 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
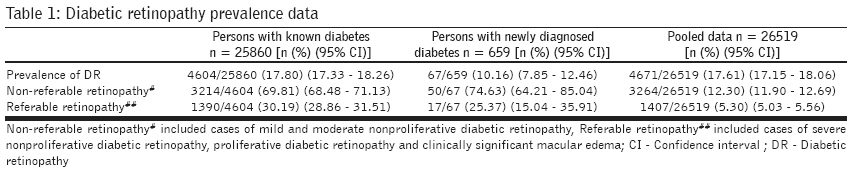
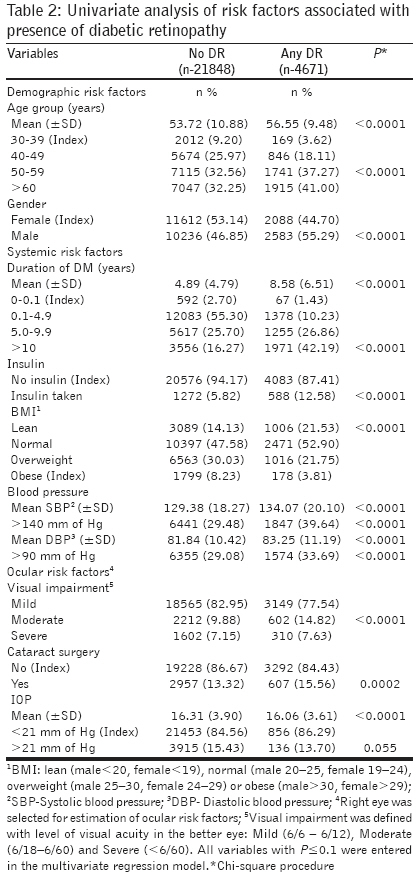
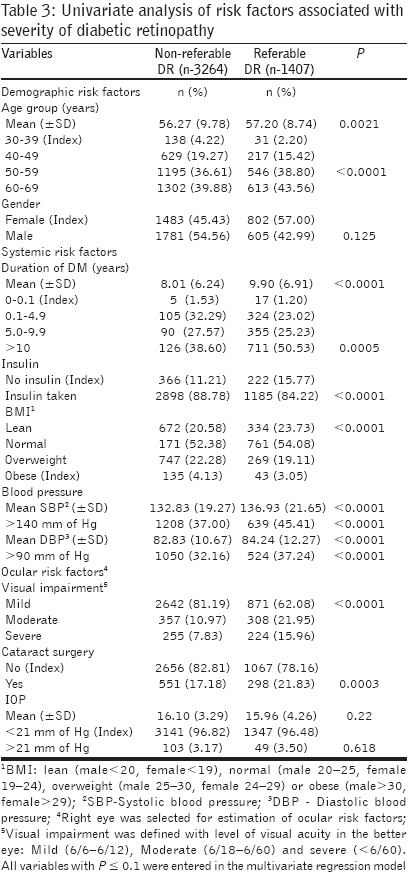
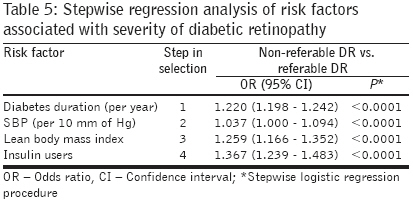
Journal of Postgraduate Medicine, Vol. 55, No. 2, April-June, 2009, pp. 92-96 Original Article Risk factors for diabetic retinopathy in self-reported rural population with diabetes Rani PK, Raman R, Chandrakantan A, Pal SS, Perumal GM, Sharma T Vision Research Foundation, Sankara Nethralaya Diabetic Retinopathy Project, 18, College Road, Sankara Nethralaya, Chennai - 600 006, Tamil Nadu Date of Submission: 15-Apr-2008 Code Number: jp09027 PMID: 19550052 Abstract Background: Diabetes and its related microvascular complications like diabetic retinopathy (DR) are showing increased prevalence in India. However, the magnitude of DR in rural population with diabetes needs exploration.Aim: To estimate the prevalence and risk factors for the presence and severity of diabetic retinopathy in the self-reported rural population with diabetes. Settings and Design: In a cross-sectional study, a total of 26,519 participants (age ≥ 30 years) attended 198 diabetic retinopathy screening camps conducted in three southern districts of Tamilnadu, India, between February 2004 and April 2006. Materials and Methods: All the participants underwent a dilated eye examination to detect DR by indirect ophthalmoscopy. Systemic and ocular risk factor estimation was done in a comprehensive examination. Statistical Analysis: Univariate and stepwise regression analyses were done to identify the independent risk factors associated with the presence and severity of retinopathy. Results: The prevalence of diabetic retinopathy was 17.6% among the self-reported rural population with diabetes. The prevalence of referable (sight threatening) retinopathy was 5.3%. Risk factors associated with the development of any DR were male gender (OR= 1.37), longer duration of diabetes (per year, OR= 1.07), lean body mass index (OR= 1.30), higher systolic blood pressure (per 10 mm Hg, OR= 1.18), and insulin treatment (OR= 1.34; P < 0.0001). Risk factors associated with referable retinopathy included longer duration of diabetes (per year, OR= 1.22), lean body mass index (OR= 1.25), higher systolic blood pressure (per 10 mm Hg, OR= 1.03), and insulin treatment (OR= 1.36; P < 0.0001). Conclusion: The study identified risk factors associated with DR in the rural population with diabetes. The results suggested that there was a need for formulating effective preventive strategies to minimize avoidable blindness due to diabetes, in rural areas. Keywords: Diabetic retinopathy, ocular risk factors, rural population, systemic risk factors Diabetic Retinopathy (DR), a microvascular complication, develops in nearly all persons with type 1 diabetes and in more than 77% of those with type 2 diabetes, who survive for over 20 years with the disease. [1] The burden of diabetes is reaching an alarming proportion in India. The World Health Organization (WHO) estimates an increase in population with diabetes: from 30 million in 2000 to 80 million in 2030. [1] WHO also estimates that DR is responsible for 4.8% of the 37 million cases of blindness throughout the world. [2] Earlier, diabetes mellitus (DM) was considered an urban disease. However, recent studies (population-based and self-reported) have shown an increasing prevalence in rural areas as well. [3],[4],[5] Ramachandran et al., [4] showed nearly a three-fold increase in the rural prevalence of diabetes to 6.3% in 2003 compared to 2.2% in 1989. In a cross-sectional study of a self-reported population attending diabetic retinopathy screening camps in 2006, in rural areas, we found the prevalence