
|
Journal of Postgraduate Medicine
Medknow Publications and Staff Society of Seth GS Medical College and KEM Hospital, Mumbai, India
ISSN: 0022-3859 EISSN: 0972-2823
Vol. 54, Num. 2, 2008, pp. 115-125
|
Journal of Postgraduate Medicine, Vol. 54, No. 2, April-June, 2008, pp. 115-125
Review Article
Present status of understanding on the genetic etiology of polycystic ovary syndrome
Dasgupta S, Reddy BMohan
Molecular Anthropology Group, Biological Anthropology Unit, Indian Statistical Institute, Habsiguda, Hyderabad - 500 007
Correspondence Address:Molecular Anthropology Group, Biological Anthropology Unit, Indian Statistical Institute, Habsiguda, Hyderabad - 500 007
bmr@isical.ac.in
Code Number: jp08043
Abstract Polycystic ovary syndrome (PCOS) is the most common endocrinopathy in women of reproductive age with a prevalence of approximately 7-10% worldwide. PCOS reflects multiple potential aetiologies and variable clinical manifestations. This syndrome is characterized by serious health implications such as diabetes, coronary heart diseases and cancer and also leads to infertility. PCOS can be viewed as a heterogeneous androgen excess disorder with varying degrees of reproductive and metabolic abnormalities determined by the interaction of multiple genetic and environmental factors. In this paper, we have attempted a comprehensive review of primarily molecular genetic studies done so far on PCOS. We have also covered the studies focusing on the environmental factors and impact of ethnicity on the presentation of this syndrome. A large number of studies have been attempted to understand the aetiological mechanisms behind PCOS both at the clinical and molecular genetic levels. In the Indian context, majority of the PCOS studies have been confined to the clinical dimensions. However, a concrete genetic mechanism behind the manifestation of PCOS is yet to be ascertained. Understanding of this complex disorder requires comprehensive studies incorporating relatively larger homogenous samples for genetic analysis and taking into account the ethnicity and the environmental conditions of the population/cohort under study. Research focused on these aspects may provide better understanding on the genetic etiology and the interaction between genes and environment, which may help develop new treatment methods and possible prevention of the syndrome.
Keywords: Epigenetics, ethnicity, hyperandrogenism, Indian scenario, insulin resistance, molecular genetic etiology, phenotypic heterogeneity, Polycystic ovary syndrome
Polycystic ovary syndrome (PCOS) is the most common endocrinopathy in women of reproductive age characterized by chronic anovulation or infrequent ovulation, obesity, hirsutism, hyperandrogenism and numerous follicular cysts in enlarged ovaries. PCOS is the leading cause of anovulatory infertility among premenopausal women. Such patients are also at increased risk for obesity, insulin resistance (IR), type-2 diabetes mellitus, premature arteriosclerosis and endometrial cancer. Consequently, PCOS has significant implications for the health and quality of life of these patients. PCOS was firstly reported as Stein-Leventhal syndrome in 1935, and since then has attracted more and more attention due to its genetic heterogeneity and diverse clinical manifestations. It has been used as an important clinical model to investigate the relationships among endocrine functions, reproductive activity and energy metabolism. [1]
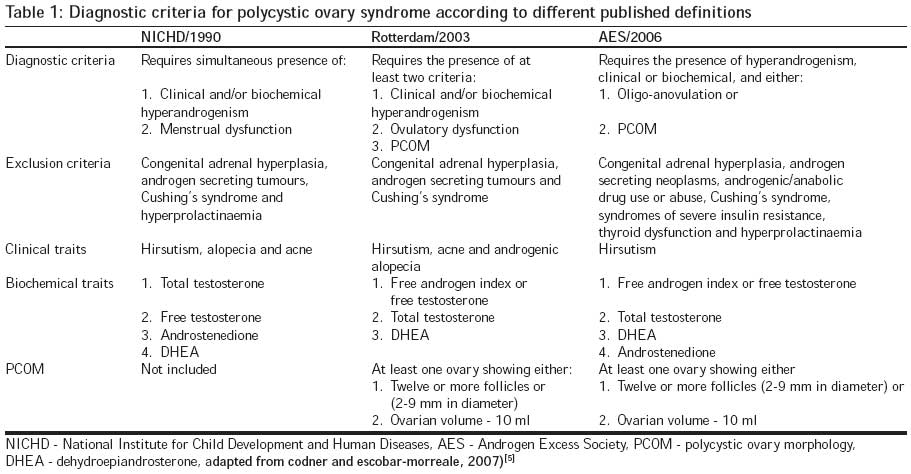
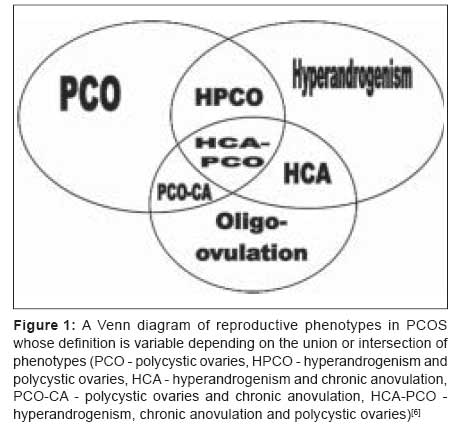
There is no consensus on the diagnostic criteria and definitions of PCOS. Until recently, two definitions were followed: one is the National Institute of Child Health and Human Development (NICHD) conference diagnostic criteria [2] and the other is suggested by the European Society of Human Reproduction and Embryology (ESHRE)/American Society for Reproductive Medicine (ASRM). [3] The third definition has been proposed recently by the Androgen Excess Society, which takes into account both the criteria existent till date. The three definitions are summarized in [Table - 1]. Diagnosing a woman as having PCOS implies serious health consequences and thus a judicious definition of PCOS is necessary to guide current and future research work. It is also now recognized that the definition of this syndrome will continue to evolve over time, incorporating new research findings. [4] The Venn diagram [Figure - 1] depicts the variability in clinical phenotypes characterizing PCOS cases.
