 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 53, No. 1, January-March, 2007, pp. 63-71 Review Article Psoriatic arthritis as a distinct disease entity Leung YY, Tam LS, Kun EW, Li EK Department of Medicine and Geriatrics. Taipo Hospital Date of Submission: 13-Jun-2006 Code Number: jp07022 Abstract Psoriatic arthritis (PsA) is a chronic systemic inflammatory disease characterized by joint inflammation associated with cutaneous psoriasis. For many years, the amount of attention directed to PsA had been less than that for various other arthropathies. With the advances in understanding its pathogensis, it is now recognized as a distinct disease entity with characteristic features. Psoriatic arthritis has a greater tendency towards asymmetric oligoarticular involvement, distal interphalangeal involvement and spondylitis. Associated features such as enthesitis and dactylitis are more common. Specific radiological features include ankylosis and bone resorption. With the availability of potent new therapeutic agents for psoriasis and PsA, interest in research and clinical care for these conditions has been reinvigorated. Anti-TNF therapy has achieved encouraging efficacy in both the joints and skin disease, improving function and quality of life and inhibiting radiological progression measured in patients with PsA and psoriasis. Biologic agents may have the potential in addressing the unmet medical need in patients with PsA.Keywords: Clinical features, psoriatic arthritis, targeted therapies Psoriatic arthritis (PsA) is a chronic systemic inflammatory disease characterized by joint inflammation associated with cutaneous psoriasis. PsA may be progressive, destructive and deforming. Its exact prevalence is unknown, but estimates vary from 0.3% to 1% of the population.[1] Both the skin lesion and the joint involvement may have deleterious effects on affected individuals. For many years the attention on PsA has been less than that on other arthropathies. The management and assessment of PsA was to "borrow" from that of rheumatoid arthritis (RA). However, this extrapolation may be inappropriate. PsA is now recognized as a distinct entity. Unique clinical features include distal phalangeal joint (DIPJ) involvement, dactylitis, enthesitis, osteolysis and periarticular new bone formation on radiographs and specific skin and nail changes. Classification Despite clinical, radiological and familial evidence supporting PsA as a distinct disease entity, controversy still exists about how to classify patients having this disease. The Moll and Wright criteria are the simplest and the most frequently used diagnosis of PsA.[2] The criteria are:
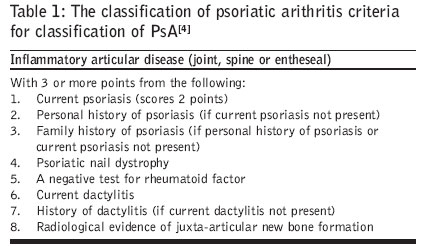
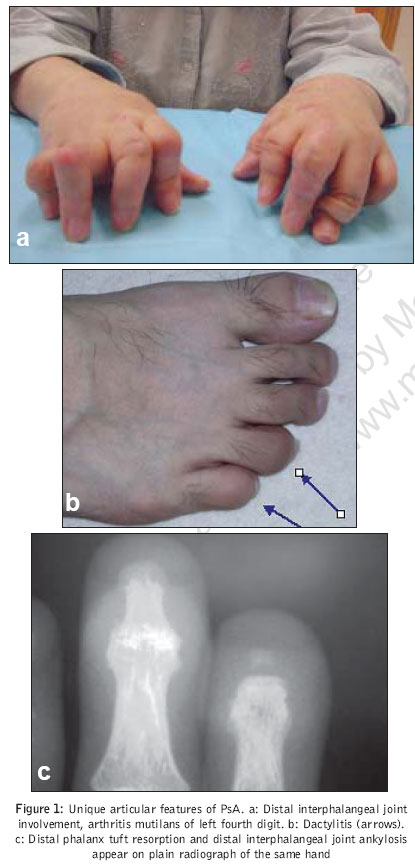
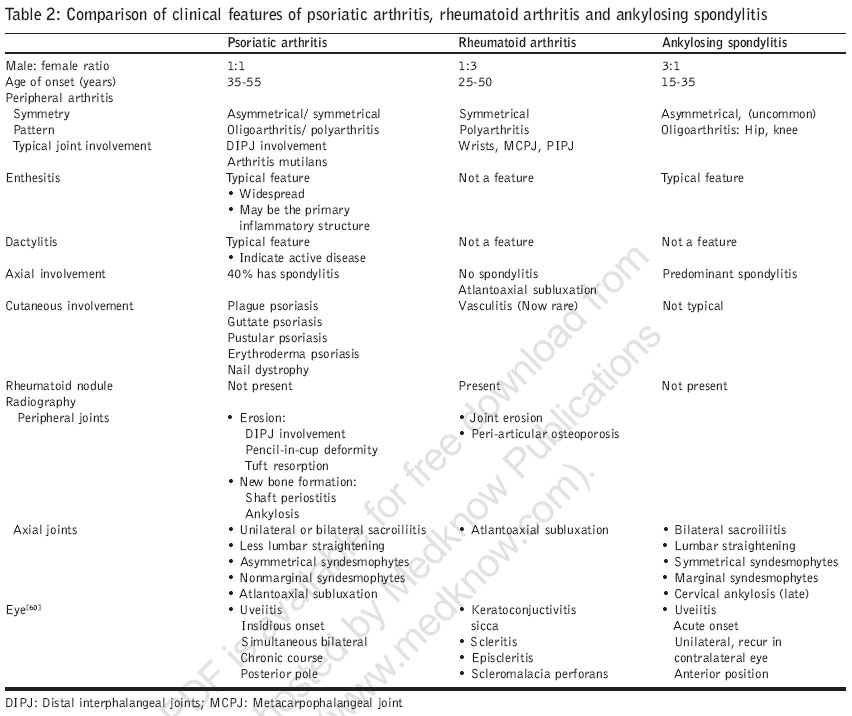
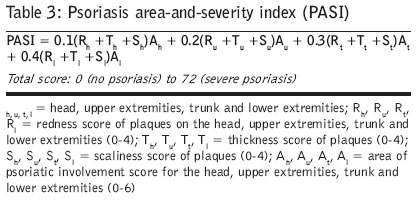
Under these diagnostic criteria, five subgroups of PsA were described: distal interphalangeal joint only, asymmetrical oligoarthritis, polyarthritis, spondylitis and arthritis mutilans. Minor modifications have been made to the Moll and Wright subgroups by a number of authors including Gladman et al , [3] Helliwell et al ,[4] Marshal et al[5] and Torre-Alonso et al[6] None of these criteria were validated using patient data and have not been used in prospective studies. It is of interest to note that in these subsequent reports, higher proportions of patients having symmetrical polyarthritis were included than the original Moll and Wright series. A definition of symmetry was never clarified. It was subsequently demonstrated that symmetry is a function of the number of joints involved rather than a distinctive feature of PsA.[4] Patients with early PsA may have fewer clinically involved joints that accounts for the asymmetry of the disease. As the disease progresses, more joints could be involved resulting in a symmetrical pattern. Some authors suggested classifying PsA into two broad subsets: peripheral and axial disease.