 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 55, No. 2, April-June, 2009, pp. 97-103 Original Article Quality of life of parents of children with newly diagnosed specific learning disability Karande S, Kulkarni S Learning Disability Clinic, Department of Pediatrics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai 400 022 Date of Submission: 16-Jan-2009 Code Number: jp09028 PMID: 19550053 Abstract Background: Poor school performance in children causes significant stress to parents.Aims: To analyze the quality of life (QOL) of parents having a child with newly diagnosed specific learning disability (SpLD) and to evaluate the impact of clinical and socio-demographic characteristics on their QOL. Design: Cross-sectional questionnaire-based study. Setting: Learning disability clinic in tertiary care hospital. Materials and Methods: From June 2006 to February 2007, 150 parents (either mother or father) of children consecutively diagnosed as having SpLD were enrolled. Parent's QOL was measured by the WHOQOL-100 instrument which is a generic instrument containing 25 facets of QOL organized in six domains. Statistical Analysis Used: Independent samples t-test, one-way analysis of variance, and multiple regression analysis were carried out for statistical significance. Results: Mean age of parents was 42.6 years (SD 5.5); mothers to fathers ratio 1.3:1; and 19 (12.7%) were currently ill. Only four WHOQOL-100 domains (psychological > social relationships > environment > spiritual) and five WHOQOL-100 facets (leisur > pfeel > energy > esteem > sex) contributed significantly to their "overall" QOL. Female gender, being currently ill, being in paid work, and having a male child were characteristics that independently predicted a poor domain/facet QOL score. Conclusions: The present study has identified domains and facets that need to be addressed by counselors for improving overall QOL of these parents. Initiating these measures would also improve the home environment and help in the rehabilitation of children with SpLD. Keywords: Dyslexia, educational status, health status, mothers, quality of life Specific learning disability (SpLD) is a group of neurodevelopmental disorders which manifest in childhood as persistent difficulties in learning to efficiently read (dyslexia), write (dysgraphia), or do simple mathematical calculations (dyscalculia) despite normal intelligence, conventional schooling, intact hearing and vision, and adequate motivation and socio-cultural opportunity. [1],[2] Up to 5-15% of "seemingly normal" school children have this invisible handicap. [1],[2] These children fail to achieve school grades commensurate with their intellectual potential. [1],[2] Up to 20-25% of children with SpLD have associated attention-deficit/hyperactivity disorder (ADHD) which is characterized by persistent hyperactivity, impulsivity, and inattention; and this co-morbidity further impairs their learning. [1],[2] In our country, due to a generalized lack of awareness, SpLD often remains undetected resulting in the afflicted child experiencing chronic poor school performance and class detainment. [2],[3] Poor school performance not only results in the child having a low self-esteem, but also causes significant stress to the parents. [3] Quality of life (QOL) is defined by the World Health Organization (WHO) as an individual′s perception of his/her position in life in the context of the culture and value systems in which he/she lives, and in relation to his/her goals, expectations, standards, and concerns. [4] It is a broad-ranging concept, incorporating in a complex way, the person′s physical health, psychological state, level of independence, social relationships, personal beliefs, and relationship to salient features of the environment. [4] A detailed Medline search using the key words "quality of life" and "parents" and "dyslexia" failed to retrieve any study which has analyzed the QOL of parents having a child with SpLD. Keeping this in mind we conducted the present study whose objectives were to measure and analyze the QOL of parents having a child with newly diagnosed SpLD and to evaluate the impact of clinical and socio-demographic characteristics on their QOL. Materials and Methods Diagnosis of SpLD Curriculum-based assessment is a recommended method of diagnosing SpLD. [1],[2],[8] Employing a locally developed curriculum-based test, the special educator conducted the educational assessment in specific areas of learning, namely, basic learning skills, reading comprehension, oral expression, listening comprehension, written expression, mathematical calculation, and mathematical reasoning. [1],[2] An academic achievement of two years below the child′s actual school grade placement or chronological age was considered diagnostic of SpLD. [1],[2] This test is a criterion-referenced test based on the Maharashtra education board curriculum followed in Mumbai schools. [2] The diagnosis of co-occurring ADHD was made by the pediatrician and also confirmed by the psychiatrist. For diagnosing ADHD the standard recommended method was followed, namely, by ascertaining that the child′s specific behaviors met the diagnostic and statistical manual of mental disorders-IV-revised (DSM-IV-R) criteria. [9] Sample size and parent enrolment