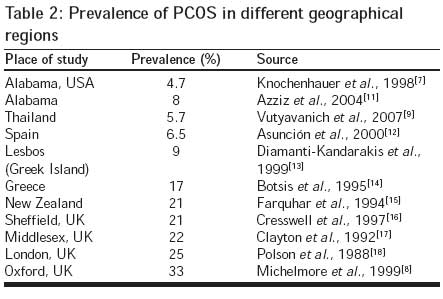
A number of studies have been performed to assess the prevalence of polycystic ovaries on ultrasound examination in the general female population of fertile age. A limited number of studies conducted so far [Table - 2] suggest that it is an extremely prevalent syndrome, which varies from about 5% in USA [7] to as high as 33% in UK. [8] Apart from the study conducted on Thai women, [9] all the others were largely on Caucasian populations; the prevalence rate of PCOS for black and white women in USA is not significantly different. [10]
Pathophysiology of PCOS and the Major Health Implications
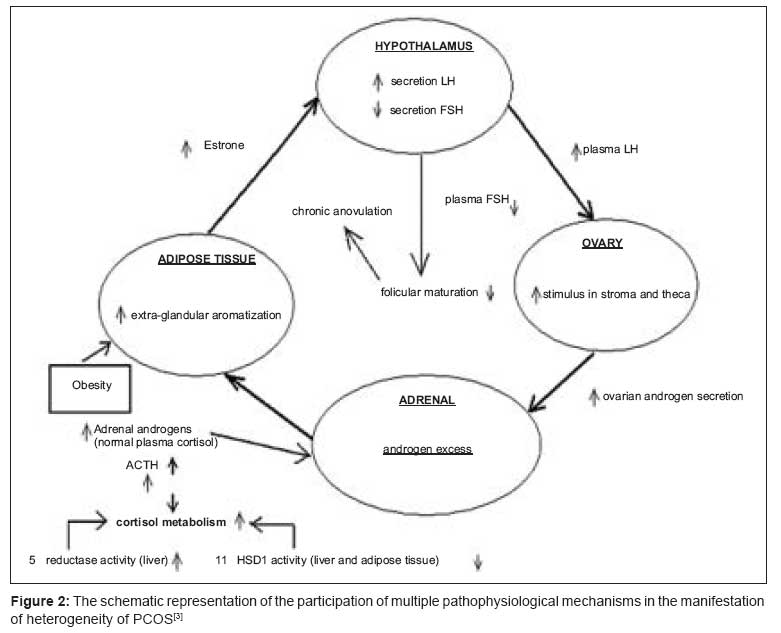
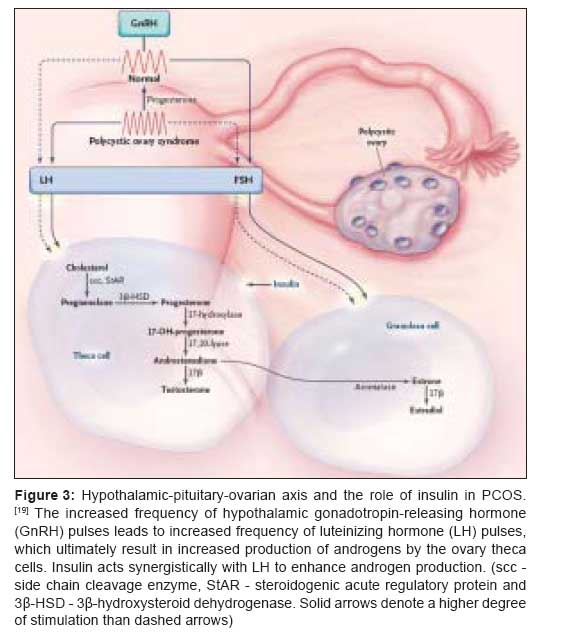
The pathological conditions result from the endocrine, metabolic and cardiovascular mechanisms. However, how much each mechanism contributes to developing PCOS is still unknown. The schematic representation of these mechanisms involved in the heterogeneous manifestation of the PCOS is presented in [Figure - 2]. The endocrine component specifically deals with the abnormal steroid synthesis from ovaries and adrenals resulting in high androgen levels. An inappropriate gonadotropin secretion is associated with the PCOS women exhibiting classic form of PCOS, i.e. hyperandrogenaemia, polycystic ovaries, chronic anovulation, hirsutism and obesity. On the contrary, the non-classical form is a more subtle condition usually found among lean women who manifest some of the above features associated with PCOS. Although androgens are obligate substrates for estrogen synthesis, an excess of androgens seem to interfere with the process of follicular maturation. Compared with the follicular phase of the normal menstrual cycle, women with PCOS exhibit a disproportionately high luteinizing hormone (LH) secretion with relatively constant low follicle stimulating hormone (FSH) secretion [Figure - 3]. The pattern of steroid secretion in polycystic ovary suggests a generalized dysregulation of ovarian androgen secretion, which is further augmented by insulin. PCOS is, thus, characterized by a metabolic disorder in which hyperinsulinaemia and peripheral IR are central features. The characteristic disturbances of insulin secretion and action are much more prominent in PCOS women with amenorrhoea or anovulatory menses than in equally hyperandrogenic women with regular cycles. [20],[21]
Insulin and FSH have a synergistic effect on estrogen production in granulosa cells from anovulatory PCO, which is not seen in the majority of ovulatory patients. Insulin also seems to produce a greater increase in androgen production by theca cells isolated from PCOS women than controls. [22],[23] Another common clinical feature of PCOS is obesity. Approximately 50% of PCOS women are overweight or obese. The history of the weight gain frequently precedes the onset of oligomenorrhoea and hyperandrogenism, suggesting a pathogenetic role of obesity in the subsequent development of the syndrome. [24] Endothelial dysfunction has been observed in PCOS women. Chronic inflammatory markers, such as TNF-α and Interleukin-6 (IL-6), promote IR and hyperandrogenism and therefore have been implicated in PCOS pathophysiology. [25] Women with PCOS also exhibit lower high-density lipoprotein (HDL) levels, higher triglyceride and higher low-density lipoprotein (LDL) levels than age- and weight-matched control women, which is responsible for the increased incidence of hypertension, coronary heart disease and thrombosis. [26] There is also an increased prevalence of endometrial hyperplasia and carcinoma in women with the PCOS. [27],[28]
Further studies are required to determine the incidence of such pathological conditions in PCOS women. Such women usually seek pre-emptive screening in their initial reproductive years, which is too early for the accumulative effects of some of these risk factors to culminate into the disease. Large multi-site simultaneous collaborative studies are necessary to evaluate the actual incidence and long-term health consequences of this syndrome. [29]
Etiology: Role of Genetic and Environmental Factors
Genetic background
Familial clustering of PCOS has been consistently reported suggesting that genetic factors play a role in the development of this syndrome, although PCOS cases do not exhibit a clear pattern of Mendelian inheritance. It is now well established that PCOS represents a complex trait similar to type-2 diabetes and obesity, and that both genetic and environmental factors contribute to the PCOS pathogenesis. Overall, PCOS can be viewed as a heterogeneous androgen excess disorder with varying degrees of gonadotropic and metabolic abnormalities. [2] However, there is strong evidence for a major genetic component in the etiology of PCOS. In families with PCOS cases, there is evidence for heritability of both hyperandrogenaemia and hyperinsulinaemia in affected siblings. [30],[31],[32] Numerous genetic mechanisms, including autosomal dominant, modified autosomal dominant, X-linked dominant and multifactorial, have been proposed, still, the precise mode of inheritance of PCOS has not been established. [33] It has been suggested that multiple loci and epigenetic modifications may play a role in the phenotype. [34] Family history, as a reflection of genetic risk, can also be considered as a risk factor and, therefore it is important for determining an individual′s risk of developing PCOS. [35]
Genetic models of PCOS
While most studies have focused on defining the characteristics of this disorder, a few have attempted to elucidate the genetic mechanisms behind the development of PCOS. The approach depends, to a significant degree, on whether the disorder is viewed as the combination of defects unique to this syndrome or as defects already present in the general population. [35] With this in mind, three general genetic models of PCOS have been proposed:
- The first one, termed as the "single-gene Mendelian" model, considers that the majority of the defects present in PCOS are unique. This model would suggest that the inheritance of PCOS should demonstrate a recessive or dominant pattern, indicative of a single-gene defect. If a dominant mode of transmission is assumed, all women who inherit the defect would develop clinically evident PCOS.