of diabetes as 20% and that of diabetic retinopathy as 18%. [5] Materials and Methods Between February 2004 and April 2006, 198 diabetic retinopathy screening camps were conducted in a cross-sectional study in three southern districts of Tamilnadu. The methodology of diabetic retinopathy screening camps is described in detail elsewhere. [6] Various measures (such as organizing awareness meetings in the community, focusing on diabetes and related complications; displaying education materials such as leaflets, banners or posters; and involving local diabetologists and volunteers from NGOs such as Lions club) were employed to maximize the effectiveness of these screening camps. The procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 2000. The Institutional Review Board approved the study. A target population with diabetes, aged 30 years and above, underwent a comprehensive dilated eye examination for the diagnosis of diabetic retinopathy. Procedures adopted for the diagnosis of diabetes mellitus and diabetic retinopathy, and data collection for risk assessments are described below. Diagnosis of diabetes mellitus Diagnosis of diabetic retinopathy Risk factor assessment Based on the BMI, individuals were classified as lean (male < 20, female < 19), normal (male 20 - 25, female 19 - 24), overweight (male 25 - 30, female 24 - 29) or obese (male > 30, female > 29). [9] Blood pressure was measured with a sphygmomanometer, with the patient in the sitting position. The ocular risk factors included details of first and last eye examinations, any visual complaint or history of laser or eye surgery. LogMAR charts were used to assess the visual acuity. Statistical analysis Results A total of 26,519 persons with diabetes participated in the 198 diabetic retinopathy screening camps. Estimation of prevalence of diabetic retinopathy Assessment of demographic, systemic, and ocular risk factors [Table - 4] and [Table - 5] present the results of stepwise forward and backward, logistic regression analyses. All variables that were significant in the univariate analyses were entered in a multivariate model. The risk factors independently associated with any diabetic retinopathy, [Table - 4] in order of importance, were, longer duration of diabetes, lean BMI, elevated systolic blood pressure, insulin intake, and male gender. Similarly, the risk factors independently associated with severity of diabetic retinopathy, [Table - 5] in order of importance, were, longer duration of diabetes, elevated systolic blood pressure, lean BMI, and insulin intake. Discussion The prevalence of diabetic retinopathy in a self-reported cohort of people with diabetes, in the rural population of India, was 17.6%. Even newly diagnosed individuals with diabetes (as defined in this study) showed evidence of ′any diabetic retinopathy′ - around 10% - , and one-fourth of them showed ′referable retinopathy′ (severe NPDR, PDR, and/or CSME). Logistic regression analysis revealed certain independent risk factors associated with both the presence and severity of diabetic retinopathy; they were, longer duration of diabetes, lean BMI, elevated systolic blood pressure, and insulin intake, in the present study of the rural population with diabetes. The duration of diabetes, however, remained the strongest predictor for any diabetic retinopathy and its severity. Moreover, such an association has been observed by several other investigators as well. [10],[11],[12],[13],[14],[15] The association showed a linear trend for any diabetic retinopathy and also for referable diabetic retinopathy. Increased duration influencing the occurrence of diabetic retinopathy and its severity was probably related to the magnitude or prolonged exposure, or both, to hyperglycemia