 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
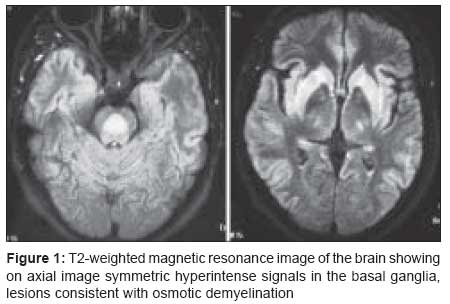
Journal of Postgraduate Medicine, Vol. 54, No. 3, July-September, 2008, pp. 243-244 Letter Catatonic stupor in a case of pontine and extrapontine myelinolysis: Clinical and radiological dissociation Ruiz Miyares FJ, Deleu D, Al Hail H, Mesraoua B Department of Neurology, Hamad Medical Hospital, Doha Code Number: jp08088 Sir, Neuropsychiatric manifestations of central pontine myelinolysis (CPM) and extrapontine myelinolysis (EPM) range from subtle variations in mood to bizarre behavior, hallucinations or catatonic stupor. [1] Extra-pyramidal features with delayed onset rigid-dystonia have also been reported, widening the spectrum of clinical manifestations. [2] We describe a case of CPM/ EPM with unusual psychiatric manifestation including compulsive eating and catatonic stupor. A 23-year-old Nepali man presented with confusion, compulsive eating and generalized catatonia. There was no past history of chronic alcohol abuse, exposure to neuroleptic drugs or toxic chemicals. Three weeks earlier he was discharged in good health after being admitted with mild disorientation and hyponatremia (127 mmol/L). At that time, all other biochemical parameters were normal. The ultrasound abdomen, CT brain, CSF analysis and electroencephalogram were also reported to be normal. The hyponatremia was corrected with normal saline (7 mmol/L in 24 h) and he was discharged after one week. Current neurological examination revealed a confused, stuporous and poorly communicative patient. He was excessively drooling and showed features of bulbar palsy. During passive movements the limb was kept in the same position for a prolonged period even when the position and posture seemed uncomfortable and bizarre. Serum biochemistry (sodium 136 mM/L) and CBC were normal, Serological tests for HIV and hepatitis was negative. Toxicology screening was also negative. The CSF analysis did not reveal any abnormality. The EEG showed mild generalized slowing of the background with no epileptiform discharges. Magnetic resonance imaging (MRI) of the brain revealed hyperintense signals in the pons and basal ganglia [Figure - 1]. Treatment with risperidone (6 mg per day) was initiated resulting in gradual improvement of symptoms. He was discharged three weeks later with manifest clinical recovery despite unremitting radiological abnormalities, expressed by the symmetyric hyperintense signals in the pons and basal ganglia in T2 weighted and FLAIR sequences. Emotional incontinence (pseudobulbar syndrome) is a rare neuropsychiatric manifestation of CPM/EPM. [1] Only one case of CPM with catatonia and behavioral deterioration has been reported. [3] Demyelination usually occurs during the initial assault of the osmotic demyelinating process, with clinical manifestations occurring commonly within one week of the initial correction of the hyponatremia. [4] However, there is extreme variability in its presentation, which is further characterized by the lack of clinicoradiological correlation. Differential diagnosis of bilateral symmetrical signal changes in the basal ganglia on MRI includes hypoxia, carbon monoxide poisoning, Wilson′s disease, Wernicke′s encephalopathy and Leigh′s disease [1] and these need to be excluded on clinical grounds and with the help of appropriate investigations. The persistence of abnormal, hyperintense signals in spite of significant clinical improvement confirms the heterogeneity of CPM/EPM. The clinical expressiveness of the lesions seems to be independent of the intensity of the signals in some cases. A careful follow-up is needed to assess the state of this patient on a long-term basis. References
Copyright 2008 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp08088f1.jpg] |
| |||||||||

{kind=link}