- The second model, termed "multifactorial", suggests that the defects present in PCOS are not unique to it, and this disorder simply represents the conglomeration of abnormalities already present in the general population. Under this concept, PCOS would be considered as a multifactorial genetic disorder such as NIDDM and CVD. Hence, women carrying multiple defects (both via inheritance and via environmental influences) would be at increasing risk of developing clinical PCOS.
- The third model, or the "variable expression-single gene" model, is a modified combined version of the above two models. Under this model, PCOS is caused by a major gene defect, which is transmitted to 50% of offspring. However, the expression of PCOS would then be modified by additional factors, both environmental and/or genetic (i.e. "genetic background"), so that the actual observed segregation ratio could be less than expected for an autosomal dominant disorder (0.5). Theoretically, women who possess the mutation would be at almost 100% risk of developing some degree of PCOS, although additional factors would determine the clinical severity of the disorder. Genetically predisposed women not exposed to these other influences might develop only subclinical forms of PCOS, or present with isolated diagnostic features seen in PCOS (e.g. hyperandrogenaemia only), but not the full disorder.
Methods used to study genetics of PCOS using candidate genes
The candidate gene approach relies upon improved molecular genetic techniques and statistical methods to analyze potential genes based on biological plausibility. Pathways that affect steroidogenesis, IR, gonadotropin function and obesity provide potential genes for investigation. [34] The finding of abnormalities in the earliest gonadotropin-independent stages of ovarian follicle development suggests that genes involved in folliculogenesis must also be considered as candidates for the etiology of PCOS. [32] To understand genetic etiology of PCOS, two mainstream approaches are employed: (i) association studies and (ii) linkage studies. Within these two approaches, three different study designs are adopted: (i) case-control study, (ii) affected sib-pair study (ASP) and (iii) transmission-disequilibrium test (TDT). Out of these three study designs, the case-control study design is mostly followed for the genetic analysis of PCOS. Genome-wide association studies are now feasible and can provide an additional means for identifying genes related to complex disorders. This approach combines the best features of linkage with the strength of association approaches. The whole genome scan approach utilizing the single nucleotide polymorphism (SNP) microarray gene chip technology brings the highest resolution in genetic mapping. Yet, there is no PCOS study published with this technique. In addition to this, the HapMap project brings further power to the association studies by genotyping over a million SNPs and characterizing patterns of genetic variation in linkage disequilibrium. [2]
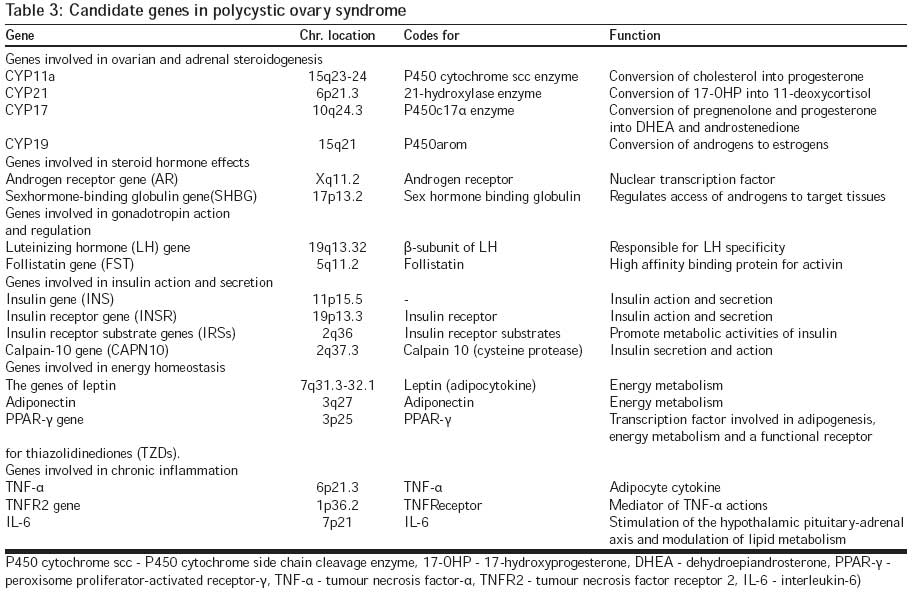
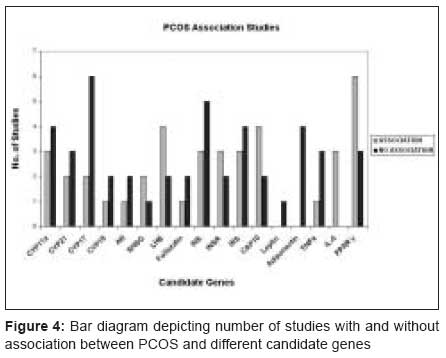
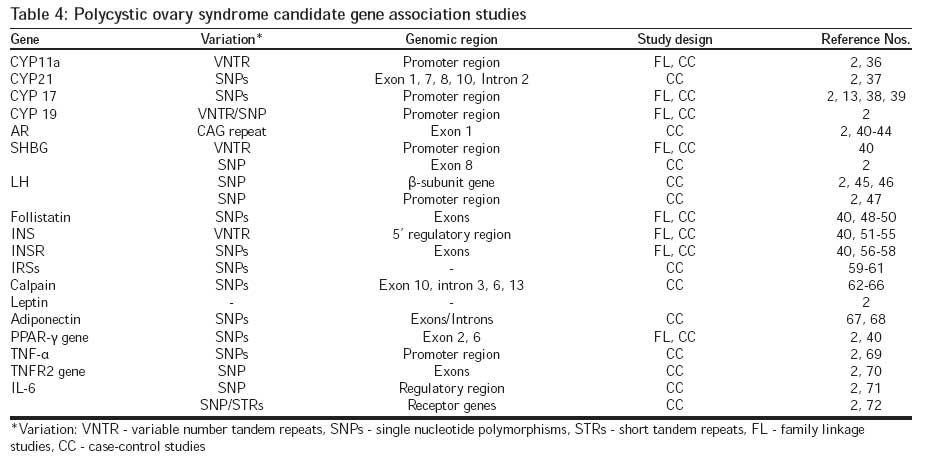
The candidate genes implicated in the etiology of PCOS along with their chromosomal location and functions are presented in [Table - 3]. A comprehensive review has been done by Unluturk et al. [2] for all the candidate gene association studies in PCOS. For most of the genes, there have been more negative results (i.e. no association with PCOS) than positive except for few genes as illustrated in [Figure - 4]. However, the inconsistent nature of data need not necessarily rule out the role of these candidate genes showing relatively lesser number of positive associations given that, overall, the major difference between the studies with and without significant association lies in the study design and the sample size. Most of the studies that have yielded positive results are case-control studies aiming at identifying SNP variation in various candidate genomic regions [Table - 4] and are based on large sample sizes. Therefore, future studies with candidate gene approach focusing on larger samples from genetically homogenous populations would be fruitful.