[4],[5] The only validated criteria for classifying psoriatic arthritis derived from patient data were developed by Fournie et al[7] The data were derived from a population of patients from a single center and have yet to be tested in other populations. The major drawback was the inclusion of HLA data as a criterion and difficulty to use it in clinical settings. The classification of PsA criteria were recently developed as an agreed and validated classification for PsA. The criteria were derived by a prospective, multi-centered observational study of 588 consecutive clinic patients with PsA and 536 controls with other inflammatory arthritis.[8] It gives a sensitivity and specificity of 0.914 and 0.987 to classify PsA from nonPsA. The criteria classify PsA when there is an inflammatory articular disease of joint, spine or enthesis plus three points of the following: current, personal or family history of psoriasis, psoriatic nail dystrophy, a negative test for rheumatoid factor, current or history of dactylitis, radiological evidence of juxta-articular new bone formation [Table - 1]. Clinical Manifestations Although some patients with PsA may have peripheral arthritis resembling RA, PsA has greater tendency towards asymmetry and oligoarticular involvement. The DIPJs are more frequently involved. Severe DIPJ involvement and digital tuft resorption could give rise to telescoping of finger or arthritis mutilans [Figure - 1]a. Enthesitis and dactylitis are more common than RA. While RA is more common among women, PsA occurs equally in both sexes. Rheumatoid factor, which is detected in 80% of patients with RA, may only present in up to 13% of patients with PsA. Rheumatoid nodules are typically absent in PsA[1] [Table - 2]. PsA is also classified under the spondyloarthropathies. Up to 40% of PsA patients have spondylitis. PsA may be distinguished from the other spondyloarthropathies by the presence of more widespread and more severe peripheral arthritis, asymmetrical distribution of sacroiliitis and syndesmophytes in the axial spine. The occurrence of extra-articular features is common to the spondyloarthropathies, including mucous membrane lesions, iritis, urethritis, diarrhea, aortic root dilatation and the association with HLA-B27. The presence of skin psoriasis The presence of skin psoriasis is the most distinguishing feature of PsA when contrasted with other arthropathies. Psoriasis comes from the Greek word 'psora', which means itch. It is characterized by well-demarcated erythematous plaques distributed over extensor body surfaces and the scalp. The plaques usually exhibit salmon redness and silvery scaling as a result of epidermal hyperproliferation and dermal inflammation. There are two main types of psoriasis: psoriasis vulgaris (plaque psoriasis) and psoriasis pustulosa (pustular psoriasis). The different types of psoriasis can be divided into subgroups according to severity, duration, location on the body and appearance of the lesions. Acute flares or relapses of plaque psoriasis may also evolve into more severe disease, such as pustular or erythrodermic psoriasis [Figure - 2]d.[9] Skin psoriasis precedes joint disease in 70% of patients of PsA and occurs concomitantly in 15%. However, arthritis may precede psoriasis in 10-30% of patients. Psoriasis may also present in "hidden" areas like natal cleft, around the umbilicus or the hairline [Figure - 2]a-b. Psoriasis may only be evident in the nails. Nail lesions are common and distinguish patients with PsA from those with RA. The characteristic lesions are pitting, subungual hyperkeratosis, discoloration, dystrophy and onycholysis [Figure - 2]c. The association of DIPJ with nail disease is well recognized.[10] Psoriatic arthritis is associated with higher rate of nail disease than psoriasis alone. In one study, nail involvement was found in 40-45% of patients with psoriasis and in up to 87% of patients with PsA.[11] In the true absence of psoriasis, a positive family history in the first degree relative might be of equal importance. The course of psoriasis is influenced by various environmental factors. Many patients experience worsening of symptoms in winter. The classical Koebner's phenomenon describes the exacerbation of psoriatic lesions at the site of physical injury and is possibly mediated through the unmasking of autoantigens and release of proinflammatory cytokines.