iran, Ahmadi et al .[45] also revealed that tobacco usage ranged from 18% in the first-year group, to 7% in the third-year group and then back up to 17% in the fourth-year group. Considering the results of previous investigations and the fact that response rates were not mentioned, the possibility of demographic differences in the third year group of Ahmadi et al 's[45] study, should be considered. Our current review located several longitudinal studies of tobacco smoking which had been conducted on medical students in Australia,[18] India,[39],[41] Ireland,[46] Japan,[47] Malaysia[51] and Turkey.[67] In the first study, Roche[18] targeted three separate groups of male and female students in their fifth year of study at an Australian medical school. Surveys were conducted in 1986, 1990 and 1993, with response rates of 65%, 73% and 68%, respectively. The prevalence of smoking among them steadily declined over the eight-year period, beginning at 10% in 1986, falling to 4% in 1990 and then to 3% in 1993.[18] In another study, Venkataraman et al[39] investigated 10 successive groups of male students enrolled at an Indian medical school between 1955 and 1988. Similar to Roche,[18] the Indian authors also found that the overall prevalence of smoking was on the decline, falling from 42% (in the period 1955-60) to 25% (in the period 1985-1988).[39] Boland et al[46] followed three separate groups of male and female students at an Irish medical school between 1973 and 2002. The 1973 investigation targeted students in their first, third, fourth and sixth year of study, while in 1990 and 2002 all six years of the medical school were surveyed. The overall prevalence of smoking declined from 29% in 1973, to 15% in 1990 and then 10% in 2002.[46] In Malaysia, Frisch et al .[51] recruited a cohort of male and female medical students in their first year of study during 1991-92, following them up two years later in the 1993-94 school year. Unlike the three previous investigations, the prevalence of smoking among this Malaysian cohort actually increased from 9% to 11% during the follow-up period. Interestingly, all smokers were male, with no female smokers in either group.[51] Again, this finding suggests a possible cultural reluctance for women to smoke in certain countries, as previously described.[83] The most recent longitudinal study of tobacco smoking among medical students appears to have been conducted in Turkey by Senol and colleagues.[67] In their investigation, 22% of students (male and female) were smoking in the first year of study, a rate which had risen to 27% by the sixth year. Roughly one-third (32.3%) of Senol et al's[67] original nonsmokers in the first year had also become smokers by the end of the sixth year at medical school. While it would no-doubt have been useful to compare the smoking habits of undergraduate medical students with postgraduate medical students, few if any researchers appear to have done so. A Japanese investigation of this nature was conducted by Imai et al in 2003,[84] but it was published in Japanese and therefore had to be excluded from the current review. Even so, in order to meet the current information shortfall, future international researchers who look at tobacco smoking among medical students would probably benefit by expanding their study to include a more comprehensive survey of the demographic wherever possible. Conclusions Overall, our review suggests that the prevalence of smoking among medical students varies widely between students of different countries and also between male and female students within the same countries. Consistently low prevalence rates were documented in regions such as Australia and the United States, while generally high rates were seen in countries such as Spain and Turkey. While many cross-sectional investigations suggested that the prevalence of smoking seems to increase during the more senior grades, it is difficult to assess whether this trend directly reflects university seniority, increasing age or both. Some other conflicting results were also found. Various researchers for example, have suggested that the smoking habits of parents may be very important in influencing whether a medical student smokes.[81],[85] On the other hand, other researchers found no association between whether students smoked at medical school and whether their parents were smokers.[86] As such, it is worthwhile considering a few key issues, such as what factors contribute to smoking in particular countries and also why medical students choose to smoke tobacco at all. In this regard, social, cultural and other country-specific factors no-doubt strongly influence whether a medical student in that particular region smokes tobacco. As previously described, most studies that reported low rates of smoking among medical students had concurrently low rates of tobacco usage in their general population. Where major gender differences existed in smoking rates among medical students, a similar phenomenon was, for the most part, also present within the general community in which they lived. The importance of population-based influences on a medical student's decision to smoke, therefore, is clear. Cognitive dissonance may also play a role for student smokers. In one of the earliest studies of smoking among medical students, Mausner[7] reported that significantly more nonsmokers than smokers accepted that evidence linking tobacco usage and disease was 'strongly convincing'. In this regard, medical students in some countries may still believe that smoking is not particularly hazardous or at least, not hazardous enough to warrant quitting. In a comprehensive survey of smoking among European medical students for example,[9] it was noted that there was limited overall knowledge regarding public health measures for tobacco control. Future population-based reduction strategies will, therefore, need to consider not only smoking among youth, but also smoking among specific young adult populations such as university students. Their motivations for taking up smoking and not quitting may or may not reflect those of the general adult communities in which they live. Whatever the underlying demographic correlates of tobacco usage in this distinct sub-population, it is clear from the current review that too many medical students continue to use tobacco. Given their important future role as exemplars, there are a few measures which will need to be considered in meeting this important public health dilemma. Education represents probably the most critical issue in smoking cessation for both medical students and the general public alike. It has previously been noted that educating both physicians and medical students about the importance of smoking as a cause of disease represents the first step for getting them involved in smoking cessation.[87] While medical schools should clearly provide educational programs in this regard,[88] it has been suggested that not enough medical schools actually teach specific courses on tobacco control.[89] Not doing so may allow an entrenched smoking culture to remain among the student demographic and thus jeopardize their future role as physicians responsible for tobacco control programs. In Japan, for example, a country with some of the highest historical and contemporary smoking rates among adults, Kawakami[90] demonstrated that the intention of medical students to perform future smoking interventions was still unsatisfactory in the late 1990s, with only one-third even being actively interested in the topic. While medical schools should clearly be encouraged to address this important issue, not all of them appear to be doing so. A previous worldwide survey on the topic, for example, suggested that some medical schools still need continued encouragement for undertaking adequate tobacco control education.[91] Postgraduate training in tobacco control represents a key step forward in this regard, as it has previously been suggested that this represents a time when basic medical education is actually completed.[92] General strategies for promoting tobacco control among young people have also been proposed by the WHO's Tobacco-Free Initiative[1] and its particular publications on tobacco smoking among the world's younger population.[93] Many of these strategies are applicable for use among medical students. Firstly, it has been noted that a comprehensive mix of anti-smoking legislation, pricing and community-based strategies can be effective in reducing tobacco consumption among youth. As most university students including those at medical school, would have limited financial means, it is reasonable to assume that any legislation increasing the price of tobacco would subsequently result in a drop in the overall number of student smokers. Secondly, there needs to be a stronger focus on positive youth development during the transition from youth into adulthood.[93] This issue could be incorporated into medical education to help students as they progress through their course and mature from undergraduate students into young doctors. As smoking rates appear to increase by year of study, this type of transition-focused approach is urgently needed in medical schools worldwide. Considering these facts, the role of medical schools in tobacco control programs to help their own students stop smoking , simply cannot be overlooked. Regardless of when medical educators actually begin teaching their students about tobacco control, it seems clear from the current review that tobacco-specific education should become mandatory in future years. References
Copyright 2007 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp07021t1b.jpg] [jp07021t1a.jpg] |
| |||||||||

{kind=link}
{kind=link}