PCOS and epigenetics
Few studies have attempted to understand the etiology of PCOS through an epigenetic perspective by considering the X-chromosome inactivation (XCI) patterns in PCOS cases. These studies have taken into account the trinucleotide (CAG) repeat of the androgen receptor (AR) gene. Initially, Mifsud etal. [41] investigated the role of these CAG repeats in PCOS by undertaking a case-control study. A longer repeat stretch was observed in patients with high serum androgen levels than the patients with a lower serum androgen level. Another study compared the frequency distributions of CAG repeat alleles and their pattern of expression via X-inactivation analysis among 83 fertile women and 122 infertile women with PCOS. [42] The infertile women with PCOS exhibited a greater frequency of CAG alleles greater than 22 repeats compared to both the fertile control group and the general population. In families with PCOS, the above authors also examined the patterns of XCI between sister pairs with the same genotype at the polymorphic locus on the X-chromosome. [73] The findings warrant a closer inspection of X-linked genes in PCOS, one in which both genotype and epigenotype are considered. Examination of epigenetic modifications to the genetic code may be necessary to unravel some of the confounding complexities that have so far hindered the identification of causal genes for this disorder. [73]
Functional genomic studies
The functional genomic technologies, such as cDNA microarray, have been applied in various biologic studies to identify differentially expressed genes. To obtain a global view of those genes that might be involved in the development of PCOS, Diao et al. [1] used cDNA microarray technique to compare differential gene expressions between normal human ovary and ovaries from PCOS patients. A total of 9216 clones randomly selected from a commercial human ovary cDNA library were screened. Among them, 119 known genes showed differential expressions. These differentially expressed genes are involved in various biologic functions, such as cell division/apoptosis, regulation of gene expression and metabolism, reflecting the complexity of clinical manifestations of PCOS. Another recent study by Wood et al. [74] suggests for the first time that there are molecular abnormalities in PCOS oocytes, which could account, in part, for the reduced fecundity that characterizes PCOS. They examined whether the perturbations in follicle growth and the intrafollicular environment affect gene expression and ultimately development of the PCOS oocyte. The main feature of the outcome of this study was mRNA abundance of oocyte-expressed genes. Cluster analysis revealed differences in global gene expression profiles between normal and PCOS oocytes. Three hundred and seventy-four genes showed significant differences in mRNA abundance in PCOS oocytes, of which some were associated with chromosome alignment and segregation during mitosis and/or meiosis, whereas others contained putative AR and/or peroxisome proliferating receptor binding sites.
Male equivalent of PCOS
Complexity of the symptoms in close relatives of women with PCOS along with its probable autosomal inheritance pattern initiated a hypothesis about the existence of a male equivalent of PCOS. Although the male phenotype of PCOS is still not established and is one of the challenges for the genetic studies of PCOS, Duskovα et al. [75] suggested premature alopecia as one of the signs of a male phenotype of this syndrome. Their study investigated a group of 30 men, in which premature hair loss started before 30 years of age. Approximately one-third of the prematurely balding men expressed subnormal levels of serum hormone binding globulin (SHBG) and an imbalance between LH and FSH, like women with PCOS. Another finding of this study was a significantly higher frequency of decreased insulin sensitivity. Thus, a final proof of existence of the male equivalent of PCOS might be important not only for closer studies of pathogenesis and genetic background of PCOS, but also for general medical application. The occurrence of androgenic alopecia, especially before the age of 30 years, may be considered as a mark of potentially increased risks of serious diseases in the later age.
Challenges for genetic studies
Obstacles, such as phenotypic variability, lack of a male phenotype, multiple attempts at analysis and small sample sizes that hamper the efforts towards understanding the genetic basis of PCOS, are outlined in [Table - 5]. Nevertheless, great care must be taken to apply rigorous standards as we proceed with genetic studies. [34]
Environmental Factors
While clustering of cases in families strongly support the role of genetic factors in the development of PCOS, heterogeneity of phenotypic features in different families and even within the same family underscores the importance of the environmental contribution. [2] The highly variable phenotype of PCOS suggests that apart from genes other factors may contribute to the development of the disorder. These factors might include environmental influences such as fat and carbohydrate consumption, exercise level, peripubertal stress and/or hormonal exposure. [35]
Prenatal: Hormonal exposure in the uterine environment
The etiology of PCOS remains unclear and the heterogeneity of clinical and biochemical features has raised the question about whether PCOS represents the common end point of several aetiological factors. [76] Abbott et al. [77] have proposed a hypothesis, which states that PCOS is a genetically determined ovarian disorder characterized by excessive androgen production and that the heterogeneity can be explained on the basis of the interaction of this disorder with other genes and with the environment. This hypothesis is based on data from animal models and is supported by clinical studies. It is suggested that, in human females, exposure to excess androgen, at any stage from foetal development of the ovary to the onset of puberty, leads to many of the characteristic features of PCOS including abnormalities of LH secretion and IR. To sum up, exposure of the foetal hypothalamic-pituitary-ovarian axis to excess androgens influences the dynamics of early follicular development and can set up a train of events, which result in both the reproductive and metabolic consequences of PCOS.
Postnatal: Diet, nutrition and obesity
In postnatal life, the natural history of PCOS can be further modified by factors affecting the insulin secretion and/or action, most importantly, nutrition. Diet is a well-known factor playing a role in the regulation of sex steroid metabolism. Several studies have demonstrated that high-lipid and low-fibre diet is related to an increase in androgen circulating levels. [24] In some reports, PCOS women were found to have a higher intake of saturated lipids and a lower intake of fibres when compared to control groups. Low-fibre and high-lipid intake has been considered as one of the nutritional factors, which favour the onset and development of obesity in industrialized countries. Therefore, it can be speculated that a low-fibre and high-lipid diet may act negatively on sex steroid metabolism in selected groups of PCOS women, by increasing androgen availability and by favouring the development of obesity. [24] Obesity is a major feature in women with PCOS, and evidence suggests that obesity contributes to the pathogenesis of PCOS by aggravating the intrinsic IR of these women. [78]
Theories behind etiology of PCOS
Odunsi and Kidd [79] have put together the main theories that have been proposed in previous studies regarding etiology of PCOS.
- The luteinizing hormone-theca interstitial cell (LHTIC) theory suggests that the pathophysiologic mechanisms leading to abnormally elevated levels of LH underlie the phenomenon of PCOS. The theory suggests that high levels of circulating LH cause an increase in the growth of TIC in developing follicles, which leads to androgen overproduction and follicular atresia.
- The follicle stimulating hormone-granulosa cell (FSH-GC) theory suggests that the reduced FSH leads to subnormal induction of cytochrome P450 aromatase in the granulosa cells, leading to elevated androgen levels. This may be due to insufficient bioactive FSH in the follicular microenvironment to induce P450 aromatase gene expression, dysfunctional FSH receptor signal transduction mechanism, or the presence of inhibitors (such as epidermal growth factor and insulin-like growth factor (IGF)-binding protein 3) that prevent the normal expression of P450 aromatase activity.
- The third theory relates to the growth factor- autocrine-paracrine system. In PCOS, there is evidence of an altered IGF/insulin system, and these act as mediators of biologic responses of the selectogenic and atretogenic follicular hormones.
Evolutionary Perspectives and Impact of Ethnicity
Polycystic ovary syndrome is neither population-specific nor restricted to any particular geographical region, its worldwide frequency is very high, affecting 5-10% of women of reproductive age. Eggers et al. [80] attempted to provide an evolutionary explanation for the high frequency of PCOS. According to this hypothesis, PCOS women may have reproductive advantage via kin selection because it seems plausible that childless women try to help to bring up the offspring of near relatives. This behaviour may increase their inclusive fitness and thus the high prevalence rates of PCOS may be the result of evolutionary mechanisms such as kin selection. However, other evolutionary processes associated with PCOS still have to be scrutinized.