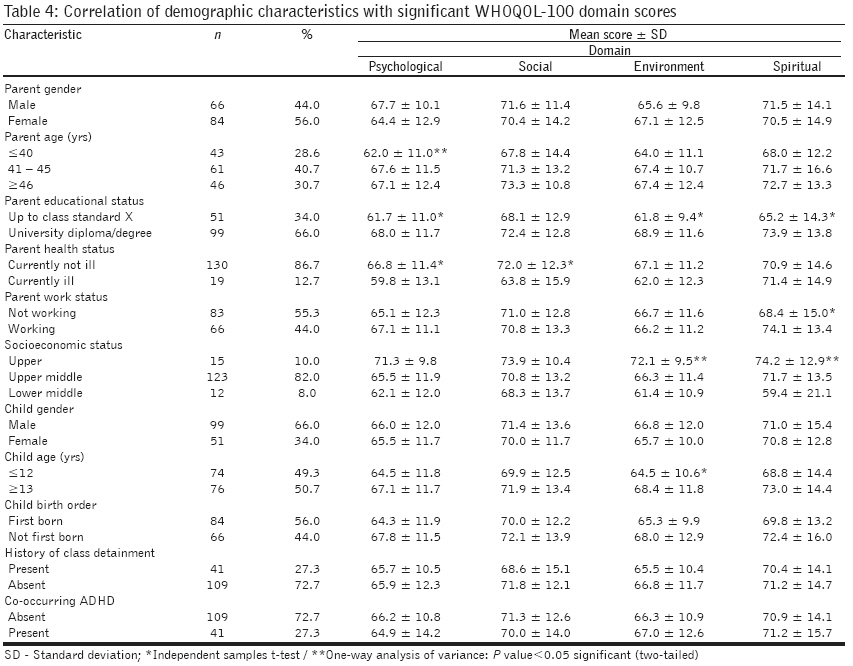
[ Z = 1.96 ( Z value for 95% confidence level); P = 0.1 (10% prevalence, expressed as decimal); C = 0.05 (confidence interval, expressed as decimal)]. The sample size calculated for the present study was 138 parents. However, we included the first consecutive 150 parents (either mother or father) who could read and understand English and were willing to participate in the study. Thus, the power of analysis for the present study was> 95%. No parent who could read and understand English refused to participate in the study. Parents having another child who had been earlier diagnosed as having SpLD were excluded from the study. Each parent was given the ′international World Health Organization Quality of Life-100 instrument (WHOQOL-100)′ to complete in a quiet secluded room during his/her last visit to our clinic but before the child′s diagnosis was informed. [10] Parents completed this self-administered questionnaire in 25 to 30 min. [10] As recommended, each parent used a two-week recall period for scoring all 100 items (questions). [10] This study was conducted from June 2006 to February 2007. Our study was approved by the scientific and ethics committees of our institution. All parents had signed an informed consent form to participate in the study. Measuring QOL of parents with WHOQOL-100 Data analyses Results The mean scores (±SD) of WHOQOL-100 domain and facet scores of study parents are given in [Table - 1]. There was little missing data for the WHOQOL-100 items [Table - 1]. Analysis of WHOQOL-100 domain scores of study parents Analysis of WHOQOL-100 facet scores of study parents Demographic variables Impact of demographic variables on "significant" WHOQOL-100 domain scores Multivariate analysis revealed that only parent gender being female "independently" predicted a "poor" psychological domain score of ≤60 ( P = 0.009, OR = 0.3, 95% CI 0.1 to 0.7); and parent gender being female, and parent being currently ill "independently" predicted a "poor" social relationships domain score of ≤60 ( P = 0.010, OR = 0.2, 95% CI 0.1 to 0.7; and P = 0.004, OR = 0.1, 95% CI 0.04 to 0.5, respectively). Impact of demographic variables on "significant" WHOQOL-100 facet scores Multivariate analysis revealed that parent gender being female, parent being currently ill, and, child gender being female "independently" predicted a "poor" energy facet score of ≤60 ( P = 0.010, OR = 0.3, 95% CI: 0.2 to 0.8; P = 0.028, OR = 0.3, 95% CI: 0.1 to 0.9; and, P = 0.048, OR = 2.2, 95% CI: 1.0 to 4.9, respectively); parent gender being female "independently" predicted a "poor" pfeel facet score of ≤60 ( P = 0.004, OR = 0.3, 95% CI: 0.1 to 0.7); and parent being currently ill, and parent working and earning an income "independently" predicted a "poor" leisur facet score of ≤60 ( P = 0.028, OR = 0.2, 95% CI: 0.1 to 0.9; and, P = 0.020, OR = 0.4, 95% CI: 0.2 to 0.9, respectively). Discussion Our study shows that parents of children with newly diagnosed SpLD regard four domains (psychological > environment > social relationships > spiritual) as significant contributors to their overall QOL. The spiritual domain is the least contributory and that too in a negative way. Multivariate analysis revealed that being a mother is an independent predictor of "poor" psychological and social relationships domain scores; and being currently ill is an independent predictor of a "poor" social relationships domain score. Our study also shows that these parents regard five facets (leisur > pfeel > energy > esteem > sex) as important contributors to their overall QOL. Multivariate analysis revealed that being currently ill is an independent predictor of "poor" leisur and energy facet scores; being in paid work is another independent predictor of a "poor" leisur facet score; being a mother is an independent predictor of "poor" pfeel and energy facet scores; and child being male is an independent predictor of "poor" energy facet score. To the best of our knowledge, ours is probably the first study that has addressed