[12] Infections, particularly streptococcal infections of the upper respiratory tract and human immunodeficiency virus infection, have long been recognized as triggers of psoriasis.[13],[14] Dactylitis Dactylitis, one of the hallmark clinical features, occurs in around one-third of patients with PsA. It appears as swelling or sausaging of the entire digit, predominantly due to swelling and inflammation in the flexor tendon sheaths [Figure - 1]b. Predominant flexor tenosynovitis was demonstrated by a magnetic resonance imaging (MRI) and ultrasonography study.[15] Although most clinicians consider dactylitis an important manifestation, there is no validated measure of assessment. Using grading system for severity (Grade 0-3) multiplied by the number of digits involved has been employed in PsA clinical trials.[16],[17],[18] Enthesitits and the enthesis organ Enthesitis is the inflammation at the site of attachment of a tendon or a ligament to the joint capsule. With the emerging knowledge from animal anatomical studies and MRI studies, the entheseal structure and function appears to be more complex than initially proposed. The concept of an 'enthesis organ' emerged.[19] In this concept, the enthesis together with the adjacent fibrocartilage, periosteum, synovial and bursa membranes should be viewed as a unique 'organ'. PsA was proposed to be a primarily enthesis disease as compared to primarily synovial disease in RA. Clinical features that are suggestive of this enthesitis pathology included peripheral enthesitis, DIPJ involvement, spinal inflammation, oligoarthritis, dactylitis and specific periostitis and osteolysis.[20] For example, the radiographic descriptions of the "pencil-in-cup" deformity of the DIPJ can be explained by enthesitis. The DIPJ has only a trace amount of synovium to be explained in terms of a synovial-based pathology. The distal tuft exhibits capsule calcification and central erosion at the site of tendon insertion. The fluffy periostitis and bone erosions adjacent to the capsule are also suggestive of enthesitis. In a cadaveric study, many articular as well as extra-articular enthesis organs were identified throughout the body. These findings may help to explain the widespread pain observed in many PsA patients that may be related to clinically unrecognized enthesitis.[21] Two methods of assessment of enthesitis were developed and validated in patients with ankylosing spondylitis (AS). These are the Mander enthesis index (MEI) and the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES).[22],[23] The MEI assesses 66 sites, which is far too many to be feasible in daily practice and clinical trials. The MASES is a culling of 13 specific points from the MEI. It has been validated in patients with AS. These scores however, have not been validated in PsA or utilized in PsA clinical trials. Simpler measures of the presence or absence of enthesitis at the Achilles tendon have been employed in clinical trials and improvement with treatment has been shown.[16],[17],[18] SAPHO syndrome The SAPHO syndrome (Synovitis, Acne, Pustulosis, Hyperostosis and Osteitis) was reported in 2% of patients with PsA.[24] This occurrence of musculoskeletal manifestations (including synovitis, chest wall arthro-osteitis and multifocal aseptic osteomyelitis) in association with severe acne, palmoplantar pustulosis and of psoriasis was also related to inflammatory bowel disease and other spondyloarthropathies. The psoriatic variety is HLA-B27 negative and with anterior chest wall symptoms including asymmetric and nonerosive swelling and pain on the sternoclavicular joint, sternal angle area, sternocostal joint and costochondral junction pain.[25] Nonsteroidal anti-inflammatory drugs (NSAIDS) and sulfasalazine used to be the cornerstone of therapy. Pamidronate was reported to be an effective therapy for patients with the SAPHO syndrome.