 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
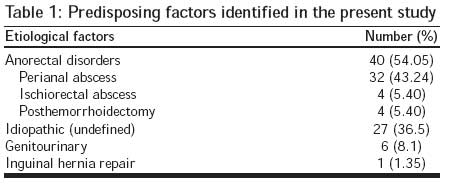
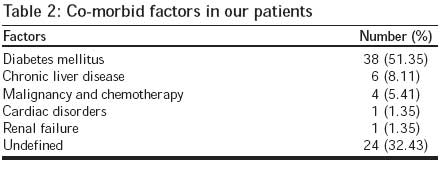
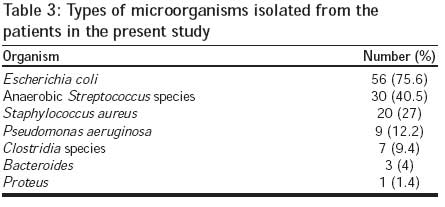
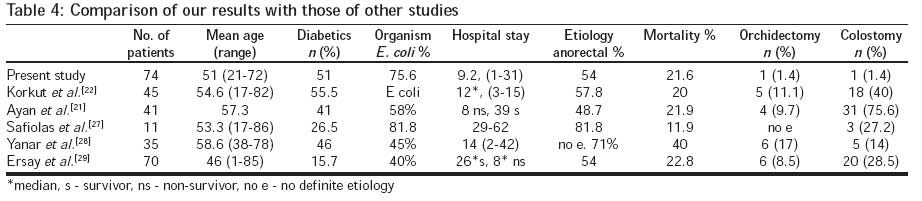
Journal of Postgraduate Medicine, Vol. 54, No. 2, April-June, 2008, pp. 106-109 Original Article Fournier's gangrene in Mansoura Egypt: A review of 74 cases Ghnnam WM Department of General Surgery, Mansoura Faculty of Medicine Code Number: jp08041 Abstract Background: Fournier's gangrene (FG), caused by synergistic aerobic and anaerobic organisms, is a life-threatening disorder in which infection of the perineum and scrotum (can affect penis alone) spreads along fascial planes, leading to soft-tissue necrosis. Despite antibiotics and aggressive debridement, the mortality rate of FG remains high. Keywords: Fournier′s gangrene, idiopathic, necrotizing fascitis, outcome, perineal infections Fournier′s gangrene (FG) is a fulminant form of infective necrotizing fascitis of the perineal, genital or perianal regions, which commonly affects men, but can also occur in women and children. [1] Fournier′s gangrene is a life-threatening disorder in which infection of the perineum and scrotum spreads along fascial planes, leading to soft-tissue necrosis. Majority of infections arise from the anorectal, genitourinary, and cutaneous sources. FG shows vast heterogenicity in clinical presentation, from an insidious onset and slow progression to rapid onset and fulminant course; the latter being the more common presentation. The patients usually present with erythema, pain, and swelling of the perineal, genital or perianal regions. There is often crepitus and areas of gangrene or blister formation on the skin. It is believed that systemic conditions such as diabetes mellitus (DM), alcoholism, paralysis or neurological deficit, malignancy and debilitated and immunosuppressed individuals are predisposed to the development of this entity. Prompt recognition of the condition, urgent radical surgical debridement, and the use of appropriate antibiotics form the mainstay of management. Despite antibiotics and aggressive debridement, the mortality rate with FG remains high. [2],[3],[4],[5] In the present study, we analyzed patients admitted to our institution′s emergency surgical unit presenting with FG noting the location of infective gangrene, predisposing factors, etiological agents and outcomes. Materials and Methods All patients diagnosed with FG admitted at the Trauma and Surgical Emergency Unit, Department of Surgery, Mansoura Faculty of Medicine, Mansoura University, Egypt, were included in this study between January 2002 and January 2007. A review of the medical records of those patients was performed noting age, gender, etiology, predisposing factors, duration between the onset of symptoms and surgery, culture findings, and clinical outcome. The general condition of the patients was noted, with special emphasis on the level of consciousness, temperature, heart and respiratory rates, and blood pressure. Laboratory parameters, such as white blood cell count (WBC), serum creatinine, and albumin, were studied. Presence of confusion, hypotension (systolic BP< 80mmHg), leukocytosis (>15,000), and fever (>38°C) were considered as sepsis criteria. Mortality was defined as disease-related death during the hospital stay and survival was measured in days. The prognostic variables analyzed were the patient′s age, sex, source of infection, existence of co-morbidities, the duration of symptoms, clinical and laboratory findings, bacterial organisms cultured from wounds and hospitalization time. Statistical analyses were carried out by using the statistical packages for SPSS 10.0 for Windows (SPSS, Chicago, IL, USA). Mean and SDs were calculated for continuous variables and median values were calculated for discrete variables. Results All the 74 patients included in this study were males. The mean age of our patients was 51±10.8 years (range: 21-72years). Themean duration from the onset of symptoms to admission to the hospital was 3.74±2.09 days (range: 1-8 days). Furthermore, the mean hospitalization time was 9.2±6.6 days (range: 1-31days). The diagnosis of FG was made from the clinical findings. Swelling and redness in the perineal area were observed in all patients. Other clinical findings included edema, indurations, partial