 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
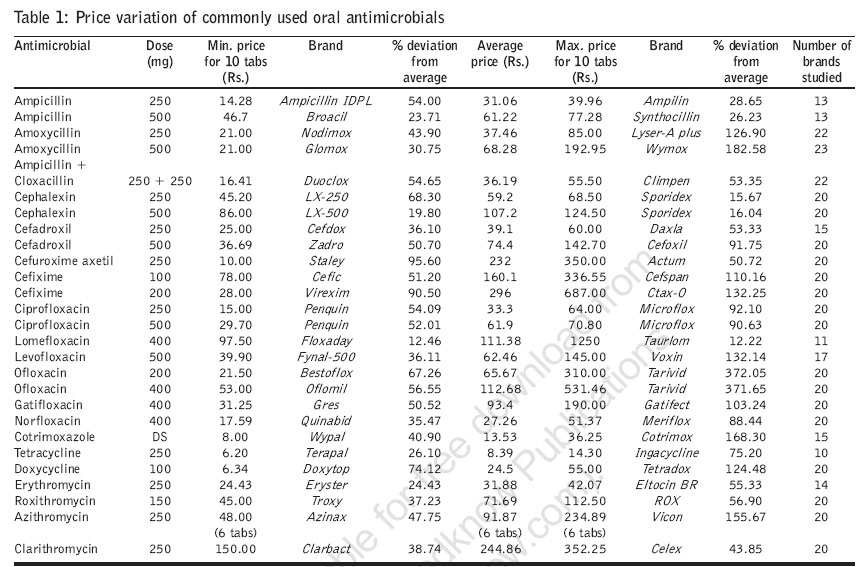
Journal of Postgraduate Medicine, Vol. 53, No. 1, January-March, 2007, pp. 72-74 View Point Antimicrobial price variation: Conundrum of medical profession! Rataboli PV, Dang A Dept. of Pharmacology, Goa Medical College, Goa Date of Submission: 25-Jul-2006 Code Number: jp07023 Abstract Pharmacoeconomics plays a pivotal role in clinical practice. High medicine prices can adversely affect a patient's finances and compliance. The Indian pharmaceutical industry has become a cornucopia of medicines with wide variation in prices for the same medicine marketed under different brand names. Price list of available antimicrobial brands was procured from a commercial drug directory. Average price of widely prescribed oral antimicrobials was found and price variation between different brands was calculated. The variation in medicine prices was found to be from 95% lower to more than 350% higher than the average price. Implications of price variation in clinical practice are discussed and remedial measures suggested.Keywords: Medicine pricing, oral antimicrobials, pharmacoeconomics Pharmacoeconomics identifies, measures and compares the costs, and consequences of pharmaceutical products and services.[1] High cost of medicines has economic implications for the patients and patient compliance may be significantly dependent on the cost of medicines prescribed. In addition to the confusing brand names of various medicines in the Indian market,[2] price variation poses a dilemma for practicing doctors. In case of many medicines there is a wide difference in the prices between different brands, which could be twofold to more than 100-fold.[3] It is not always easy for the practitioner to decide which brand to prescribe by merely considering the medicine price. Antimicrobials are commonly prescribed medicines. We compared the price of some branded antimicrobials to find their price difference when compared to the average price. The prices of the available antimicrobial brands were downloaded from the IDR site (IDRMedCLIK@MedCLIK. com). Brands of 20 most commonly used oral antimicrobials were selected and their maximum retail price (MRP) without addition of local taxes was used for comparison. Average price for an antimicrobial was calculated by adding the price of all its brands studied, divided by the number of brands. The minimum and maximum price for each antimicrobial formulation of same concentration was noted and percentage variation in price was calculated from the average price. [Table - 1] shows the price variation of a few commonly used antimicrobials. Among aminopenicillins, Wymox was the costliest brand of amoxycillin 500 mg with 182.58% higher price than the average price. Similarly, Lyser-A plus has 126.9% higher rate than the average price of amoxycillin 250 mg capsules. Ampilin (28.65% higher) and Synthocillin (26.23% higher) were the costliest brands of ampicillin 250 mg and 500 mg respectively. The ampicillin-cloxacillin combination Duoclox was the cheapest brand. Cefixime showed the maximum price variation among the cephalosporins. Virexim was one of the cheapest 200 mg brands and CTAX-O was the costliest with 132.25% higher price than the average. Among fluoroquinolones, the maximum variation in prices was in the two strengths of ofloxacin viz. Tarivid , the prices of which for 200 mg and 400 mg were Rs. 310 and Rs. 531.46 respectively. The cheaper brands of ofloxacin namely Bestoflox (200 mg) cost as low as Rs. 21.5 and Oflomil (400 mg) was priced at Rs. 53. The deviation of price was more than 300% towards the higher side as compared to the average prices of both strengths. Azithromycin brands also showed more than 150% variation on the higher side as compared to the average price, with Vicon costing Rs. 234.89 as compared to the average price of Rs. 91.87. Discussion Our findings reveal that the prices of various antimicrobial brands show great variation with the difference being from 95% lesser to more than 350% higher than the average price. The mean price was considered to be the most appropriate price parameter for comparison because prices of 80% of the drug brands revolved around the mean price. In India, in 1979, 80-85% of the drugs in the market were under price control. The number has slowly decreased and by 2002 only 15-20% drugs were under price control.[4] The common man therefore has to shell out more money with medicine prices spinning out of his reach. The clinicians in addition to remembering the pharmacological and trade names also have to remember the prices of various brands. There is a general feeling that a very low-priced drug although affordable may not fulfill the bioavailability standards expected of a good brand and a high-priced drug could be better. However, pricing does not give any assurance of the product′s quality, although most of the companies are careful about quality control.