Studies highlighting the impact of ethnicity on the presentation of PCOS basically have taken into consideration the metabolic aspects of the syndrome, which include IR, glucose intolerance, lipid abnormalities and coronary artery diseases. Williamson etal. [81] conducted a cross-sectional study of women of European, Maori, Pacific Island, Indian and Chinese origin for clinically and ultrasonically diagnosed PCOS. According to this study, European and Maori women were more likely to present with hirsutism than other ethnic groups, whereas Maori and Pacific Island women were more obese and had the highest rates of IR and lipid abnormalities. Other comparative investigations have revealed that Indian PCOS subjects had higher insulin responses compared to the cases with white ethnic background. The ethnic difference was less pronounced in obese women. [82] In addition, PCOS is reported to be more prevalent in South Asian women residing in the UK than the native Caucasians. [83]
Hyperhomocysteinaemia is a recognized risk factor for atherosclerosis, particularly among migrant South Asians, and has recently been shown to be correlated positively with the degree of IR/hyperinsulinaemia. Subsequently, another study by Wijeyaratne et al. [84] showed that elevation of fasting plasma homocysteine in PCOS varies with ethnicity and correlates significantly with fasting insulin. High homocysteine in young Sri Lankans with PCOS has major implications for their long-term risk for atherosclerosis. The incidence of IR is higher in Mexican American women with PCOS than in native white women. [85] While Japanese PCOS subjects might have insulin resistance but the factor of obesity has a stronger effect on insulin resistance than the existence of PCOS. [86] A general outcome of the above-mentioned studies demonstrates that the ethnic background of subjects with PCOS needs to be considered in studies on the metabolic parameters. In particular, the normative values for IR screening in the PCOS population should be individualized for different racial or ethnic populations. [85]
Indian Scenario
Population structure
Population substructure and recent admixture may confound the results of genetic association studies in unrelated individuals, leading to a potential excess of both false positive and false negative results. The possibility of false associations depends on the sampled population, the trait being studied and the marker being tested. [87] Ongoing modernization in India has elevated the prevalence of many complex genetic diseases associated with a Western lifestyle and diet. During the last few decades, the prevalence in India of complex genetic diseases associated with increased life span and with urban and Western lifestyles, including coronary artery disease, non-insulin-dependent diabetes and metabolic syndrome, has risen considerably and is now greater than in most other populations. Although Indian populations constitute more than one-sixth of the world′s human population, they have not generally been incorporated into the largest genomic surveys and thus, a genome-wide catalogue of genetic variation important to the design of association studies does not yet exist for India. [88]
Studies in India
In the Indian context, majority of the PCOS studies have been confined to the clinical dimensions. Apart from one genetic association study, no family studies regarding PCOS have been reported so far. Maitra et al. [89] conducted mutational analysis of CYP11A1 and Leptin as genetic determinants of hyperandrogenicity and obesity in PCOS patients, although the study did not indicate any variations in the exons of the aforesaid genes with regard to the syndrome. The same group exhibited a trend towards dyslipidaemia among women with PCOS, particularly in parameters associated with cardiovascular risk. [90] A significant association of obesity rather than raised testosterone with this dyslipidaemia was also confirmed by this study. In addition to this, Kalra et al. [91] concluded that IR is associated with dyslipidaemia in women with PCOS, independent of obesity. Incidence of type-2 diabetes is quite high in India and this metabolic feature was taken into account by Zargar et al. , [92] where a higher prevalence of polycystic ovaries was found in women with T2DM as compared to non-diabetic subjects. Asian Indians are insulin-resistant and prone to metabolic syndrome at an earlier age. South Indian women with the reproductive abnormalities of PCOS have greater IR and intimal median thickness (IMT), and therefore they must be advised about lowering the risk of future vascular disease. [93] IR is central to the pathogenesis of PCOS, while type-2 diabetes is commoner in South Asians. [83] The prevalence of polycystic ovaries in Indian women is very high and it has significant clinical associations.
End Note
Polycystic ovary syndrome is a highly prevalent endocrine disorder affecting approximately 7% of women of reproductive age. Patients with PCOS have several interrelated characteristics including hyperandrogenism, altered gonadotropin dynamics, chronic anovulation, polycystic ovaries and IR. The syndrome has a significant reproductive and metabolic impact, and is associated with increased risk of type-2 diabetes, dyslipidaemia, cardiovascular disease (CVD) and endometrial carcinoma. Development of PCOS may require the interaction of multiple genetic and environmental factors. The metabolic syndrome is evident at an early age in women with PCOS, irrespective of race and ethnicity. Hyperinsulinaemia, a central factor in the pathogenesis of PCOS, also appears to be a critical link between PCOS and the metabolic syndrome. In the absence of a concrete molecular genetic explanation for susceptibility, perhaps the most convincing evidence in favour of a particular variant or gene contributing to a complex disease is in the replicability of its association with the condition in different backgrounds. However, with regard to PCOS, such findings have yet not been obtained. Since most of the positive association studies are case-control studies based on large sample sizes, emphasis of future studies should be on the study design and the sample size. Apart from the conventional candidate gene approaches, the genome-wide scans might be promising. Further, employing cDNA technology, which would shed light on the functional aspect of the candidate genes, and epigenetic dimensions to the studies may help in attaining better understanding of the molecular genetic etiology of PCOS.
Considering the unique Indian population structure with strictly defined endogamous and genetically homogenous populations, it is imperative that more studies of molecular genetic nature should be undertaken in order to elucidate the pathogenicity and effect of ethnicity on the manifestation of this syndrome paving way for suitable medical intervention.
