
|
Journal of Postgraduate Medicine
Medknow Publications and Staff Society of Seth GS Medical College and KEM Hospital, Mumbai, India
ISSN: 0022-3859 EISSN: 0972-2823
Vol. 55, Num. 2, 2009, pp. 143-149
|
Journal of Postgraduate Medicine, Vol. 55, No. 2, April-June, 2009, pp. 143-149
Review Article
Targeting connexin 43 in diabetic wound healing: Future perspectives
Bajpai S, Shukla VK, Tripathi K, Srikrishna S, Singh RK
Department of Biochemistry, Faculty of Science, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005
Correspondence Address:Department of Biochemistry, Faculty of Science, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005
rakesh_bc@bhu.ac.in/rakeshbhu@yahoo.com
Date of Submission: 30-Jul-2008
Date of Decision: 28-Dec-2008
Date of Acceptance: 15-Jan-2009
Code Number: jp09040
PMID: 19550065
DOI: 10.4103/0022-3859.48786
Abstract The unknown mechanisms of impaired tissue repair in diabetes mellitus are making this disease a serious clinical problem for the physicians worldwide. The lacuna in the knowledge of the etiology of diabetic wounds necessitates more focused research in order to develop new targeting tools with higher efficacy for their effective management. Gap-junction proteins, connexins, have shown some promising results in the process of diabetic wound healing. Till now the role of connexins has been implicated in peripheral neuropathy, deafness, skin disorders, cataract, germ cell development and treatment of cancer. Recent findings have revealed that gap junctions play a key role in normal as well as diabetic wound healing. The purpose of this review is to provide the information related to etiology, epidemiology, clinical presentation of diabetic wounds and to analyze the role of connexin 43 (Cx43) in the diabetic wound healing process. The current control strategies and the future research challenges have also been discussed briefly in this review.
Keywords: Connexin-43, diabetes, diabetic wound, gap-junction proteins
The process of wound healing is a synchronized and magnificently coordinated interplay of several cellular and biochemical components. The precise and optimum response of various inflammatory elements and growth factors is essentially required during the normal wound healing process. In case of diabetes this synchronization is interrupted due to several extrinsic (high glucose level, oxidative stress) as well as intrinsic (cytokines, pro-apoptotic molecules like bim, bad, bax, bak and anti-apoptotic molecules viz. bcl-2, bcl-xL) factors, which in turn result in delayed wound healing. [1] Research conducted so far is mainly confined to the area of controlling the microbial infections through the use of modified dressings, growth factors, combinations of antibiotics and few other recently developed techniques that will be discussed later. The increasing incidence of diabetic wound patients impels us to search for causal factors, and design new therapeutic strategies to combat this emerging issue.
The current research regarding the identification and characterization of the connexin gene family has led to the discovery of a variety of inherited human diseases that result from mutations in these genes. [2],[3] These findings emphasize the importance of gap junctions in the normal functioning of the cells. Connexins are the structural gap-junction proteins that form channels for exchange of small molecules between connected cells. The cells efficiently utilize these gap junctions for electrical synapse and sharing of intracellular metabolites that coordinate various metabolic events. The role of gap junctions in tissue reactions, and its potential to damage or heal the wounds, has been widely debated and discussed by researchers and clinicians worldwide. [4] Studies conducted in animals as well as humans have drawn special attention towards gap junctions due to the fact that connexins (especially Cx43 and Cx26) play a crucial role in the wound healing process. [5] This review opens new approaches for understanding the etiology, epidemiology along with clinical features, new treatment strategies and last but not the least, a new panorama of gap junction proteins with special reference to the role of Cx43 in diabetic wound healing.
Epidemiology and Etiology
Rapid urbanization, sedentary lifestyle and imbalanced/ junk foods are the major factors for increased prevalence of diabetes today. A study including all age groups worldwide estimated about 2.8% prevalence of diabetes in the year 2000 and it is expected to rise up to 4.4% by the year 2030. [6] Nearly ten countries are estimated to have highest number of people suffering from diabetes in 2000 with India, China and the US occupying the top three positions, which appears to remain unchanged till 2030. [6] Moreover, there is a gross under-reporting of the current epidemiological data in developing countries. Recently, a diabetic awareness campaign launched by a few non-governmental organizations (NGOs) in the northern part of India revealed that about 20-25% of the population has significantly increased blood sugar levels (unpublished data). The clinical complications of diabetes like neuropathy, nephropathy, cardiac myopathy and retinopathy are also significantly increasing. [7],[8],[9] Diabetic ulcers are generally neuropathic in nature, though a few ischemic and neuroischemic cases contribute to the list. [10] It is now clear that there is about 25% lifetime risk of occurrence of diabetic foot ulcers in patients suffering from diabetes, [11] and in every 30 sec the lower limb of a person is amputated because of this fatal disease in the world. [12]
Diabetic ulcers are endemic in the rural areas of developing countries like India. This would be attributed to illiteracy, lack of health consciousness and poor health amenities. [13] In these countries, walking barefoot is a major risk factor for an increased prevalence of diabetic foot ulcers. Notwithstanding, intensive prevention and care can reduce the incidence of ulcers by 25%, but cost-effective and optimum preventive measures are yet to be explored. [14] Moreover, acute diabetic wounds have their impact on the socioeconomic life of the people and greatly reduce their working efficiency.
In the context of unclear etiology of diabetic wounds, it is essential to mention that factors like impaired glucose metabolism, [15] hampered migration of fibroblast cells to the wound site, [16] prolonged inflammation, decreased growth factors like platelet derived growth factor (PDGF), [17] keratinocyte growth factor (KGF), [18] enhanced protease activity, [19] essentially upregulated microbial activity, [20] endothelial cell apoptosis [1] and abnormal connexins expression [21] together play a very significant role in the process of wound healing in diabetes.