[5] The implications of such price differences are: a) With over 64,000 brands of various medicines being sold in the market, the doctor has a big range to choose from. Medical representatives vie for his prescription and decision-making is difficult.[6] b) It is reported that the pharmacists do not dispense the same brand as prescribed by the doctor and try to substitute it with other alternatives, quoting the reason of nonavailability. This is often done with vested interest for economic gains as some brands have a higher profit margin. Pharmaceutical companies may also offer more remuneration to a pharmacist for stocking only their higher priced item rather than generics.[7] c) Literate patients through word of mouth get to know about cheaper brands of medicine and change the brand on their own. This may result in variation in bioavailability and response.[8] d) Smaller private pharmacies usually stock only a few brands, forcing the patients to choose from these.[6] e) Patients may be noncompliant to the expensive brands and take a lesser dose to save money without realizing that reduced dosage will decrease the therapeutic response. Interaction with leading practitioners confirms this point. f) Lesser known companies are known to price their products lower than well-established brands to promote their product economically thus indirectly aiding the doctors to prescribe cheaper versions. The medical representatives try to push their products using incentives.[7] Also, most of the pharmacies are forced to sell the drugs at a very lean margin as a neighbor pharmacist may sell the same for a good undercut in prices.[8] Currently, very few medicines are under drug prices control order.[9] Hence it is desired that the Government should bring all lifesaving and essential medicines under price control. A company with an innovator brand may be allowed to have a higher reasonable margin. Bioequivalence reports comparing the marketed brand with the innovator brand should be made mandatory. The current practice of adding taxes on the printed MRP should be stopped and the prices should be standardized by incorporating the applicable sales tax so that the customers will not be subjected to price variation in the same medicine brands across the country.[9] Organizations like low cost standard therapeutics have suggested that all brand names should be abolished and medicines should be sold only under generic names. This would also decrease the possibility of medication errors due to look-alike and sound-alike brands.[2] The medical practitioners have to keep in mind the link between quality and price. In an agreement between the industry and trade, the retailer is entitled to a margin of 16-20% of the MRP that is printed on the medication. The stockist gets between 8-10% of his sale price to the retailer.[6] Advertisements and medicine promotion prop the brands and a huge amount of money is spent. All such expenditure is passed on to the customer making some drugs very expensive.[10] Certain companies operate monopolistically and use various marketing strategies for the benefit of doctors. Thus, even if the prices are high, their products are prescribed and the customer is always at the receiving end.[5] Giant pharmaceutical companies realizing the competitive nature of the drug industry have started producing the same drug under various brands and sell them at different rates to capture different market segments.[5] In India, prescribing pharmacists also recommend the medicine to the patient.[11] More than 60% of the patients consult chemists rather the doctors to decide as to which medicine(s) to buy.[9] Hence the pharmacists can play a vital role in intervention. A reactive intervention can be undertaken after a prescription has been written. Upon receiving the prescription, the pharmacist recognizing the potential for improved therapy can initiate one of the following: a nonfill of the prescription, a change of medication or a termination of therapy and discuss the same with the doctor. In contrast, a proactive intervention involves a scheduled visit by the pharmacist to the physician and possibly subsequent reinforcing contacts, to present and review therapeutic alternatives to influence prescription behavior at the point of prescribing.[12] However, such interventions seem too farfetched in the Indian context. It is recommended that the appraisal and management of marketed drugs should be directed toward maximizing the benefits of therapy and minimizing negative personal and economic consequences.[13] References
Copyright 2007 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp07023t1.jpg] |
| |||||||||

{kind=link}