References
| 1. | Diao F, Xu M, Hu Y. The molecular characteristics of polycystic ovary syndrome (PCOS) ovary defined by human ovary cDNA microarray. J Mol Endocrinol 2004;33:59-72. Back to cited text no. 1 |
| 2. | Unluturk U, Harmanci A, Kocaefe C, Yildiz BO. The genetic basis of the polycystic ovary syndrome: A literature review including discussion of PPAR -γ. PPAR Res 2007;2004:49109. Back to cited text no. 2 |
| 3. | The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004;81:19-25. Back to cited text no. 3 |
| 4. | Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Futterweit W, et al . POSITION STATEMENT: Criteria for Defining Polycystic Ovary Syndrome as a predominantly hyperandrogenic syndrome: An androgen excess society guideline. J Clin Endocrinol Metab 2006;91:4237-45. Back to cited text no. 4 |
| 5. | Codner E, Escobar-Morreale HF. Clinical review: Hyperandrogenism and polycystic ovary syndrome in women with type-1 diabetes mellitus. J Clin Endocrinol Metab 2007;92:1209-16. Back to cited text no. 5 |
| 6. | Legro RS. Polycystic ovary syndrome and cardiovascular disease: A premature association? Endocr Rev 2003;24:302-12. Back to cited text no. 6 |
| 7. | Knochenhauer ES, Key TJ, Kahsar-Miller M. Prevalence of the polycystic ovary syndrome in unselected black and white women of the Southeastern United States: A prospective study. J Clin Endocrinol Metab 1998;83:3078-82. Back to cited text no. 7 |
| 8. | Michelmore KF, Balen AH, Dunger DB, Vessey MP. Polycystic ovaries and associated clinical and biochemical features in young women. Clin Endocrinol 1999;51:779-86. Back to cited text no. 8 |
| 9. | Vutyavanich T, Khaniyao V, Wongtra-Ngan S. Clinical,endocrine and ultrasonographic features of polycystic ovary syndrome in Thai women. J Obstet Gynecol Res 2007;33:677-80. Back to cited text no. 9 |
| 10. | Homburg R. What is polycystic ovary syndrome? Hum Reprod 2002;17: 2495-9. Back to cited text no. 10 |
| 11. | Azziz R, Woods KS, Reyna R. The prevalence and features of the polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab 2004;89:2745-9. Back to cited text no. 11 |
| 12. | Asunción M, Calvo RM, San Millan JL, Sancho J, Avila S, Escobar-Morreale HF. A prospective study of the prevalence of the polycystic ovary syndrome in unselected Caucasian women in Spain. J Clin Endocrinol Metab 2000;85:2434-8. Back to cited text no. 12 |
| 13. | Diamanti-Kandarakis E, Kouli CR, Bergiele AT, Filandra FA, TsianateliTC, Spina GC, et al . A survey of the polycystic ovary syndrome in the Greek island of Lesbos: Hormonal and metabolic profile. J Clin Endocrinol Metab 1999;84:4006-11. Back to cited text no. 13 |
| 14. | Botsis D, Kassanos D, Pyrgiotis E, Zourlas PA. Sonographic incidence of polycystic ovaries in a gynecological population. Ultrasound Obstet Gynecol 1995;6:182-5. Back to cited text no. 14 |
| 15. | Farquhar CM, Birdsall M, Manning P, Mitchell JM, France JT. The prevalence of polycystic ovaries on ultrasound scanning in a population of randomly selected women. Aust NZJ Obstet Gynaecol 1994;34:67-72. Back to cited text no. 15 |
| 16. | Cresswell JL, Barker DJ, Osmond C. Fetal growth, length of gestation and polycystic ovaries in adult life. Lancet 1997;350:1131-5. Back to cited text no. 16 |
| 17. | Clayton RN, Ogden V, Hodgkinson J, Worswick L, Rodin DA, Dyer S, et al . How common are polycystic ovaries in normal women and what is their significance for the fertility of the population? Clin Endocrinol 1992;37:127-34. Back to cited text no. 17 |
| 18. | Polson DW, Adams J, Wadsworth J, Franks S. Polycystic ovaries: A common finding in normal women. Lancet 1988;1:870-2. Back to cited text no. 18 |
| 19. | Ehrmann DA. Polycystic ovary syndrome. N Engl J Med 2005;352:1223-36. Back to cited text no. 19 |
| 20. | Dunaif A, Graf M, Mandeli J, Laumas V, Dobrjansky A. Characterisation of groups of hyperandrogenic women with acanthosis nigricans, impaired glucose tolerance, and/or hyperinsulinemia. J Clin Endocrinol Metab 1987;65:499-507. Back to cited text no. 20 |
| 21. | Norman RJ, Hagne WM, Masters SC, Wang XJ. Subjects with polycystic ovaries without hyperandrogenism exhibit similar disturbances in insulin and lipid profiles as those with polycystic ovary syndrome. Hum Reprod 1995;10:2258-61. Back to cited text no. 21 |
| 22. | Willis D, Mason H, Gilling-Smith C, Franks S. Modulation by insulin of follicle-stimulation hormone and leuteinizing hormone actions in human granulosa cells of normal and polycystic ovaries. J Clin Endocrinol Metab 1996;81:302-9. Back to cited text no. 22 |
| 23. | Nestler JE. Insulin regulation of human ovarian androgens. Hum Reprod 1997;12:53-62. Back to cited text no. 23 |
| 24. | Gambineri A, Pelusi C, Vicennati V, Pagotto U, Pasquali R. Obesity and the polycystic ovary syndrome. Int J Obestet 2002;26:883-96. Back to cited text no. 24 |
| 25. | Diamanti-Kandarakis E, Piperi C, Spina J. Polycystic ovary syndrome: The influence of environmental and genetic factors. Hormones 2006;5:17-34. Back to cited text no. 25 |
| 26. | Loucks TL, Talbott EO, Kathleen PM, Keelan M, Berga SL, GuzickDS. Do polycystic-appearing ovaries affect the risk of cardiovascular disease among women with PCOS. Fertil Steril 2000;74:547-52. Back to cited text no. 26 |
| 27. | Balen A. Polycystic ovary syndrome and cancer. Hum Reprod Update 2001;7:522-5. Back to cited text no. 27 |
| 28. | Hardiman P, Pillay OC, Atiomo W. Polycystic ovary syndrome and endometrial carcinoma. Lancet 2003;361:1810-2. Back to cited text no. 28 |
| 29. | Wild RA. Long term health consequences of PCOS. Hum Reprod Update 2002;8:231-41. Back to cited text no. 29 |
| 30. | Legro RS, Driscoll D, Strauss JF 3rd, Fox J, Dunaif A. Evidence for a genetic basis for hyperandrogenemia in polycystic ovary syndrome. Proc Natl Acad Sc USA 1998;95:14956-60. Back to cited text no. 30 |
| 31. | Legro RS, Strauss JF. Molecular progress in infertility: polycystic ovary syndrome. Fertil Steril 2002;78:569-76. Back to cited text no. 31 |
| 32. | Franks S, McCarthy M. Genetics of ovarian disorders: polycystic ovary syndrome. Rev Endo Metab Disord 2004;5:69-76. Back to cited text no. 32 |
| 33. | Franks S, Gharani N, McCarthy M. Candidate genes in polycystic ovary syndrome. Hum Reprod Update 2001;7:405-10. Back to cited text no. 33 |
| 34. | Menke MN, Strauss JF. Genetic approaches to polycystic ovarian syndrome. Curr Opin Obstet Gynecol 2007;19:355-9. Back to cited text no. 34 |
| 35. | Kahsar-Miller M, Azziz R. The development of the polycystic ovary syndrome: Family history as a risk factor. Trends Endo Metab 1998;9:55-8. Back to cited text no. 35 |
