 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
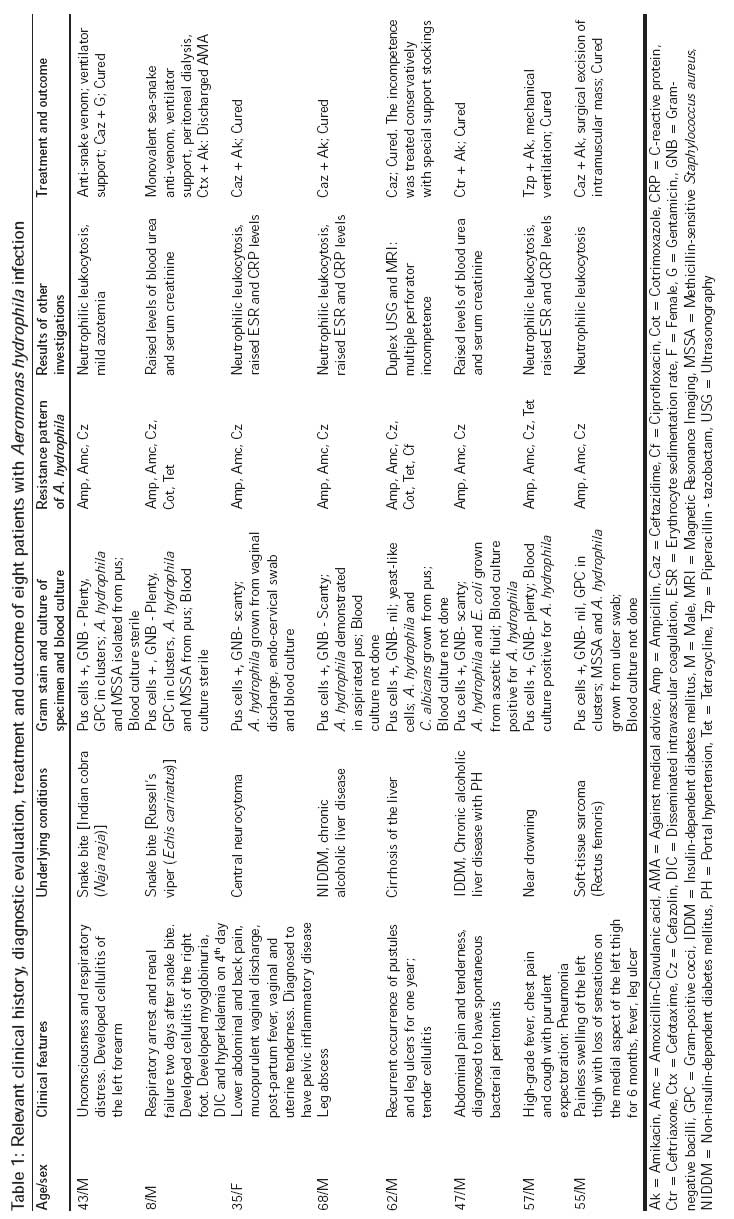
Journal of Postgraduate Medicine, Vol. 54, No. 3, July-September, 2008, pp. 199-202 Original Article Emerging extra-intestinal infections with Aeromonas hydrophila in coastal region of southern Karnataka Mukhopadhyay C, Chawla K, Sharma Y, Bairy I Department of Microbiology, Kasturba Medical College, Manipal - 576 104, Karnataka Code Number: jp08068 Abstract Background: Aeromonas species are gram-negative rods usually isolated from the gastrointestinal tract. They have been occasionally reported as a cause of extra-intestinal infections such as cellulitis, cholangitis, necrotizing fascitis, meningitis, bacteremia, or peritonitis in both immunocompetent and immunocompromised patients .Aim: To determine the role and possible pathogenesis of Aeromonas in extra-intestinal infections. Settings and Design: Retrospective analysis carried out at Kasturba Hospital Manipal, Karnataka in the months of January and February 2007. Materials and Methods: Clinical manifestations and management of eight cases of extra-intestinal infections caused by A. hydrophila , from the south Karnataka coastal region were reviewed. The isolates were identified with the help of biochemical tests using standard guidelines. Results: All patients acquired Aeromonas infections in the community. Five (62.5%) had underlying illnesses, such as liver disease, diabetes mellitus or malignancy. Five (62.5%) had polymicrobial infections, and three (37.5%) were complicated with bacteremia. These included three patients with ulcers or abscess over the lower leg, two with cellulitis due to snake bite and one each with pelvic inflammatory disease, spontaneous bacterial peritonitis and pneumonia. A. hydrophila was found to be a causative agent of pelvic inflammatory disease or cellulitis following sea snake bite, and such a clinical scenario has not been previously described. Seven patients survived the illness. Conclusions: Isolation of A. hydrophila from extra-intestinal specimens demands utmost clinical and microbiological vigilance in diagnosis, since the organism can cause serious infections among immunocompromised as well as immunocompetent individuals. Keywords: Aeromonas hydrophila , extra-intestinal infections, India The genus Aeromonas has become an increasingly troublesome group to physicians and microbiologists by virtue of its changing phylogenetic relationships, evolving taxonomy and controversial role in certain diseases. [1] These short gram-negative rods with rounded ends are facultative anaerobes. [2] Although discovered over 100 years ago, their role in the human bloodstream - or other sterile body sites - infection has been proven only in the last three decades. However, their role in human gastrointestinal infections is still speculative. As an ′emerging pathogen′, the major diseases caused by Aeromonas spp. can be classified into two major groups: septicemia (mainly by strains of A. veronii subspp. sobria and A. hydrophila ), and gastroenteritis (any mesophilic spp., but particularly A. hydrophila and A. veronii ). [3] Nowadays it has also been implicated as a cause of various extra-intestinal manifestations, like peritonitis, cholangitis, skin and soft tissue infections, septic arthritis, osteomyelitis, ocular infections, myositis, urinary tract infections, pneumonia, meningitis and hemolytic uremic syndrome. [4],[5] The infection is mainly acquired from two sources: environment-water-animals complex and ingestion of contaminated food. [6] Aeromonas has been reported as a contaminant (37%) from seafood samples from the west coastal region of southern India, where sea-water fish farming is a major occupation of the local inhabitants. [7] Drugs like tetracycline and cotrimoxazole are routinely included in the medicated feeds for the fish. This practice could be responsible for the occurrence of drug-resistant strains. [8] This communication describes eight cases with varied extra-intestinal manifestations, antibiotic sensitivity, therapeutic