 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
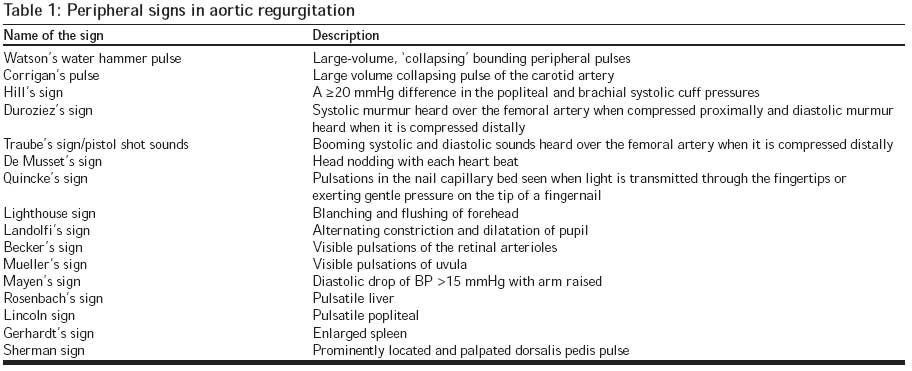
Journal of Postgraduate Medicine, Vol. 54, No. 2, April-June, 2008, pp. 163-165 Clinical Signs Watson's water hammer pulse Suvarna JC Department of Pediatrics, Seth GS Medical College and KEM Hospital, Parel, Mumbai - 400 012 Code Number: jp08056 Watson′s water hammer pulse (whp), also known as collapsing pulse, cannonball pulse or pulsus celer, is used to describe a pulse with a rapid upstroke and descent, characteristically described in aortic regurgitation. [1] Although the term Corrigan′s pulse has been used at times synonymously with whp, Corrigan′s pulse/sign is largely used to describe the abrupt distension and quick collapse of carotid pulse in aortic regurgitation whereas the term ′water hammer pulse′ is used for the characteristic pulse seen in peripheral arteries like the radial artery. It may be seen in a number of other conditions and with hyperdynamic circulation. [2] History Sir Dominic John Corrigan a British pathologist, in 1833 at a young age of 30, described the visible abrupt distension and collapse of the carotid arteries in patients with aortic insufficiency. However, the similarity of the palpable characteristics of the pulse in aortic insufficiency and that of a 19 th century Victorian ′water hammer toy′ was pointed out by Thomas Watson in the year 1844. Therefore the eponym, ′Watson pulse′ substituted ′Corrigan pulse′. [1] The ′water hammer toy′ is a hermetically sealed glass tube partly filled with water and exhausted of air. When reversed or shaken, the water being unimpeded by air strikes the sides or ends with the sound and impact of a hammer. [3] The characteristic collapsing carotid pulse seen in aortic regurgitation is still referred to as Corrigan′s sign. [1] Method to Elicit the ′Water Hammer Pulse′ Patient is made to recline. The examiner raises the patient′s arm vertically upwards and grasps the muscular part of the patient′s forearm with the entire hand (the flexor aspect of the patient′s forearm being covered with the examiner′s palm, principally the thenar eminence). The water hammer pulse is felt as an impact (tapping pulse) through the bulk of the forearm muscles with the thenar eminence of the palpating hand. [3]Causes Water hammer pulse indicates a low filling resistance in the blood vessels into which the left ventricle pumps the blood. This may be seen in physiological states (like exercise, heat, emotion, alcohol and pregnancy), hyperkinetic circulatory states (like anemia, thyrotoxicosis, Paget′s disease, cirrhosis of liver, beriberi, some cases of anoxic cor pulmonale and systolic hypertension with wide pulse pressure), a leak in the arterial side of the circulation (like in aortic regurgitation, patent ductus arteriosus, aorto-pulmonary window, rupture of sinus of Valsalva, leaking aortic valve prosthesis, ventricular septal defect with aortic regurgitation, truncus arteriosus, large ventricular septal defect and to a lesser degree in mitral regurgitation) and in complete heart block (a large volume of blood is pumped into a relatively empty reservoir with each systole). [3]Pathogenesis The abrupt jerky, forceful upstroke of the whp implies a rapid filling of the radial artery in systole due to an extra large amount of blood pushed by the distended left ventricle into relatively empty arterial vessels. The collapsing or sudden down stroke may be partly due to a sudden fall in the diastolic pressure in the aorta due to regurgitation of blood into the left ventricle through a leaky valve and partly due to the rapid emptying of the arterial system due to the marked increase in the velocity of the bloodstream. [3],[4] Apart from the pathogenetic factors which cause the widened pulse pressure, lifting the patient′s arm vertically upwards when eliciting the whp, helps the blood to empty quickly into the heart during diastole due to the gravity and also brings the radial artery more in line with the outflow stream of the aorta, thus accentuating the sign. [3],[5] It is interesting to note that while whp is a predominant feature in chronic aortic regurgitation (due to rheumatic