Clinical Presentation
Diabetic ulcers are essentially characterized by delayed contraction of the wound, hampered migration of fibroblast cells to the wound site, [16] reduced deposition of extracellular matrix, [22] reduced collagen synthesis, abnormal functioning of neutrophils and decreased number of macrophages. [23] Further, the reduced expression of vascular endothelial growth factor receptor-3 (VEGFR-3), along with its ligands VEGFR-C and VEGFR-D, lead to poor lymphatic vessel formation that eventually delays the healing process in diabetic wounds. [24] Diabetic wounds are also characterized by decreased levels of various growth factors like platelet derived growth factor (PDGF), transforming growth factor (TGF-β), fibroblast growth factor (FGF), vascular endothelial growth factor (VEGF). [23],[25] However, the main obstacle in wound healing is impairment of blood flow that results in oxygen deficiency and delayed migration of fibroblast cells to the wound site resulting in delayed tissue remodeling at the wound site. [16] The expression levels of various matrixmetalloproteinases (MMPs) have been found to be elevated in diabetic wounds, impairing the rate of diabetic wound healing by the destruction of extracellular matrix, but the underlying molecular mechanisms for their decreased or increased production are yet to be resolved. [19],[26]
Therapeutic Options and Novel Approaches
Due to an unclear etiology, the treatment options for diabetic wounds are far from satisfactory. However, recent advances have provided newer understandings to manage diabetic wounds. A few FDA-approved advanced dressing materials like sodium carboxyl-methyl-cellulose, alginate and semi-permeable polymeric membrane dressings, [27] are being used topically for the management of diabetic wounds. Several other modified dressing materials like biocompatible wound dressings made of gelatin containing epidermal growth factor, [28] protease-modulating matrixes combined with autologous growth factors, [29] recombinant human acidic fibroblast growth factor impregnated in chitosan cross-linked collagen sponge (CCCS/FGF), [30] polyhydrated ionogen (formulation of metallic ions and citric acid) have also been reported to be beneficial in early wound closure of diabetic wounds. [31]
Although new treatments for diabetic wound are being introduced, their efficacy and safety are not optimal and require further improvement. The applications of various growth factors have been found to accelerate the wound healing process significantly in diabetic conditions. [32],[33] The topical application of PDGF, [33] nerve growth factor (NGF), [34] recombinant human-VEGF, [35] recombinant human epidermal growth factor (REGEN- D TM 50), [36] diphenyhydantoin sodium, [37] chrysalin-a thrombin peptide, [38] aminated beta 1,3-D glucan, [39] talactoferrin alpha-a recombinant human lactoferrin [40] and a few metal ions like copper ions [41] have been proved to elicit a substantial healing effect in diabetic wounds in human and animal models. However, only PDGF and its analogues are approved by the United States Food and Drug Administration (US FDA) for human use.
The intralesional/subcutaneous or intraperitoneal injections of citoprot-P containing recombinant human EGF, [42] dalteparin-a low molecular weight heparin compound, [43] simvastatin, [44] bioactive lipids like sphingosine-1 phosphate [45] and lipid-lowering agents like statins [46] have been found to enhance the rate of angiogenesis in the diabetic wound healing process in human and other experimental models. Similarly, the oral administration of L-arginine, the substrate for nitric oxide synthesis, and nitric oxide itself have a substantial role in increasing the rate of angiogenesis and collagen deposition thereby enhancing the rate of diabetic wound healing. [47],[48],[49]
In addition, several other novel approaches like biocompatible nanofibers impregnated with recombinant human epidermal growth factor (EGF), [50] biotinylated glycyl-histidyl-lysyl (GHK) incorporated collagen matrices, [51] HMGB-1 (high mobility group box 1 protein), [52] IGF-1(insulin-like growth factor-1), [53] endothelin-1 (a key signaling protein) [54] and stromal derived growth factor-alpha (SDF-1α) [55] have proved to accelerate the rate of re-epithelization, granular tissue formation, eventually leading to increased rate of diabetic wound healing.
In spite of the significant development in wound research the lack of efficacy, reliability and compatibility of these formulations remains a major drawback in the management of diabetic wounds. Most of the current studies are still under evaluation and limited to experimental conditions. Impaired cell-to-cell signaling, prolonged inflammatory responses and cellular apoptosis are the major features associated with diabetic wounds and in this context, a detailed investigation of the underlying role of gap-junction proteins in regulation of these events is urgently required.