[26] Specific radiological changes In addition to clinical observations and findings, radiographs have also been used to distinguish PsA from RA. In general, the radiographic features can be grouped into erosive and proliferative changes. Erosions typically start at the margins then progressing towards the center. Erosive damage may be very extensive leading to the characteristic pencil-in-cup deformity with a blunted osseous surface on the proximal bone of a joint, protruding into an expanded surface of the distal bone. Marked osteolysis may occur such that the whole phalanx may be resorbed. The DIPJs are often the first to be affected. Proliferative new bone formation can occur along the shaft of the metacarpal and metatarsal bones causing shaft periostitis. Osteoperiostitis of the distal phalanx of the great toe is more frequent in PsA and is associated with nail dystrophy.[27] While some joints demonstrate osteolysis, others demonstrate total ankylosis. The osteolysis and ankylosis may occur in the same hand and even in the same finger [Figure - 1]c. Joint involvement in PsA is often asymmetrical, while periarticular osteopenia is less commonly observed than in RA.[28] Spondylitis is also a characteristic feature of PsA. Features may be similar to that of AS. However, unilateral sacroiliitis, asymmetry of syndesmophytes and development of nonmarginal syndesmophytes may distinguish PsA from AS. Nonmarginal syndesmophytes describes vertebral ossification from vertebral body-to-body as compared to those from corner-to-corner in AS. Psoriatic spondylitis can be less symptomatic and even asymptomatic [Table - 2]. Nonetheless, radiological joint damage at baseline was also found to be a predictor of increased mortality.[29] Genetic Basis for PsA and Psoriasis Psoriasis and PsA are complex genetic disorders resulting from an interplay between genetic and environmental factors. The genetic basis is supported by family-based studies, epidemiology studies, genome-wide linkage scans, association studies with human leucocyte antigens (HLAs) and candidate gene studies within and outside the major histocompatibility complex (MHC) region. Monozygotic twins have a threefold increased risk for psoriasis compared with fraternal twins.[30] Familial clustering of PsA was demonstrated in a populational study by Moll and Wright.[31] The overall prevalence of PsA among first-degree relatives was 5.5% and there was a 19-fold increase in the prevalence of psoriasis among first-degree relatives of patients with PsA compared with the general population. Genetic associations in PsA and psoriasis have been noted in the genes of the MHC region. Individual alleles may be associated with certain features of PsA, such as HLA-B27 with axial involvement and HLA-B38 and HLA-B39 with peripheral polyarthritis. As for psoriasis, the locus termed psoriasis susceptibility 1 (PSORS1) located in the MHC region on chromosome 6 has been replicated in several populations and is considered the most important susceptibility locus.[9] Based on association studies, two types of psoriasis were identified. Type I, young onset psoriasis before age 40 years, is associated with stronger HLA associations (in particular HLA-Cw6), greater family aggregation and more severe psoriasis. Whereas the Type II psoriasis was characterized by later age of onset, lower familial tendency and not related to HLA-Cw6 containing haplotypes.[32] Two genome-wide scans have identified additional regions that may predispose to PsA susceptibility. One is located on chromosome 16q and overlaps with the location of a psoriasis locus.[33] The other is located on Chromosome 15q.[34] Recent studies in Newfoundland suggest that variants within CARD15 on chromosome 16q predispose to PsA[35] but not in psoriasis.[36] CARD15 was proposed to activate nuclear factor kB (NFkB) in response to bacterial lipopolyssacharides. Functional cytokine gene polymorphisms may influence disease susceptibility and phenotype in patients with PsA. Tumor necrosis factor (TNF)-alpha gene promoter polymorphisms were found to be associated with PsA in a meta-analysis.