| 36. | Gharani N, Waterworth DM, Batty S. Association of the steroid synthesis gene CYP11a with polycystic ovary syndrome and hyperandrogenism. Hum Mol Genet 1997;6:397-402. Back to cited text no. 36 |
| 37. | Witchel SF, Kahsar-Miller M, Aston CE, White C, Azziz R. Prevalence of CYP21 mutations and IRS1 variant among women with polycystic ovary syndrome and adrenal androgen excess. Fertil Steril 2005;83:371-5. Back to cited text no. 37 |
| 38. | Wickenheisser JK, Nelson-DeGrave VL, McAllister JM. Dysregulation of cytochrome P450 17α-hydroxylase messenger ribonucleic acid stability in theca cells isolated from women with polycystic ovary syndrome. J Clin Endocrinol Metab 2005;90:1720-7. Back to cited text no. 38 |
| 39. | Carey AH, Waterworth D, Patel K. Polycystic ovaries and premature male pattern baldness are associated with one allele of the steroid metabolism gene CYP17. Hum Mol Genet 1994;3:1873-6. Back to cited text no. 39 |
| 40. | Urbanek M, Legro RS, Driscoll DA. Thirty-seven candidate genes for polycystic ovary syndrome: Strongest evidence for linkage is with follistatin. Proc Natl Acad Sc USA 1999;96:8573-8. Back to cited text no. 40 |
| 41. | Mifsud A, Ramirez S, Yong EL. Androgen receptor gene CAG trinucleotide repeats in anovulatoty infertility and polycystic ovaries. J Clin Endocrinol Metab 2000;83:3484-8. Back to cited text no. 41 |
| 42. | Hickey T, Chandy A, Norman RJ. The androgen receptor CAG repeat polymorphism and X-chromosome inactivation in Australian Caucasian women with infertility related to polycystic ovary syndrome. J Clin Endocrinol Metab 2002;87:161-5. Back to cited text no. 42 |
| 43. | Jaaskelainen J, Korhonen S, Voutilainen R, Hippelainen M, Heinonen S. Androgen receptor gene CAG length polymorphism in women with polycystic ovary syndrome. Fertil Steril 2005;83:1724-8. Back to cited text no. 43 |
| 44. | Shah NA, Antoine HJ, Pall M, Taylor KD, Azziz R, Goodarzi MO. Association of androgen receptor CAG repeat polymorphism and PCOS. J Clin Endocrinol Metab 2008 [Epub ahead of print]. Back to cited text no. 44 |
| 45. | Rajkhowa M, Talbot JA, Jones PW. Prevalence of an immunological LH β-subunit variant in a UK population of healthy women and women with polycystic ovary syndrome. Clin Endocrinol 1995;43:297-303. Back to cited text no. 45 |
| 46. | Tapanainen JS, Koivunen R, Fauser BC. A new contributing factor to polycystic ovary syndrome: The genetic variant of luteinizing hormone. J Clin Endocrinol Metab 1999;84:1711-5. Back to cited text no. 46 |
| 47. | Takahashi K, Karino K, Kanasaki H. Influence of missense mutation and silent mutation of LHβ-subunit gene in Japanese patients with ovulatory disorders. Eur J Hum Genet 2003;11:402-8. Back to cited text no. 47 |
| 48. | Urbanek M, Wu X, Vickery KR. Allelic variants of the follistatin gene in polycystic ovary syndrome. J Clin Endocrinol Metab 2000;85:4455-61. Back to cited text no. 48 |
| 49. | Liao WX, Roy AC, Ng SC. Preliminary investigation of follistatin gene mutations in women with polycystic ovary syndrome. Mol Hum Reprod 2000;6:587-90. Back to cited text no. 49 |
| 50. | Calvo RM, Villuendas G, Sancho J, San Millan JL, Escobar-MorrealeHF. Role of the follistatin gene in women with polycystic ovary syndrome. Fertil Steril 2001;75:1020-3. Back to cited text no. 50 |
| 51. | Waterworth DM, Bennett ST, Gharani N. Linkage and association of insulin gene VNTR regulatory polymorphism with polycystic ovary syndrome. Lancet 1997;349:986-90. Back to cited text no. 51 |
| 52. | Eaves IA, Bennett ST, Forster P. Transmission ratio distortion at the INS-IGF2 VNTR. Nat Genet 1999;22:324-5. Back to cited text no. 52 |
| 53. | Michelmore K, Ong K, Mason S. Clinical features in women with polycystic ovaries: Relationships to insulin sensitivity, insulin gene VNTR and birth weight. Clin Endocrinol 2001;55:439-46. Back to cited text no. 53 |
| 54. | Calvo RM, Teller?a D, Sancho J, San Millan JL, Escobar-Morreale HF. Insulin gene variable number of tandem repeats regulatory polymorphism is not associated with hyperandrogenism in Spanish women. Fertil Steril 2002;77:666-8. Back to cited text no. 54 |
| 55. | Powell BL, Haddad L, Bennett A. Analysis of multiple data sets reveals no association between the insulin gene variable number tandem repeat element and polycystic ovary syndrome or related traits. J Clin Endocrinol Metab 2005;90:2988-93. Back to cited text no. 55 |
| 56. | Tucci S, Futterweit W, Concepcion ES. Evidence for association of polycystic ovary syndrome in caucasian women with a marker at the insulin receptor gene locus. J Clin Endocrinol Metab 2001;86:446-9. Back to cited text no. 56 |
| 57. | Villuendas G, Escobar-Morreale HF, Tosi F, Sancho J, Moghetti P, SanMillan JL. Association between the D19S884 marker at the insulin receptor gene locus and polycystic ovary syndrome. Fertil Steril 2003;79:219-20. Back to cited text no. 57 |
| 58. | Urbanek M, Woodroffe A, Ewens KG. Candidate gene region for polycystic ovary syndrome on chromosome 19p13.2. J Clin Endocrinol Metab 2005;90:6623-9. Back to cited text no. 58 |
| 59. | El Mkadem SA, Lautier C, Macari F. Role of allelic variants Gly972Arg of IRS-1 and Gly1057Asp of IRS-2 in moderate-to severe insulin resistance of women with polycystic ovary syndrome. Diabetes 2001;50:2164-8. Back to cited text no. 59 |
| 60. | Villuendas G, Botella-Carretero JI, Roldan B. Polymorphisms in the insulin receptor substrate-1 (IRS-1) gene and the insulin receptor substrate-2 (IRS-2) gene influence glucose homeostasis and body mass index in women with polycystic ovary syndrome and non-hyperandrogenic controls. Hum Reprod 2005;20:3184-91. Back to cited text no. 60 |
| 61. | Dilek S, Ertunc D, Tok EC, Erdal EM, Aktas A. Association of Gly972Arg variant of insulin receptor substrate- 1 with metabolic features in women with polycystic ovary syndrome. Fertil Steril 2005;84:407-12. Back to cited text no. 61 |
| 62. | Ehrmann DA, Schwarz PEH, Hara M. Relationship of calpain-10 genotype to phenotypic features of polycystic ovary syndrome. JClinEndocrinol Metab 2002;87:1669-73. Back to cited text no. 62 |
| 63. | Gonzalez A, Abril E, Roca A. Comment: CAPN10 alleles are associated with polycystic ovary syndrome. J Clin Endocrinol Metab 2002;87:3971-6. Back to cited text no. 63 |
| 64. | Gonzalez A, Abril E, Roca A. Specific CAPN10 gene haplotypes influence the clinical profile of polycystic ovary patients. J Clin Endocrinol Metab 2003;88:5529-36. Back to cited text no. 64 |