Emerging Role of Cx43 in Diabetic Wound Healing
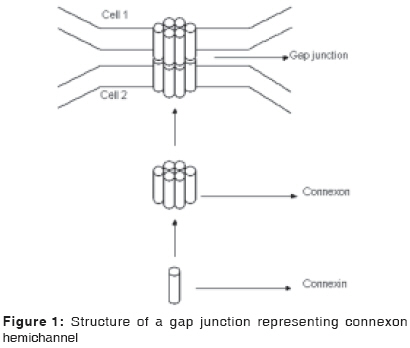
A new era of wound healing research has emerged with the discovery of involvement of gap-junction proteins in normal and diabetic wound healing processes. Gap junctions are intercellular junctions containing hydrophilic membrane channels that allow direct communication between neighboring cells through the diffusion of ions, metabolites and cell-signaling molecules. These junctions are tightly packed in hexagonal array termed connexon, which is made up of six connexin protein subunits [Figure - 1]. These channels mediate various cell-to-cell communications that are essential for regulation of cellular growth, differentiation, development as well as apoptosis. These proteins have also been implicated in many human diseases like cardiovascular, peripheral neuropathy, skin disorders and cataract. Connexins are found in vertebrates while their functional homologues, innexins are identified in invertebrates. [56] In humans more than 20 connexins are expressed [57] and of these the Cx43 is abundantly expressed in keratinocytes, [58] dermal fibroblasts, [59] vascular system, [60],[61] skin appendages, [62] macrophages, neutrophils and mast cells. [63] It plays a key role in cellular communication to maintain tissue homeostasis and angiogenesis. [64]
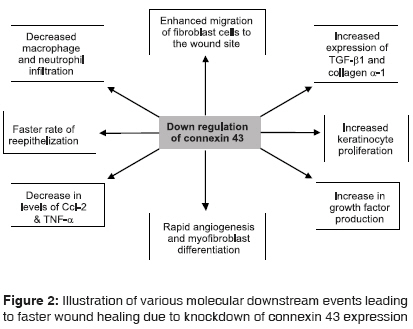
In normal rodents and humans there is a natural down-regulation of Cx43 and an up-regulation of Cx26 and Cx30 in keratinocytes at the wound edges. [58],[65],[66] The down-regulation of Cx43 further results in increased levels of TGF-β, collagen α-1 and decreased levels of chemokine ligand-2, tumor necrosis factor alpha (TNFα) and reduced infiltration of neutrophils, macrophages at the wound site [Figure - 2]. The down-regulation of Cx43 also promotes rapid angiogenesis, enhanced fibroblast migration and keratinocyte proliferation leading to earlier wound contraction and faster wound closure. [67] However, the complete silencing of Cx43 transcripts using antisense oligodeoxynucleotides (asODNs) at wound sites result in faster wound closure with reduced inflammation and scar formation. It is also reported that the rate of re-epithelization and granulation at the wound site is enhanced by 47%, 55%, and 27% during Day 1, 2 and 4, respectively using Cx43 asODN treatment as compared to sense-treated controls. [68]
It is now well established that the Cx43 is abnormally expressed and dynamically regulated in intact skin including the dermis, epidermis and granular tissues in diabetic and chronic wounds in comparison with normal wounds and its down-regulation significantly enhances the rate of wound healing in diabetic conditions. [21],[65] Hence, a thorough understanding of the expression and turnover profiles of connexins in general and Cx43 in particular is required for formulating newer strategies for effective control of diabetic wounds.
Correlation of Connexin 43 with Cellular Apoptosis
Several studies have shown that there is an increased endothelial cell apoptosis in the case of diabetic wounds. [69],[70] The optimal activity of connexin hemichannels is required for normal physiological functions of the cell but its prolonged and uncontrolled activities can potentially lead to cell death. [71] This fact was reinforced by some prominent studies which showed that continuous opening of hemichannels formed by Cx43 induces cell death in nervous tissue during ischemia. [72] It was also predicted that ions and toxic molecules like nitric oxide (NO), superoxide (O 2- ), nicotinamide adenine dinucleotide (NAD + ), present in higher concentrations in the injured cells, could be transported from injured to normal cells leading to propagation of cell death. [72] Recently it has been observed that the altered Cx43 expression in cardiac ventricles resulted in myocyte apoptosis causing tissue injury and post-ischemic cardiac dysfunction. [71],[73] In case of cerebral ischemia also, the dying glial cells kill the neighboring cells by exporting cell death components via the gap junctions leading to amplified cell injury. [74]
The combinatorial role of Cx43 and gap junctional intercellular communications (GJIC), has been implicated in the propagation of apoptosis. It has been observed that a Cx43-mediated inhibition of GJIC leads to decreased apoptosis in rat bladder carcinoma cell lines (BC-31 cells). Further, it is predicted that various oncogenes like v-Ha-ras, v-raf, v-src and v-fps down-regulate GJIC that eventually results in decreased apoptosis. [57] Therefore, the up-regulation of GJIC might promote apoptosis of cancer cells. [75] Additionally, the Cx43-linked apoptosis has also been shown to be mediated through down-regulation of bcl-2, a anti-apoptotic factor, in human glioblastoma cells. [76] Further, recent evidences suggest that Cx43 along with other connexins might have additional functions, which could be important in cell death or survival by mechanisms which could be independent of cell to cell communication. [77] However, the Cx43-mediated apoptosis of endothelial and other cells in diabetic wounds is yet to be elucidated.
Factors Affecting Gap Junctional Gating and Cx43 Regulation
The gating or opening of gap junctional channels allows various apoptotic and inflammatory signals between cells eventually leading to increased endothelial cell apoptosis and delayed wound contraction in diabetes. Gating of gap junction channels is generally affected by calcium ion concentration, [78] pH, [79] transjunctional membrane potential [80],[81] and protein phosphorylation. [82],[83] An increased calcium ion concentration and decreased intracellular acidification (pH) results in closure of gap junction channels. [78],[79] Further, the decreased expression and phosphorylation of Cx43 by protein kinase C leads to an inhibition in cell-cell coupling, which may lead to blockage in the passage of various inflammatory and apoptotic signals resulting in early healing of diabetic wounds. [56]
The Cx43 is also known to be regulated by various factors like glucose, [84] , nitric oxide, [85] and growth factors like FGF, [86] TGF-β, [87] EGF, [88] PDGF, [89] nerve growth factor, [90] ATP, [91] and few cytokines like TNF-α and IFN-γ[92] though the precise molecular mechanisms by which they regulate Cx43 is not fully understood. However, all these factors contribute significantly in wound healing, and therefore, their effective management could lead to faster wound healing in diabetic patients.