necrosis, gangrenous patches of the skin, and crepitation. Sepsis was observed in 32 (43.2%) patients. Atotal of 16patients with sepsis (50%) died. Forty patients (54.05%) had FG secondary to anorectal conditions - perineal abscess (32), ischiorectal abscess (4), and posthemorrhoidectomy (4). No etiologic factors for FG were found in 27 (36.5%) patients and they were classified as idiopathic FG. Six patients (8.1%) developed FG secondary to urogenital infections (scrotal abscess in five patients and one following scrotal trauma), and one patient (1.35%) developed FG following inguinal hernia repair [Table - 1]. Most of the patients had one or more than one predisposing disorders for FG. These included DM in 38 patients (51.35%), chronic liver disease in 6 patients (8.11%), malignancy and chemotherapy in 4 patients (5.41%), cardiac disorders in 1 patient (1.35%), renal failure in 1 patient (1.35%), and no definite predisposing factor in 24 patients (32.43%) [Table - 2]. Infection was present on the scrotal and perianal regions bilaterally in 62 patients, extending to the lower abdomen in 10 patients and there was an extension to unilateral or bilateral femoral regions in two patients. Seven patients (9.45%) were unconscious on presentation. According to tissue samples taken during debridement, the microbiological etiology of FG was polymicrobial in 48patients (64.8%) and monomicrobial in 26 patients (35.1%). The microorganisms isolated on cultures are shown in [Table - 3]. Although subcutaneous emphysema was observed clinically in 64 cases, only 30 cultures presented anaerobic bacteria. The most frequent bacterial organisms cultured from the wounds were Escherichia coli (75.6%), anaerobic Streptococcus species (40.5%), Staphylococcus aureus (27%), Pseudomonas aeruginosa (12.2%), Clostridia species (9.4%), Bacteroides (4%) and Proteus (1.4%). Before surgery, all patients underwent aggressive fluid resuscitation and were treated mostly with parenteral broad-spectrum triple antimicrobial agents, using a third-generation cephalosporin, an amino glycoside and metronidazole and received hemodynamic support when required. Mechanical ventilation, continuous monitoring, and inotropic support were applied when necessary in patients with cardiopulmonary failure due to sepsis. Following the optimum radical and aggressive debridement, all necrotic skin, subcutaneous tissue, fascia, and obviously non-viable muscle were removed and sent for microbiological examination. The areas of debridement were initially irrigated by hydrogen peroxide, then saline, and packed with dressings soaked in povidone-iodine and glycerin manesia (glycerin and magnesium hydroxide). After the initial surgery, the wound was closely monitored, adequate nutrition was ensured to support wound healing and early enteral feeding was considered. Patients underwent repeated debridement, two or more days after the first and further necrotic tissues were debrided when needed under local or no anesthesia. Closure of wounds was commenced as soon as healthy, viable tissue allowed re-approximation. If necessary, split-thickness skin graft or rotational cutaneous flaps were also used to repair large defects. Colostomy was carried out for fecal diversion when the source of infection originated from the anorectum and the wound was likely to be contaminated by feces. If penile skin was affected, split-thickness skin graft was carried out with skin from the inguinal area. Multiple resection procedures were carried out in 24 (32.4%) cases. Simple sigmoid loop colostomy was carried out in one patient (1.4%). In addition to scrotal resection, unilateral orchidectomy was done because of necrosis in the testicle in one case (1.4%). Nearly all survived patients′ wounds healed by secondary intention or were managed by local advancement or rotational flaps. Skin grafting was reserved only for cases with lost penile skin without available local skin cover. One patient developed right inguinal hernia one year later and was treated successfully with mesh hernioplasty. The overall mortality rate was 16 patients (21.6%); all of them presented with sepsis syndrome in addition to local signs of FG, 14 of them had diabetes; 10 were over 55 years of age and seven of them had late admission to hospital. Discussion Fournier′s gangrene was first described by Fournier in 