| 65. | Haddad L, Evans JC, Gharani N. Variation within the type 2 diabetes susceptibility gene calpain-10 and polycystic ovary syndrome. J Clin Endocrinol Metab 2002;87:2606-10. Back to cited text no. 65 |
| 66. | Escobar-Morreale HF, Peral B, Villuendas G, Calvo RM, Sancho J, San Millan JL. Common single nucleotide polymorphisms in intron 3 of the calpain-10 gene influence hirsutism. Fertil Steril 2002;77:581-7. Back to cited text no. 66 |
| 67. | San Millan JL, Corton M, Villuendas G, Sancho J, Peral B, Escobar-Morreale HF. Association of the polycystic ovary syndrome with genomic variants related to insulin resistance, type 2 diabetes mellitus, and obesity. J Clin Endocrinol Metab 2004;89:2640-6. Back to cited text no. 67 |
| 68. | Panidis D, Kourtis A, Kukuvitis A. Association of the T45G polymorphism in exon 2 of the adiponectin gene with polycystic ovary syndrome: Role of ?4- androstenedione. Hum Reprod 2004;19:1728-33. Back to cited text no. 68 |
| 69. | Escobar-Morreale HF, Calvo RM, Sancho J, San Millan JL. TNF-α and hyperandrogenism: A clinical, biochemical, and molecular genetic study. J Clin Endocrinol Metab 2001;86:3761-7. Back to cited text no. 69 |
| 70. | Peral B, San Millan JL, Castello R. Comment: the methionine 196 arginine polymorphism in exon 6 of the TNF receptor 2 gene (TNFRSF1B) is associated with the polycystic ovary syndrome and hyperandrogenism. J Clin Endocrinol Metab 2002;87:3977-83. Back to cited text no. 70 |
| 71. | Villuendas G, San Millan JL, Sancho J, Escobar-Morreale HF. The-597 G ® A and -174 G ® C polymorphisms in the promoter of the IL-6 gene are associated with hyperandrogenism. J Clin Endocrinol Metab 2002;87:1134-41. Back to cited text no. 71 |
| 72. | Escobar-Morreale HF, Calvo RM, Villuendas G. Association of polymorphisms in the interleukin 6 receptor complex with obesity and hyperandrogenism. Obestet Res 2003;11:987-96. Back to cited text no. 72 |
| 73. | Hickey TE, Legro RS, Norman RJ. Epigenetic modification ofthe Xchromosome influences susceptibility to polycystic ovary syndrome. J Clin Endocrinol Metab 2006;91:2789-91. Back to cited text no. 73 |
| 74. | Wood JR, Dumesic DA, Abbott DH. Molecular abnormalities in oocytes from women with polycystic ovary syndrome revealed by microarray analysis. J Clin Endocrinol Metab 2007;92:705-13. Back to cited text no. 74 |
| 75. | Duskovα M, ?ermαkovα I, Hill M. What may be the markers of the male equivalent of polycystic ovary syndrome? Physiol Res 2004;53:287-95. Back to cited text no. 75 |
| 76. | Franks S, McCarthy MI, Hardy K. Development of polycystic ovary syndrome: Involvement of genetic and environmental factors. Int J Androl 2006;29:278-85. Back to cited text no. 76 |
| 77. | Abbott DH, Dumesic DA, Franks S. Developmental origin of polycystic ovary syndrome a hypothesis. J Endocrinol 2002;174:1-5. Back to cited text no. 77 |
| 78. | Nestler JE. Obesity, insulin, sex steroids and ovulation. Int J Obes Relat Metab Disord 2000;24:S71-3. Back to cited text no. 78 |
| 79. | Odunsi K, Kidd KK. A paradigm for finding genes for a complex human trait: Polycystic ovary syndrome and follistatin. Proc Natl Acad Sci USA 1999;96:8315-7. Back to cited text no. 79 |
| 80. | Eggers S, Hashimoto DM, Kirchengast S. An evolutionary approach to explain the high frequency of the polycystic ovary syndrome (PCOS). Anthropol Anz 2007;65:169-79. Back to cited text no. 80 |
| 81. | Williamson K, Gunn AJ, Johnson N, Milsom SR. The impact of ethnicity on the presentation of polycystic ovarian syndrome. Aust NZJ Obstet Gynaecol 2001;41:202-6. Back to cited text no. 81 |
| 82. | Norman RJ, Mahabeer S, Masters S. Ethnic differences in insulin and glucose response to glucose between white and Indian women with polycystic ovary syndrome. Fertil Steril 1995;63:58-62. Back to cited text no. 82 |
| 83. | Wijeyaratne CN, Balen AH, Barth JH, Belchetz PE. Clinical manifestations and insulin resistance (IR) in polycystic ovary syndrome (PCOS) among South Asians and Caucasians: Is there a difference? Clin Endocrinol 2002;57:343-50. Back to cited text no. 83 |
| 84. | Wijeyaratne CN, Nirantharakumar K, Balen AH, Barth JH, Sheriff R, Belchetz PE. Plasma homocysteine in polycystic ovary syndrome: Does it correlate with insulin resistance and ethnicity? Clin Endocrinol 2004;60:560-7. Back to cited text no. 84 |
| 85. | Kauffman RP, Baker VM, DiMarino P, Gimpel T, Castracane VD. Polycystic ovarian syndrome and insulin resistance in white and Mexican American women: A comparison of two distinct populations. Am J Obstet Gynecol 2002;187:1362-9. Back to cited text no. 85 |
| 86. | Kurioka H, Takahashi K, Miyazaki K. Glucose intolerance in Japanese patients with polycystic ovary syndrome. Arch Gynecol Obstet 2007;275:169-73. Back to cited text no. 86 |
| 87. | Ziv E, Burchard EG. Human population structure and genetic association studies. Pharmacogenomics 2003;4:431-41. Back to cited text no. 87 |
| 88. | Rosenberg NA. Low levels of genetic divergence across geographically and linguistically diverse populations from India. PLoS Genet 2006;2:2052-61. Back to cited text no. 88 |
| 89. | Maitra A, Pusalkar M, Gokral J, Meherji P. Mutational analysis of CYP11A1 and Leptin as genetic determinants of hyperandrogenicity and obesity in PCOS: Study in an Indian Cohort Group. Available from: http://www.ics-elsevier.com. International Congress Series 1271; 2004. p. 38-41. Back to cited text no. 89 |
| 90. | Maitra A, Pingle RR, Menon PS. Dyslipidemia with particular regard to apolipoprotein profile in association with polycystic ovary syndrome: A study among Indian women. Int J Fertil Womens Med 2001;46:271-7. Back to cited text no. 90 |
| 91. | Kalra A, Nair S, Rai L. Association of obesity and insulin resistance with dyslipidemia in Indian women with polycystic ovarian syndrome. Indian J Med Sci 2006;60:447-53. Back to cited text no. 91 |
| 92. | Zargar AH, Gupta VK, Wani AI. Prevalence of ultrasonography proved polycystic ovaries in North Indian women with type 2 diabetes mellitus. Reprod Biol Endocrinol 2005;3:35. Back to cited text no. 92 |
| 93. | Sundararaman PG, Manomani R, Sridhar GR, Sridhar V, SundaravalliA, Umachander M. Risk of atherosclerosis in women with polycystic ovary syndrome: A study from South India. Metab Syndr Relat Disord 2003;1:271-5. Back to cited text no. 93 |
Copyright 2008 - Journal of Postgraduate Medicine
The following images related to this document are available:
Photo images
[jp08043f2.jpg]
[jp08043f4.jpg]
[jp08043t4.jpg]
[jp08043t3.jpg]
[jp08043t1.jpg]
[jp08043t5.jpg]
[jp08043f3.jpg]
[jp08043f1.jpg]
[jp08043t2.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}