Cx43-Mediated Inflammatory Response The Cx43 is expressed by most of the immunocompetent cells including macrophages, neutrophils, mast cells and lymphocytes. [93] It is also expressed along with Cx40 in polymorphonuclear cells under inflammatory conditions in humans. [94] The increased expression of Cx43 has shown to increase the levels of various inflammatory and immunomodulatory molecules like interleukin-1 (IL-1) and interleukin-6 (IL-6), TGF-β in co-cultured endothelial cells and smooth muscle cells. [95] During the development of atheroma in case of low-density-lipoprotein-deficient mice and human atherosclerotic plaques, a redistribution of Cx43 along with Cx37 and Cx40 occurs in the arterial wall suggesting the role for connexins in inflammatory responses. [96] The growing incidence of involvement of connexins in relation with gap junctions in inflammatory responses in normal wound tissues strongly suggests a key functional role of these candidates in diabetic wound healing processes.
Concluding Remarks and Future Research Challenges
Diabetic wound healing is a complicated process and requires the superfine coordinated activity of several cell types and mechanisms. The traditional approaches to combat diabetic wounds are not very efficient. The exact molecular mechanisms that delay diabetic wound healing largely remain to be elucidated. Most of the studies conducted so far have been confined to intracellular signaling pathways but tissue remodeling also essentially involves intercellular communication through gap junctions. The effect of different hypoglycemic drugs, few cytokines and reactive oxygen species on regulation of connexin expression, in general, needs to be explored in cells like endothelial, fibroblasts and macrophages in diabetic wounds. In addition, the precise mechanisms of Cx43 expression either in endothelial cells or leukocytes, which regulate various inflammatory responses in diabetic wounds, are a subject of future investigations. Therefore, intensive research is required to explore the novel mechanisms linked to gap junction communication in order to design newer treatment strategies for cost-effective management of diabetic wounds.
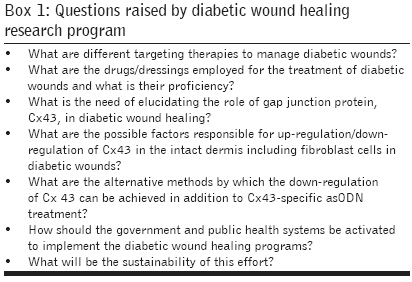
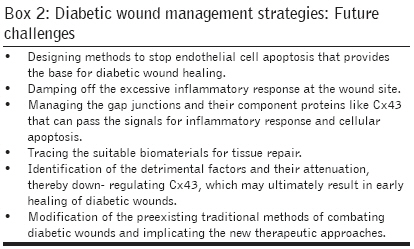
The initiative of elimination of diabetic ulcers itself raises several questions regarding the therapeutic implementation in the near future [Box 1]. This initiative also includes some multidisciplinary management programs for diabetic wounds, which includes care for all the people who are at the risk of diabetic ulcers. The research investments are the need of present era to fill the lacuna in the wound research with some novel approaches and therapeutic compounds/drugs [Box 2]-. In spite of this, sincere commitments will be required for implementation of diabetic ulcer eradication programs to benefit the common man of the society.
Acknowledgment Authors are highly thankful to Dr. H. P. Pandey, Professor of Biochemistry and Dr. A. Khanna, Reader, Department of English, Banaras Hindu University, Varanasi for their support in reviewing this manuscript. The financial assistance extended by the Department of Science and Technology, New Delhi is highly acknowledged.
References
| 1. | Rai NK, Tripathi K, Sharma D, Shukla VK. Apoptosis: A basic physiologic process in wound healing. Int J Low Extrem Wounds 2005;4:138-44. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Kelsell DP. Connexin mutations in human disease. Exp Dermatol 2004;13:661-2. Back to cited text no. 2 [PUBMED] [FULLTEXT] |
| 3. | Richard G. Connexin gene pathology. Clin Exp Dermatol 2003;28:397-409. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Goliger JA, Paul D L. Wounding alters epidermal connnexin expression and gap junction-mediated intercellular communication. Mol Biol Cell 1995;6:1491-501. Back to cited text no. 4 |
| 5. | Brandner JM, Zacheja S, Houdek P, Moll I, Lobmann R. Expression of matrix metalloproteinases, cytokines, and connexins in diabetic and nondiabetic human keratinocytes before and after transplantation into an ex vivo wound-healing model. Diabetes Care 2008;31:114-20. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes. Diabetes Care 2004;27:1047-53. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Friedman EA. Advanced glycation end -products in diabetic nephropathy. Nephrol Dial Transplant 1999;14:1-9. Back to cited text no. 7 |
| 8. | Podwall D, Gooch C. Diabetic neuropathy: Clinical features, etiology and therapy. Curr Neurol Neurosci Rep 2004;4:55-61. Back to cited text no. 8 [PUBMED] |