1883 as an idiopathic condition, but in most cases a perianal infection, urinary tract infection, and local trauma or a cutaneous source can be identified. In our study, anorectal causes were the most leading cause (54%), next was idiopathic (36.5%) followed by genitourinary (10%) and these findings are in agreement with published literature. The illness is more frequently seen in men with poor hygiene, diabetes, paraplegia, cirrhosis and in alcoholics. [6],[7],[8],[9],[10] The findings from the present study support these results because all our patients were males, 51.35% of them were diabetics, 8% had chronic liver disease (no one was an alcoholic because of social and religious factors), although one study reported that diabetes is not a prognostic factor in the outcome. [11] In our study, various bacteriologic agents have been identified in patients with FG. It is known that multiple organisms can be identified from each wound culture. Gram-negative enteric bacilli and Gram-positive cocci have been identified in the majority of patients. [12],[13] Colostomy is sometimes needed to decrease fecal contamination, especially so in the presence of infective sphincteric destruction or rectal perforation. [14],[15],[16],[17],[18] Adequate urinary diversion can usually be accomplished by a Foley′s catheter unless urethral disruption or stricture coexists. In such situations, cystostomy is needed. [17],[19] Fecal diversion was needed only for one of our patients and suprapubic cystocatheter was needed in another one with urethral injury. In a retrospective review of 29 patients over a 13-year period, Baskin et al. [20] reported that only three patients (all more than 65 years of age) underwent orchidectomy. The authors deduced from previous records that the testes were removed not because of ischemia but because of extensive tissue damage in the surrounding scrotum, groin, and perineal area, advanced age and difficulty in dressing. They added that it is unusual for the testis to be necrotic; indeed they were unable to document necrosis in any of their 29 patients. In a recent study by Ayan etal. , who retrospectively reviewed records of 41 patients, bilateral orchidectomy were done in four (9.7%) patients and unilateral orchidectomy in five (12.1%) patients due to necrosis. [21] This study though reported testicular gangrene with FG, but did not throw any light on the cause and pathogenesis of testicular gangrene. In a review by Smith et al ., orchidectomy was done in 21% patients but in most cases, the indications of orchidectomy were preexisting epididymorchitis or scrotal abscess. [1] Eke reviewed 1726 FG cases and stated that testicular involvement was rare and when it occurs, it indicates retroperitoneal or intraabdominal source of infection. [3] In our study, only one patient had unilateral orchidectomy because of gangrenous testis and no one needed subcutaneous testicular repositioning. We agree with Eke′s explanation in that the patient for whom we did orchidectomy had extensive lower abdominal gangrene. Early diagnosis, antimicrobial treatment with broad-spectrum combinations followed by prompt surgical debridement is the recommended management of FG. [3],[6],[7] Even with this sequence of treatment approaches, mortality is high, 4 to 67%. [8],[22],[23],[24],[25] These as mortality rates are due to the rapid progression of the disease associated with sepsis and the presence of other co-morbid illnesses. In our study, the overall mortality rate was 21.6%, and mortality rates were found to be the highest in patients presenting with sepsis, with DM and late admission to the hospital, in accordance with previous studies [26],[27] [Table - 4]. Conclusion FG is a rapidly progressive, fulminant infection. Nevertheless, surgical debridement must be extensive and, if necessary, serial. Even with aggressive surgical and medical treatment, mortality of the disease is high. In the present cases, such a high ratio of 21.6% means that this disease is still serious and fatal in Egypt. For this reason, advanced studies may be necessary to decrease this high mortality rate and perhaps find an alternative effective management policy.References
Copyright 2008 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp08041t4.jpg] [jp08041t3.jpg] [jp08041t2.jpg] [jp08041t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}