[37] The TNF-alpha-308 and TNF-beta +252 polymorphisms were associated with the presence and progression of joint erosions in PsA, suggesting that TNF gene polymorphism may be a prognostic marker in PsA.[38] Pathogenesis Recent research has illuminated the pathological changes of PsA in skin, joints and enthesis at the molecular, cellular and tissue levels. These organs share similar pathogenic mechanisms that are different from those in RA. By defining the pathogenic cells, cytokines and inflammatory pathways, a rationale is being established for the targeted immunotherapy. An infiltrate comprising activated T cells is localized in the dermal papillae of the skin, the sublining layer of the joint synovium and the enthesial insertion. Other key cells include dendritic cells, macrophages and B cells. These cells generate proinflammatory cytokines, such as TNF-alpha, interleukin (IL)-1 and IL-6, which in turn contribute to the activation of additional pathogenic cells.[39] TNF-alpha plays a key role in driving the inflammatory process that mediates angiogenesis and bone resorption. Targeting TNF-alpha has achieved considerable success in the treatment of PsA and psoriasis.[16],[17],[18],[40],[41] Angiogenesis is a prominent early event in psoriasis and PsA. Elongated and tortuous vessels in the skin and joint suggest dysregulated angiogenesis, which results in immature vessels. TNF-alpha up-regulates angiogenic growth factors, including vascular endothelial growth factor, transforming growth factor beta (TGF-beta), platelet-derived growth factor and angiopoietins. The resultant neovascularization is an important component of the inflammatory and erosive nature of the disease.[39],[42] Abnormal bone remodeling is also a key feature of PsA. TNF-alpha contributes to the increased production of proteases such as matrix metalloproteinases, which are involved in cartilage destruction. Joint-space narrowing, joint erosions as well as osteolysis of digital tufts and joint space occur. There is also juxta-articular periosteal new bone formation and ankylosis. An increase in the differentiation of monocytes into osteoclast precursor cells and then to mature osteoclasts via the action of TNF-alpha was demonstrated. There are receptors that activates nuclear factor kappa-beta ligand (RANKL) and IL-1 in the synovium-bone interface which in terms, mediate the bone resorption.[43] In the skin, keratinocytes proliferate and have prolonged survival under the influence of proinflammatory cytokines such as TNF-alpha. As a result, there is skin thickening and plaque formation. TNF-alpha activates endothelial cells to express adhesion molecules such as intercellular adhesion molecule-1 (ICAM-1), vascular adhesion molecule-1 (VCAM-1) and E-selectin, which promote lymphocyte migration to sites of inflammation.[9] Cutaneous lymphocyte-associated antigen is expressed on lymphocytes homing to skin lesions.[44] Burden of Disease PsA characteristically develops in young adults aged 35-55 years. Men and women are equally affected. The spectrum of the severity of PsA is broad, ranging from mild degree of joint pain or stiffness to severe deformities. Psoriatic arthritis was once thought to be a benign condition; it is now well recognized as a cause of chronic joint damage, increased disability,[45] decreased quality of life (QoL)[46] and increased mortality.[29] The commonest cause of death is cardiovascular diseases. The risk for premature death is related to previously active and severe joint disease, presence of erosions and a high erythrocyte sedimentation rate at presentation. There are also social and financial implications to the society, including impact on medical burden and inability to work.