| 9. | Cai L, Kang YJ. Oxidative stress and diabetic cardiomyopathy. Cardiovasc Toxicol 2001;01:181-93. Back to cited text no. 9 |
| 10. | Rathur HM, Boulton AJ. The diabetic foot. Clin Dermatol 2007;25:109-20. Back to cited text no. 10 [PUBMED] [FULLTEXT] |
| 11. | Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 2005;293:217-28. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Act IDFTt. diabetes and foot care. Brussels:International Diabetes Federation 2005. Back to cited text no. 12 |
| 13. | Shukla VK, Ansari MA, Gupta SK. Wound healing research: A perspective from India. Int J Low Extrem Wounds 2005;4:7-8. Back to cited text no. 13 [PUBMED] [FULLTEXT] |
| 14. | Ragnarson-Tennvall G, Apelqvist J. Prevention of diabetes-related foot ulcers and amputations: A cost-utility analysis based on Markov model simulations. Diabetologia 2001;44:2077-87. Back to cited text no. 14 |
| 15. | Rai NK, Suryabhan, Ansari M, Kumar M, Shukla VK, Tripathi K. Effect of glycaemic control on apoptosis in diabetic wounds. J Wound Care 2005;14:277-81. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Lerman OZ, Galiano RD, Armour M, Levine JP, Gurtner GC. Cellular dysfunction in the diabetic fibroblast: Impairment in migration, vascular endothelial growth factor production, and response to hypoxia. Am J Pathol 2003;162:303-12. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Doxey DL, Ng MC, Dill RE, Iacopino AM. Platelet-derived growth factor levels in wounds of diabetic rats. Life Sci 1995;57:1111-23. Back to cited text no. 17 [PUBMED] [FULLTEXT] |
| 18. | Werner S, Breeden M, Hubner G, Greenhalgh DG, Longaker MT. Induction of keratinocyte growth factor expression is reduced and delayed during wound healing in the genetically diabetic mouse. J Invest Dermatol 1994;103:469-73. Back to cited text no. 18 |
| 19. | Lobmann R, Ambrosch A, Schultz G, Waldmann K, Schiweck S, Lehnert H. Expression of matrix-metalloproteinases and their inhibitors in the wounds of diabetic and non-diabetic patients. Diabetologia 2002;45:1011-6. Back to cited text no. 19 [PUBMED] [FULLTEXT] |
| 20. | Shaw JE, Boulton AJ. The pathogenesis of diabetic foot problems: An overview. Diabetes 1997;46:S58-61. Back to cited text no. 20 [PUBMED] |
| 21. | Wang CM, Lincoln J, Cook JE, Becker DL. Abnormal connexin expression underlies delayed wound healing in diabetic skin. Diabetes 2007;56:2809-17. Back to cited text no. 21 [PUBMED] [FULLTEXT] |
| 22. | Loots MA, Lamme EN, Zeegelaar J, Mekkes JR, Bos JD, Middelkoop E. Differences in cellular infiltrate and extracellular matrix of chronic diabetic and venous ulcers versus acute wounds. J Invest Dermatol 1998;111:850-7. Back to cited text no. 22 [PUBMED] |
| 23. | Kapoor M, Appleton I. Wound healing abnormalities and future therapeutic targets. Curr Anaesth Crit Care 2005;16:88-93. Back to cited text no. 23 |
| 24. | Maruyama K, Asai J, Ii M, Thorne T, Losordo DW, D'Amore PA. Decreased macrophage number and activation lead to reduced lymphatic vessel formation and contribute to impaired diabetic wound healing. Am J Pathol 2007;170:1178-91. Back to cited text no. 24 [PUBMED] [FULLTEXT] |
| 25. | Kim BC, Kim HT, Park SH, Cha JS, Yufit T, Kim SJ, et al . Fibroblasts from chronic wounds show altered TGF-beta-signaling and decreased TGF-beta Type II receptor expression. J Cell Physiol 2003;195:331-6. Back to cited text no. 25 [PUBMED] [FULLTEXT] |
| 26. | Muller M, Trocme C, Lardy B, Morel F, Halimi S, Benhamou PY. Matrix metalloproteinases and diabetic foot ulcers: The ratio of MMP-1 to TIMP-1 is a predictor of wound healing. Diabetes Med 2008;25:419-26. Back to cited text no. 26 |
| 27. | Eldor R, Raz I, Ben Yehuda A, Boulton AJ. New and experimental approaches to treatment of diabetic foot ulcers: A comprehensive review of emerging treatment strategies. Diabetes Med 2004;21:1161-73. Back to cited text no. 27 |
| 28. | Ulubayram K, Nur Cakar A, Korkusuz P, Ertan C, Hasirci N. EGF containing gelatin-based wound dressings. Biomaterials 2001;22:1345-56. Back to cited text no. 28 [PUBMED] [FULLTEXT] |
| 29. | Kakagia DD, Kazakos KJ, Xarchas KC, Karanikas M, Georgiadis GS, Tripsiannis G, et al . Synergistic action of protease-modulating matrix and autologous growth factors in healing of diabetic foot ulcers: A prospective randomized trial. J Diabetes Compl 2007;21:387-91. Back to cited text no. 29 |
| 30. | Wang W, Lin S, Xiao Y, Huang Y, Tan Y, Cai L, et al . Acceleration of diabetic wound healing with chitosan-crosslinked collagen sponge containing recombinant human acidic fibroblast growth factor in healing-impaired STZ diabetic rats. Life Sci 2008;82:190-204. Back to cited text no. 30 [PUBMED] [FULLTEXT] |