the QOL of parents having a child with SpLD and that too utilizing a detailed instrument, namely, the WHOQOL-100. Hence, we cannot compare our results with any previous work. What is the utility of the present study? First; it is well known that parents of children with SpLD experience a lot of stress and impaired mental health. [3] The present study has identified the significant clinical and socio-demographic variables which impact the quality of life of these parents and which need to be addressed by counselors right at the time SpLD is diagnosed in their child. For example, our results indicate that mothers in particular have significantly poor psychological health and social relationships; and parents who are currently ill, irrespective of their gender, have significantly poor social relationships. Keeping this in mind counselors should spend more time and have follow up visits especially for all mothers in general and for parents who are ill. Our study has also identified that parents who are working or currently ill get significantly less opportunities for recreation and leisure activities. Counselors should therefore advice such parents to make efforts to keep time aside each week for such activities. Our study results indicate that mothers experience significantly less feelings of contentment and have a negative view of the future, and have less energy, enthusiasm, and endurance to perform the necessary tasks of daily living. Also, parents who are currently ill and parents having a male child with SpLD have less energy, enthusiasm, and endurance to perform the necessary tasks of daily living. Apart from counseling sessions, such mothers/parents may benefit by doing regular ′yoga′ exercises or other relaxation techniques. New research should be conducted to measure the effectiveness of these strategies. Improving the QOL of parents would eventually improve the home environment and help rehabilitation of children with SpLD. [1],[2] Second; in general, there is also very little information available in world literature on QOL of parents of children having other neurodevelopmental disorders such as pervasive development disorder, cerebral palsy, or mental retardation. [13] We believe that our study results are an important contribution to help reduce this deficit. The present study has its limitations. First; we could not compare our study scores with any normative data as there are no population norms available for QOL of Indian parents. Second; after the parent had completed the WHOQOL-100 instrument we did not personally interview him/her to collect any further detailed information and this could have biased some of our results. [14] Third; as vernacular (Marathi or Gujarati) versions of the WHOQOL-100 instrument are not available, non-English-speaking parents were excluded from the study. However, our numbers of these parents were very small (less than five). Fourth; parents from the lower socio-economic strata of society were not represented in our study population. Either their children′s school authorities were not aware about SpLD or their parents were not motivated enough to bring their child to our clinic for assessment. Fifth; we did not attempt to reassess the QOL of these parents after initiation of psycho-educational interventions in their child. Many parents in our city cannot afford remedial education services; also it takes at least a year for remedial education to start showing improvement in child′s school performance; and many schools in our city just do not offer the necessary provisions (accommodations) even after the diagnosis of SpLD is confirmed. [2] However, we do not believe that these limitations adversely affect the utility of our results. Both due to the limitations as outlined above and the general paucity of data, there is a need for further study of this topic in clinics situated all over the world. Acknowledgments We thank Dr. D.P. Singh, Reader, Department of Research Methodology, Tata Institute of Social Sciences, Deonar, Mumbai for his help in the statistical analysis of the data; and the parents who participated in the study. We also thank Professor Suzanne Skevington, Professor of Health Psychology and Director of WHO Centre for the Study of Quality of Life, University of Bath, UK for her guidance in analyzing our data. The material in this publication is the result of use of the WHOQOL-100 instrument and the assistance of the World Health Organization is acknowledged.References
Copyright 2009 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp09028t3.jpg] [jp09028t5.jpg] [jp09028t2.jpg] [jp09028t1.jpg] [jp09028t4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}