etiology, collagen vascular disorders, Marfan′s syndrome, syphilis, bicuspid aortic valve or aortic root dilatation) it is not seen in acute aorticregurgitation (for example, that related to endocarditis, aortic dissection etc). This difference can be explained on the basis of the following mechanism: In chronic aortic regurgitation there is an increase in the left ventricular end-diastolic volume (due to the regurgitation). This leads to hemodynamic compensation in the form of chamber dilatation and eccentric hypertrophy; the latter being attained through replication of sarcomeres in series and elongation of the myocytes and myocardial fibers. [6] This results in an increase in the stroke volume and systolic pressure in the aorta. There is also an accompanying decrease in the diastolic pressure in the aorta resulting from diastolic aortic run-off into the left ventricle and decrease in the peripheral resistance due to peripheral vasodilatation. [7] The heart attempts to increase the stroke volume even further so as to compensate for thelow diastolic pressure in the aorta and thus try to maintain a normal mean arterial pressure. [7] This combination of raised systolic pressure and lowered diastolic pressure results in increased pulse pressure and therefore a water hammer pulse. [8] In contrast, in aortic regurgitation of short duration (acute aortic regurgitation) there is not enough time for the development of adequate compensatory mechanisms like eccentric left ventricular hypertrophy and dilatation. The left ventricle cannot respond to the diastolic volume overload with increase in the stroke volume and increase in the systolic pressure in the aorta. Theleft ventricular diastolic pressure increases suddenly due to the volume overload of the regurgitant blood. The elevated left ventricular diastolic pressure further restricts the volume of aortic reflux and therefore the aortic diastolic pressure may not be as low as that encountered in chronic aortic regurgitation. Hence, in acute aortic regurgitation, the pulse pressure may not be very wide and therefore, water hammer pulse may not ensue. [8] The early stage of hypertension, also described as high output hypertension, is associated with decreased peripheral vascular resistance and concomitant cardiac stimulation (due to adrenergic hyperactivity and altered calcium homeostasis). This causes whp. In contrast, the chronic phase of essential hypertension has normal or reduced cardiac output and elevated systemic vascular resistance and therefore no whp. In cirrhosis of liver, arterial vasodilatation and increase in cardiac output lead to a hyperdynamic circulation thus causing a whp. Approach to a Case with WHP Conditions like severe anemia, thyrotoxicosis, beriberi, fever, pregnancy, chronic alcoholism, Marfan′s syndrome, collagen vascular disorders, syphilis can be recognized by virtue of their extra-cardiac manifestations. A history of prior throat infection in an older child with accompanying features of carditis, arthritis, subcutaneous nodule, chorea or erythema marginatum would suggest a rheumatic etiology for the aortic regurgitation. History of recurrent respiratory tract infections from early infancy and characteristic examination findings could help in the diagnosis of congenital heart diseases like patent ductus arteriosus, aorto-pulmonary window, truncus arteriosus or ventricular septal defect with aortic regurgitation. A 2-D echo may be required to establish the diagnosis in these cases. Importance of ′water hammer pulse′ Similar Terminology: Blood Hammer Phenomenon The term, ′blood hammer phenomenon′ was first introduced in cerebral hemodynamics to describe a sudden increase of the upstream blood pressure in a blood vessel (especially an artery or arteriole) due to an abrupt vessel obstruction causing a block. It was described by analogy with the term water hammer in hydraulics (i.e. sudden and significant rise in pressure inside a pipe with flowing fluid when the flow is sharply interrupted). It should not be confused with whp. [9]References
Copyright 2008 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp08056t1.jpg] |
| |||||||||

{kind=link}