| 31. | Pirayesh A, Dessy LA, Rogge FJ, Hoeksema HJ, Sinove YM, Dall' Antonia A, et al . The efficacy of a polyhydrated ionogen impregnated dressing in the treatment of recalcitrant diabetic foot ulcers: A multi-centre pilot study. Acta Chir Belg 2007;107:675-81. Back to cited text no. 31 [PUBMED] |
| 32. | Galeano M, Deodato B, Altavilla D, Cucinotta D, Arsic N, Marini H, et al . Adeno-associated viral vector-mediated human vascular endothelial growth factor gene transfer stimulates angiogenesis and wound healing in the genetically diabetic mouse. Diabetologia 2003;46:546-55. Back to cited text no. 32 [PUBMED] [FULLTEXT] |
| 33. | Cheng B, Liu HW, Fu XB, Sun TZ, Sheng ZY. Recombinant human platelet-derived growth factor enhanced dermal wound healing by a pathway involving ERK and c-fos in diabetic rats. J Dermatol Sci 2007;45:193-201. Back to cited text no. 33 [PUBMED] [FULLTEXT] |
| 34. | Generini S, Tuveri MA, Matucci Cerinic M, Mastinu F, Manni L, Aloe L. Topical application of nerve growth factor in human diabetic foot ulcers: A study of three cases. Exp Clin Endocrinol Diabetes 2004;112:542-4. Back to cited text no. 34 [PUBMED] [FULLTEXT] |
| 35. | Hanft JR, Pollak RA, Barbul A, van Gils C, Kwon PS, Gray SM, et al . Phase I trial on the safety of topical rhVEGF on chronic neuropathic diabetic foot ulcers. J Wound Care 2008;17:30-2,34-7. Back to cited text no. 35 [PUBMED] [FULLTEXT] |
| 36. | Mohan VK. Recombinant human epidermal growth factor (REGEN-D 150): Effect on healing of diabetic foot ulcers. Diabetes Res Clin Pract 2007;78:405-11. Back to cited text no. 36 [PUBMED] [FULLTEXT] |
| 37. | Chan FC, Kennedy C, Hanson RP, O'Sullivan B, Kelly J, Bouchier-Hayes D. Topical diphenylhydantoin sodium can improve healing in a diabetic incisional animal wound model. J Wound Care 2007;16:359-63. Back to cited text no. 37 [PUBMED] [FULLTEXT] |
| 38. | Fife C, Mader JT, Stone J, Brill L, Satterfield K, Norfleet A, et al . Thrombin peptide Chrysalin stimulates healing of diabetic foot ulcers in a placebo-controlled phase I/II study. Wound Repair Regen 2007;15:23-34. Back to cited text no. 38 [PUBMED] [FULLTEXT] |
| 39. | Berdal M, Appelbom HI, Eikrem JH, Lund A, Zykova S, Busund LT, et al . Aminated beta-1,3-D-glucan improves wound healing in diabetic db/db mice. Wound Repair Regen 2007;15:825-32. Back to cited text no. 39 [PUBMED] [FULLTEXT] |
| 40. | Lyons TE, Miller MS, Serena T, Sheehan P, Lavery L, Kirsner RS, et al . Talactoferrin alfa, a recombinant human lactoferrin promotes healing of diabetic neuropathic ulcers: A phase 1/2 clinical study. Am J Surg 2007;193:49-54. Back to cited text no. 40 [PUBMED] [FULLTEXT] |
| 41. | Borkow G, Gabbay J, Zatcoff RC. Could chronic wounds not heal due to too low local copper levels? Med Hypotheses 2008;70:610-3. Back to cited text no. 41 [PUBMED] [FULLTEXT] |
| 42. | Fernandez-Montequin JI, Infante-Cristia E, Valenzuela-Silva C, Franco-Perez N, Savigne-Gutierrez W, Artaza-Sanz H, et al . Intralesional injections of Citoprot-P (recombinant human epidermal growth factor) in advanced diabetic foot ulcers with risk of amputation. Int Wound J 2007;4:333-43. Back to cited text no. 42 |
| 43. | Kalani M, Silveira A, Blomback M, Apelqvist J, Eliasson B, Eriksson JW, et al . Beneficial effects of dalteparin on haemostatic function and local tissue oxygenation in patients with diabetes, severe vascular disease and foot ulcers. Thromb Res 2007;120:653-61. Back to cited text no. 43 |
| 44. | Bitto A, Minutoli L, Altavilla D, Polito F, Fiumara T, Marini H, et al . Simvastatin enhances VEGF production and ameliorates impaired wound healing in experimental diabetes. Pharmacol Res 2008;57:159-69. Back to cited text no. 44 |
| 45. | Kawanabe T, Kawakami T, Yatomi Y, Shimada S, Soma Y. Sphingosine 1-phosphate accelerates wound healing in diabetic mice. J Dermatol Sci 2007;48:53-60. Back to cited text no. 45 |
| 46. | Gulcan E, Gulcan A, Erbilen E, Toker S. Statins may be useful in diabetic foot ulceration treatment and prevention. Med Hypotheses 2007;69:1313-5. Back to cited text no. 46 [PUBMED] [FULLTEXT] |
| 47. | Arana V, Paz Y, Gonzalez A, Mendez V, Mendez JD. Healing of diabetic foot ulcers in L-arginine-treated patients. Biomed Pharmacother 2004;58:588-97. Back to cited text no. 47 |
| 48. | Witte MB, Kiyama T, Barbul A. Nitric oxide enhances experimental wound healing in diabetes. Br J Surg 2002;89:1594-601. Back to cited text no. 48 [PUBMED] [FULLTEXT] |
| 49. | Witte MB, Thornton FJ, Tantry U, Barbul A. L-Arginine supplementation enhances diabetic wound healing: Involvement of the nitric oxide synthase and arginase pathways. Metabolism 2002;51:1269-73. Back to cited text no. 49 [PUBMED] [FULLTEXT] |