[47] Study of PsA has lagged behind that of other arthropathies. With the availability of new therapeutic options, there is rising interest for research in PsA. Treatment Treatment of PsA should be individualized balancing risk associated with active disease and likelihood of progression in peripheral joints, spine, enthesis, skin and the impact on physical function and QoL. Patients with mild joint symptoms and lack of progressive joint damage are usually treated with NSAIDs or intra-articular corticosteroid injections. However, oligoarticular joint involvement is not necessarily benign. A single joint could be persistently inflamed with progressive erosive changes leading to disability, which may warrant systemic disease-modifying anti-rheumatic drugs (DMARDs). Similarly, patients with mild skin disease may be treated with topical corticosteroid or vitamin D preparations. There are situations in which systemic therapy may be warranted in minor skin lesions involving the face or hands and compromising a patient's activities. NSAIDs have been used for symptomatic control in patients with PsA and there are some data showing their efficacy. Corticosteroids have not been subjected to controlled trials in PsA patients. Intra-articular injection of corticosteroid can be of value in the management of patients with oligoarticular disease. While there is a potential risk of flare of skin psoriasis upon withdrawal of steroid, clinicians have been using low-dose oral corticosteroids for patients with PsA as they do for patients with RA. Conventional DMARDs have been used in PsA over the years. Salfasalazine, leflunomide, methotrexate (MTX) and cyclosporine A have been shown to be of benefit for psoriasis and peripheral arthritis of PsA, although the evidence is quite weak. These traditional DMARDs have not been successful in improving spondylitis symptoms and their impact on radiographic progression has not been adequately assessed. No data exist that demonstrate their efficacy in enthesitis or dactylitis. The potential hepatotoxicity is an additional concern with use of MTX in PsA. In a meta-analysis of serial liver biopsy studies, patients with psoriasis were three times more likely to have histological liver damage as compared to patients with RA.[48] There is an essential difference in the concern about MTX-related hepatic adverse effects between dermatologists and rheumatologists. Dermatologists recommend routine liver biopsies with every 1.5 g of cumulative dose of MTX, while most rheumatologists do not recommend this approach. The reasons for greater hepatic side-effects in patients with psoriasis are unknown. The greatest excitement for clinicians with regard to PsA is about its novel treatments and therapeutic strategies. Based on greater understanding of immunology and pathogenesis of the disease along with progress in biopharmaceutical development, a new frontier in the treatment of PsA has emerged. Much data focus on anti-TNF-alpha. Results of 3 Phase III randomized controlled trials each used infliximab, etanercept and adalimumab in the treatment of PsA have been published. All three agents were approved for use in PsA by the United States Food and Drug Administration (FDA). Anti-TNF therapy is associated with an increased risk of infection, in particular tuberculosis. Proper screening for latent tuberculosis should be done before initiating treatment and treatment of latent tuberculosis should be initiated before anti-TNF treatment. Etanercept Etanercept is a soluble TNF receptor-IgG fusion protein. The usual dose for RA is 25 mg, subcutaneous twice weekly or 50 mg weekly. The Phase III trial in PsA with etanercept using the RA dose was evaluated in 205 patients, 41% of who were on background methotrexate. At week 12, 59% of the etanercept group met the American College of Rheumatology 20% improvement criteria for joint response (ACR20), compared with 15% of the placebo group ( P < 0.0001) and results were sustained at 24 and 48 weeks. At 24 weeks, 23% of the etanercept group achieved at least 75% improvement in the psoriasis area and severity index (PASI75), compared with 3% of the placebo group ( P = 0.001). Psoriasis Area and Severity Index (PASI) is a measure of overall psoriasis severity and coverage and is a commonly used method to evaluate the clinical efficacy of a new treatment for psoriasis.