coupled with other risk factors. While the duration of diabetes was an independent risk factor, 10% of the individuals with newly diagnosed diabetes did show diabetic retinopathy, suggesting that these patients would have been undiagnosed or undetected; in other words, the duration of diabetes and the exact duration of hyperglycemia did not go hand in hand. Male gender was observed to be associated with the presence of any DR (1.37 times), but not its severity. Similar observations were made by Pradeepa et al., in an urban Indian population and in the Los Angeles Latino Eye Study. [10],[11] The inverse relation between BMI and diabetic retinopathy was also observed in the Indian population-based studies and also by others. [13],[14],[15] This could be due to the catabolic effect of the lack of insulin over a long duration of hyperglycemia, resulting in lean individuals. There are evidences that South Asians have abdominal obesity despite normal body mass indices, the so called "Asian Indian phenotype"; which may explain this paradox. [16] Further, it is interesting to note that in Caucasians, high BMI is observed in subjects with diabetes, but in Asian population, subjects with diabetes are lean with low BMI. [17] This may be linked to the fact that Asians with type 2 diabetes mellitus show lesser insulin secretion, but greater insulin sensitivity, as compared to Caucasian diabetic patients. [18],[19] Every increase in systolic blood pressure by 10 mm of Hg showed a linear trend, around 1 - 1.2 times the risk of influencing the presence and severity of diabetic retinopathy. Such a correlation between systolic blood pressure and diabetic retinopathy was also noted by others. [11] The association noted with insulin therapy could be because patients with retinopathy are preferentially started on insulin by their physicians. Retinopathy was positively associated with moderate visual impairment (6/18 - 6/60). Similar risk association with moderate visual impairment was observed in our earlier study. [5] Retinopathy was positively associated with the history of cataract surgery. Cataract surgery as a risk factor for DR was also reported in the Los Angeles Latino Eye Study. [11] The limitation of the present study was the self-reported diabetic population and so the possibility of a selection bias. Identified risk factors were based on just point estimation; therefore, a causal relationship with diabetic retinopathy could not be proved. Nevertheless, some of the factors like systolic blood pressure could be modulated, thereby reducing the risk of preventable blindness in susceptible populations. Another limitation of the present study was DR grading that was based on indirect ophthalmoscopy and not on fundus photography grading. This could have resulted in the underestimation of the prevalence of DR. There is a paucity of published data regarding DR prevalence as well as risk factor estimates of the rural population with diabetes. The present study gives us an important measure of the DR burden and associated risk factors in a large sample size of over 25000 individuals with diabetes, in rural settings. Therefore, there is an urgent need to formulate effective screening strategies for the early detection of diabetes and diabetic retinopathy. This would minimize the occurrence of avoidable blindness in developing nations such as India. Acknowledgments We acknowledge the support of the Lions Clubs International Foundation (LCIF) and RD Tata Trust, Mumbai, for providing grants to support this project.References
Copyright 2009 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp09027t5.jpg] [jp09027t2.jpg] [jp09027t4.jpg] [jp09027t1.jpg] [jp09027t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}