| 50. | Choi JS, Leong KW, Yoo HS. In vivo wound healing of diabetic ulcers using electrospun nanofibers immobilized with human epidermal growth factor (EGF). Biomaterials 2008;29:587-96. Back to cited text no. 50 [PUBMED] [FULLTEXT] |
| 51. | Arul V, Kartha R, Jayakumar R. A therapeutic approach for diabetic wound healing using biotinylated GHK incorporated collagen matrices. Life Sci 2007;80:275-84. Back to cited text no. 51 [PUBMED] [FULLTEXT] |
| 52. | Straino S, Di Carlo A, Mangoni A, De Mori R, Guerra L, Maurelli R, et al . High-mobility group box 1 protein in human and murine skin: Involvement in wound healing. J Invest Dermatol 2008;128:1545-53. Back to cited text no. 52 |
| 53. | Yu DH, Mace KA, Hansen SL, Boudreau N, Young DM. Effects of decreased insulin-like growth factor-1 stimulation on hypoxia inducible factor 1-alpha protein synthesis and function during cutaneous repair in diabetic mice. Wound Repair Regen 2007;15:628-35. Back to cited text no. 53 [PUBMED] [FULLTEXT] |
| 54. | Solini A, Santini E, Madec S, Cuccato S, Ferrannini E. Effects of endothelin-1 on fibroblasts from type 2 diabetic patients: Possible role in wound healing and tissue repair. Growth Factors 2007;25:392-9. Back to cited text no. 54 [PUBMED] [FULLTEXT] |
| 55. | Badillo AT, Chung S, Zhang L, Zoltick P, Liechty KW. Lentiviral gene transfer of SDF-1alpha to wounds improves diabetic wound healing. J Surg Res 2007;143:35-42. Back to cited text no. 55 [PUBMED] [FULLTEXT] |
| 56. | Wei CJ, Xu X, Lo CW. Connexins and cell signaling in development and disease. Annu Rev Cell Dev Biol 2004;20:811-38. Back to cited text no. 56 [PUBMED] [FULLTEXT] |
| 57. | Yamasaki H, Naus CC. Role of connexin genes in growth control. Carcinogenesis 1996;17:1199-213. Back to cited text no. 57 [PUBMED] [FULLTEXT] |
| 58. | Coutinho P, Qiu C, Frank S, Tamber K, Becker D. Dynamic changes in connexin expression correlate with key events in the wound healing process. Cell Biol Int 2003;27:525-41. Back to cited text no. 58 [PUBMED] [FULLTEXT] |
| 59. | Moyer KE, Davis A, Saggers GC, Mackay DR, Ehrlich HP. Wound healing: The role of gap junctional communication in rat granulation tissue maturation. Exp Mol Pathol 2002;72:10-6. Back to cited text no. 59 [PUBMED] [FULLTEXT] |
| 60. | Pepper MS, Montesano R, el Aoumari A, Gros D, Orci L, Meda P. Coupling and connexin 43 expression in microvascular and large vessel endothelial cells. Am J Physiol 1992;262:C1246-57. Back to cited text no. 60 [PUBMED] [FULLTEXT] |
| 61. | Polacek D, Bech F, McKinsey JF, Davies PF. Connexin43 gene expression in the rabbit arterial wall: Effects of hypercholesterolemia, balloon injury and their combination. J Vasc Res 1997;34:19-30. Back to cited text no. 61 [PUBMED] |
| 62. | Guo H, Acevedo P, Parsa FD, Bertram JS. Gap-junctional protein connexin 43 is expressed in dermis and epidermis of human skin: Differential modulation by retinoids. J Invest Dermatol 1992;99:460-7. Back to cited text no. 62 |
| 63. | Orta EO, Evans WH. Gap junctions and connexins: Potential contributors to immunological synapse. Leuk Biol 2002;72:636-42. Back to cited text no. 63 |
| 64. | Willmott T, Leach L. The effects of high glucose on connexin 43 in human endothelial cells. J Anat 2002;200:532. Back to cited text no. 64 [PUBMED] [FULLTEXT] |
| 65. | Goliger JA, Paul DL. Wounding alters epidermal connnexin expression and gap junction-mediated intercellular communication. Mol Biol Cell 1995;6:1491-501. Back to cited text no. 65 [PUBMED] [FULLTEXT] |
| 66. | Brandner JM, Houdek P, Husing B, Kaiser C, Moll I. Connexins 26, 30, and 43: Differences among spontaneous, chronic and accelerated human wound healing. J Invest Dermatol 2004;122:1310-20. Back to cited text no. 66 |
| 67. | Mori R, Power KT, Wang CM, Martin P, Becker DL. Acute down regulation of connexin43 at wound sites leads to a reduced inflammatory response, enhanced keratinocyte proliferation and wound fibroblast migration. J Cell Sci 2006;119:5193-203. Back to cited text no. 67 [PUBMED] [FULLTEXT] |
| 68. | Qiu C, Coutinho P, Frank S, Franke S, Law LY, Martin P, et al . Targeting connexin43 expression accelerates the rate of wound repair. Curr Biol 2003;13:1697-703. Back to cited text no. 68 [PUBMED] [FULLTEXT] |
| 69. | Artwohl M, Graier WF, Roden M, Bischof M, Freudenthaler A, Waldhausl W, et al . Diabetic LDL triggers apoptosis in vascular endothelial cells. Diabetes 2003;52:1240-7. Back to cited text no. 69 |
| 70. | Ho FM, Liu SH, Liau CS, Huang PJ, Lin-Shiau SY. High glucose-induced apoptosis in human endothelial cells is mediated by sequential activation of c-jun NH 2 terminal kinase and caspase-3. Circulation 2000;101:2618-24. Back to cited text no. 70 [PUBMED] [FULLTEXT] |