[49] The cutaneous psoriasis lesions are scored on a scale of 0 to 4 for three characteristics: erythema, induration and desquamation; and in four anatomical regions: head, trunk, arms and legs. The index ranges from 0 (no psoriasis) to 72 (severe disease) [Table - 3]. Measures of function and quality of life also showed significant improvement in the treatment group. Inhibition of radiographic progression was evident in the etanercept group at 12 months; the mean annualized rate of change in the modified total Sharp score was -0.03 units, compared with +1.00 unit in the placebo group ( P = 0.0001).[40] These results were sustained at two years in a follow-on open label study.[41] Etanercept was well tolerated. Infliximab Infliximab is a human-mouse chimeric monoclonal antibody that neutralizes both soluble and membrane-bound TNF-alpha. Infliximab is typically administered as an intravenous (IV) fusion at baseline, two weeks and six weeks and then every six to eight weeks thereafter with dosages ranging from 3-10 mg/kg. Two hundred patients with active PsA unresponsive to previous treatment were assessed in the Phase III Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT II). At week 14, ACR20 and Psoriatic Arthritis Response Criteria (PsARC) were achieved by 58% and 77% in the infliximab group and 11% and 27% in the placebo group at week 14 (both P < 0.001). Significant response in the skin psoriasis by PASI, dactylitis and enthesopathy assessments was also demonstrated.[16],[17],[18] Infliximab is the only anti-TNF agent that demonstrated efficacy in the reduction of dactylitis and enthesitis. Continued inhibition of radiographic progression was shown in the extension trial. Patients on placebo were given infliximab treatment after week 16. At week 50, 85% and 84% of patients in the placebo/infliximab and infliximab/ infliximab groups had no worsening in radiological progression as measured by the PsA-modified van der Heijde-Sharp (vdH-S) score as compared to the estimated mean annual rate of 5.8 PsA-modified vdH-S points per year.[50] Aminotransferase increase occurred more frequently in the treated group than placebo group, which was usually mild. Markedly abnormal alanine transaminase (ALT) and/or aspartate transaminase (AST) values (predefined as> 150IU/l and> 100% increase from baseline) were reported in five patients in the infliximab group and required discontinuation. Four patients had ALT/AST levels returned to normal, one patient was lost to follow-up. One of the five patients was receiving concomitant methotrexate.[17] Adalimumab Adalimumab is a fully humanized anti-TNF monoclonal antibody. The typical dosage for RA is 40 mg subcutaneous every other week. A large placebo-controlled trial (ADEPT) evaluated 313 patients with active PsA. Methotrexate was allowed but not required and was used by 50% of the patients. At Week 12, 58% of the adalimumab-treated patients achieved an ACR20 response, compared with 14% of the placebo-treated patients ( P < 0.001). The results were maintained at week 24. A tendency of improvement in dactylitis and enthesitis was observed but did not reach statistical significance. Radiographic progression was prevented with the mean change in the modified total Sharp score -0.2 in adalimumab-treated patients and 1.0 in placebo-treated patients ( P < 0.001). Fifty-nine per cent achieved a 75% PASI improvement response at 24 weeks, compared with 1% of the 69 placebo-treated patients evaluated ( P < 0.001). Disability and quality of life measures were also significantly improved with adalimumab treatment compared with placebo. Adalimumab was generally safe and well tolerated.[18] Safety of anti-TNF medications In general, anti-TNF medications are well tolerated, but some adverse effects can be significant and life-threatening. The biologics can cause administration reactions. A third of the patients using etanercept have mild and short-lived injection-site reactions which resolve with continued use. Adalimumab can also cause injection-site reactions, although less frequently.[51] Infliximab infusions reactions are usually mild and modulated by slowing the infusion rate or pretreatment with antihistamines and antiinflammatories. Rarely, severe reactions, such as bronchospasm, hypotension, fever or chest pain may occur requiring stopping the infusion and administering appropriate medical treatment.