management and outcome. Materials and Methods In this retrospective study, the clinical features and management of eight cases of Aeromonas admitted to the hospital in the months of January and February 2007 were reviewed and analyzed. The source of infection was determined to be "community-acquired" if the infection was present at the time of admission or became evident within 48 h after admission. The patient was diagnosed to have a polymicrobial infection, if microorganisms other than Aeromonas spp. were also isolated in the same clinical specimen. The following procedure was implemented for isolation and identification of Aeromonas spp. and for determination of antimicrobial sensitivity: all clinical samples were transported within ½ h of collection. After gram staining, samples were cultured aerobically on MacConkey agar and blood agar, and anaerobically in some cases. Oxidase-positive, non-lactose fermenter colonies showing β-hemolysis on sheep blood agar were further identified using standard procedures. [9] The isolate was identified as A. hydrophila , if it showed positive aesculin hydrolysis, DNAse, Voges-Proskauer test, indole, lysine decarboxylase and arginine dehydrolase. It fermented glucose with acid and gas, and arabinose, mannitol, sucrose with acid only. Antibiotic susceptibility to the following antimicrobial agents was studied according to the criteria of the Clinical and Laboratory Standards Institute: ampicillin, amoxicillin -clavulanic acid, cefazolin, cefotaxime, gentamicin, tetracycline, ciprofloxacin and cotrimoxazole. [10] Results Eight patients (age range: 8-68 years; six adult males, one boy and one adult female) fishermen or women by occupation, were identified to have extra-intestinal infections caused by A. hydrophila . Salient points in presentation and treatment are summarized in [Table - 1]. The majority of infections were polymicrobial (62.5%) in nature with methicillin-sensitive Staphylococcus aureus (MSSA) or Escherichia coli as the commonly isolated accompanying organisms. Infections mostly involved the extremities and most patients (62.5%) had underlying illnesses, such as diabetes mellitus, liver disease or malignancy. Three patients suffered from bacteremia. Despite several subjects having serious predisposing conditions, some requiring life support systems or having infections resistant to anti-microbial agents, they showed response to therapy. Seven patients survived and one was lost to follow-up.Discussion The spectrum of extra-intestinal A. hydrophila infection in our series of patients ranged from superficial soft-tissue infections to deep-seated infections. Following the feces, wounds are the second common clinical specimens yielding Aeromonas . [1] Microbial virulence factors interact with host defenses in the pathogenesis of soft-tissue infections by two mechanisms. First, the bacterium invades through trauma and causes primary infection of soft tissue, which is followed by secondary sepsis. [11] Second, sepsis is first induced by the bacterium, followed by secondary metastatic lesions of the soft tissues. Healthy individuals become infected with Aeromonas subsequent to abrasion or penetrating injury (82%) that results in exposure to environmental sources (43% related to aquatic facilities, either recreational or occupational). [1],[12] Young men often suffer from trauma (67-90%) [4],[13],[14] and the lower extremities (60-65%) are the most common sites of infection, followed by the scalp, hands and arms. [12],[14] Penetrating injuries of soft-tissue with snake bite followed by infection only appear to have been reported thrice before, once in Thailand [15] and twice from Brazil, [16] but none of those cases was preceded by a sea-snake bite. Snakes have a local necrotizing, myotoxic, edema-inducing venom that would favor the multiplication of A. hydrophila strains in the injured tissues. It is possible that these organisms were present in the mouth, fangs or venom of the snakes. [16],[17] The use of tourniquet might have increased the intensity and