[52] Severe and problematic bacterial infection can occur with anti-TNF-alpha therapy. Careful surveillance for infection and early and aggressive treatment are warranted. Opportunistic infections occur more frequently in patients treated with anti-TNF-alpha. Tuberculosis (TB) is a particular concern in Asian countries where the prevalence of TB remains high. One half of the cases of tuberculosis associated with anti-TNF-alpha therapy were extrapulmonary and a quarter was disseminated.[53] Speculatively, this is related to the role of TNF in maintaining granuloma formation.[54] The risk associated with the monoclonal antibody against TNF, infliximab, was higher than that associated with the TNF fusion protein etanercept. As in case of adalimumab proper screening and treatment of latent TB infection prior to anti-TNF therapy was shown to be effective in reducing the incidence of TB.[55],[56] The risk of other granulomatous infections including histoplasmosis, listeriosis, candidiasis and coccidioidomycosis was also increased in patients who received anti-TNF therapy.[57] Other rare adverse events associated with anti-TNF therapy include elevation of liver enzyme, exacerbation of congestive heart failure, multiple sclerosis, theoretical risk of malignancy like lymphoma and occurrence of autoimmune anti-chimeric antibodies. Other biologic agents like alefacept and efalizumab were approved by the FDA for use in the treatment of psoriasis. Alefacept is a fusion protein of the binding site for leukocyte-function-associated antigen 3 (LFA-3) with the Fc segment of human IgG. It binds to CD2 on activated T cells and impairs the co-stimulatory signals delivered by LFA-3 and induces apoptosis in circulating memory T cells. Recently, a Phase II trial has proven its efficacy in the treatment of both joint and skin diseases despite the fact that its efficacy for joint disease was very limited.[58] Efalizumab is a humanized monoclonal antibody direct against an extracellular epitope of the LFA-1 (alpha) chain. It prevents the interaction between LFA-1 on the T cell surface and ICAM-1 on the endothelial cells thus decreasing T cell migration. It is FDA approved for use in psoriasis. However, a Phase II trial in 107 patients with PsA failed to show a statistically significant difference between treated and placebo patients.[59] Conclusion PsA is a chronic systemic inflammatory disease involving peripheral joints, spine or enthesis and is associated with psoriasis. It is now recognized as a distinct disease entity separated from other chronic arthropathies. Unique clinical features include distal phalangeal joint involvement, enthesitis, dactylitis, asymmetrical spondylitis, specific radiological ankylosis and osteolysis, specific psoriasis skin and nail lesions. PsA affects young adults and may be progressive, destructive, causing deformities, and impaired functional status and quality of life. Anti-TNF therapy has achieved encouraging efficacy in alleviating signs and symptoms in both the joints and skin, improving function and quality of life and inhibiting radiological progression measured in patients with PsA and psoriasis. The potential benefits of anti-TNF therapy should however, be balanced against the risk of serious infection, tuberculosis and its high cost. Lastly, we still have 40% of patients with PsA who cannot achieve a clinically significant response with the latest advance. With the emerging knowledge in pathogenesis, we are waiting for methods that assist in stratifying patients who would be best benefited from these biologic agents. Numerous other biologic agents and immune-response modifiers are under development. These compounds have the potential to address some of the unmet medical needs in the treatment of PsA and psoriasis[60]. References
Copyright 2007 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp07022t2.jpg] [jp07022t1.jpg] [jp07022f2.jpg] [jp07022f1.jpg] [jp07022t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}