probability of local tissue damage and increased the chances for the occurrence of soft-tissue infection. [17] However, in case of snake bites, local envenomation rather than trauma contributes to more severe injuries. [4],[18] Based on the previous case reports and our observations in the first case, the prognosis of soft-tissue infections by A. hydrophila complicating snake bite appears to be good. Sea snake bites are most often inconspicuous and in nearly 80% cases, they fail to produce significant envenomation. [18] However, sea-snake venom accounts for significant muscle necrosis with consequent myoglobinemia and hyperkalemia. We had three patients with localized A. hydrophila infection in legs, where there was no history of penetrating injury. The patients were suffering from non-insulin-dependent diabetes mellitus, cirrhosis and malignancy (sarcoma), which might have predisposed the respective individuals to the development of infection. [4],[19],[20] Bacterial peritonitis is a frequent complication in patients with cirrhosis of the liver and Aeromonas is a very infrequent causative agent. [21],[22],[23] In patients with liver cirrhosis, the presence of portal hypertension, reticulo-endothelial system dysfunction and bowel wall congestion and inflammation can lead to significant degeneration of intestinal mucosa. Under these circumstances, intestinal bacteria can easily invade the bloodstream and cause bacteremia. Hematogenous spread from the gastrointestinal tract is suggested to be a source of spontaneous bacterial peritonitis. [24] The association of A. hydrophila infection with various malignancies, such as malignant melanoma, pancreas cancer, hepatoma, and leukemia, has been described. [25] However, it needs to be seen whether occurrence of A. hydrophila infection in a woman with neurocytoma is a chance observation. Pelvic inflammatory disease and bacteremia caused by Aeromonas species is a unique clinical setting which has not yet been reported. Although the source of infection could not be traced, long-term chemotherapy for neurocytoma might have contributed to predisposition to Aeromonas infection. It is possible that the infection may, in fact, have been acquired during the process of child birth conducted at home. One of the cases developed A. hydrophila -related pneumonia after near-drowning in sea water. A. hydrophila is considered to be frequently associated with serious pneumonia in such situations, especially in hypoxia-induced lung damage due to pulmonary edema. [26],[27],[28] Circumstantial evidence suggests that patients reported in this series had community-acquired A. hydrophila infection. The organism has been isolated from chlorinated [29] as well as from fresh or brackish water [30] and from sea foods purchased from retail markets and supermarkets. [31] This series of cases occurring in individuals working as fishermen and fisherwomen could indicate possible contamination of seawater with the organism, which could be proved by checking samples of the seawater. Also, the ′emergence′ of extra-intestinal Aeromonas infections demands a thorough surveillance in the suspected population in the coastal region. The organisms were susceptible to third-generation cephalosporins and aminoglycosides in vitro, which were successfully used for the treatment of infections. However, an increase in the incidence of resistance to cephalosporins, aminoglycosides, tetracycline and cotrimoxazole is not uncommon nowadays. [1] We concede that a comprehensive phylogenetic analysis of the genus Aeromonas by 16s rRNA gene sequencing could be a better option for ensuring identification. [32],[33] Despite this limitation, our study has helped describe newer sites of A. hydrophila infection and has added to the variability of manifestations described in the literature. Acknowledgment We are grateful to our clinician colleagues, the patients and their relatives for their support and cooperation.References
Copyright 2008 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp08068t1.jpg] |
| |||||||||

{kind=link}