| 71. | Rodriguez-Sinovas A, Cabestrero A, Lopez D, Torre I, Morente M, Abellan A, et al . The modulatory effects of connexin 43 on cell death/survival beyond cell coupling. Prog Biophys Mol Biol 2007;94:219-32. Back to cited text no. 71 |
| 72. | Contreras JE, Sanchez HA, Veliz LP, Bukauskas FF, Bennett MV, Saez JC. Role of connexin-based gap junction channels and hemichannels in ischemia-induced cell death in nervous tissue. Brain Res Brain Res Rev 2004;47:290-303. Back to cited text no. 72 |
| 73. | Goubaeva F, Mikami M, Giardina S, Ding B, Abe J, Yang J. Cardiac mitochondrial connexin 43 regulates apoptosis. Biochem Biophys Res Commun 2007;352:97-103. Back to cited text no. 73 [PUBMED] [FULLTEXT] |
| 74. | Lin JH, Weigel H, Cotrina ML, Liu S, Bueno E, Hansen AZ, et al . Gap-junction-mediated propogation and amplification of cell injury. Nat Neurosci 1998;1:494-500. Back to cited text no. 74 |
| 75. | Katoh F, Klein JL, Bignami M, Yamasaki H. Association of viral oncogene-induced changes in gap junctional intercellular communication and morphological transformation in BALB/c3T3 cells. Carcinogenesis 1993;14:435-40. Back to cited text no. 75 [PUBMED] [FULLTEXT] |
| 76. | Huang RP, Hossain MZ, Huang R, Gano J, Fan Y, Boynton AL. Connexin 43 (cx43) enhances chemotherapy-induced apoptosis in human glioblastoma cells. Int J Cancer 2001;92:130-8. Back to cited text no. 76 [PUBMED] [FULLTEXT] |
| 77. | Rodriguez-Sinovas A, Cabestrero A, Lopez D, Torre I, Morente M, Abellan A, et al . The modulatory effects of connexin 43 on cell death/survival beyond cell coupling. Prog Biophys Mol Biol 2007;94:219-32. Back to cited text no. 77 |
| 78. | Hertzberg EL, Van Eldik LJ. Interaction of calmodulin and other calcium-modulated proteins with gap junctions. Met Enzymol 1987;139:445-54. Back to cited text no. 78 |
| 79. | Bevans CG, Harris AL. Regulation of connexin channels by pH: Direct action of the protonated form of taurine and otheraminosulfonates. J Biol Chem 1999;274:3711-9. Back to cited text no. 79 [PUBMED] [FULLTEXT] |
| 80. | Barrio LC, Suchyna T, Bargiello T, Xu LX, Roginski RS, Bennett MV, et al . Gap junctions formed by connexins 26 and 32 alone and in combination are differently affected by applied voltage. Proc Natl Acad Sci USA 1991;88:8410-4. Back to cited text no. 80 [PUBMED] [FULLTEXT] |
| 81. | Barrio LC, Capel J, Jarillo JA, Castro C, Revilla A. Species-specific voltage-gating properties of connexin-45 junctions expressed in Xenopus oocytes. Biophys J 1997;73:757-69. Back to cited text no. 81 [PUBMED] [FULLTEXT] |
| 82. | Herve JC, Sarrouilhe D. Modulation of junctional communication by phosphorylation: Protein phosphatases, the missing link in the chain. Biol Cell 2002;94:423-32. Back to cited text no. 82 |
| 83. | Lampe PD, TenBroek EM, Burt JM, Kurata WE, Johnson RG, Lau AF. Phosphorylation of connexin43 on serine368 by protein kinase C regulates gap junctional communication. J Cell Biol 2000;149:1503-12. Back to cited text no. 83 [PUBMED] [FULLTEXT] |
| 84. | Ogawa T, Hayashi T, Yorioka N, Kyoizumi S, Trosko JE. Hexamethylene bisacetamide protects peritoneal mesothelial cells from glucose. Kidney Int 2001;60:996-85. Back to cited text no. 84 [PUBMED] [FULLTEXT] |
| 85. | Yao J, Hiramatsu N, Zhu Y, Morioka T, Takeda M, Oite T, et al . Nitric oxide-mediated regulation of connexin43 expression and gap junctional intercellular communication in mesangial cells. J Am Soc Nephrol 2005;16:58-67. Back to cited text no. 85 [PUBMED] [FULLTEXT] |
| 86. | Shiokawa-Sawada M, Mano H, Hanada K, Kakudo S, Kameda T, Miyazawa K, et al . Down-regulation of gap junctional intercellular communication between osteoblastic MC3T3-E1 cells by basic fibroblast growth factor and a phorbol ester (12-O-tetradecanoylphorbol-13-acetate). J Bone Miner Res 1997;12:1165-73. Back to cited text no. 86 [PUBMED] |
| 87. | van Zoelen EJ, Tertoolen LG. Transforming growth factor-beta enhances the extent of intercellular communication between normal rat kidney cells. J Biol Chem 1991;266:12075-81. Back to cited text no. 87 [PUBMED] [FULLTEXT] |
| 88. | Lau AF, Kanemitsu MY, Kurata WE, Danesh S, Boynton AL. Epidermal growth factor disrupts gap-junctional communication and induces phosphorylation of connexin43 on serine. Mol Biol Cell 1992;3:865-74. Back to cited text no. 88 [PUBMED] [FULLTEXT] |
| 89. | Burt JM, Steele TD. Selective effect of PDGF on connexin43 versus connexin40 comprised gap junction channels. Cell Commun Adhes 2003;10:287-91. Back to cited text no. 89 [PUBMED] |
| 90. | Cushing P, Bhalla R, Johnson AM, Rushlow WJ, Meakin SO, Belliveau DJ. Nerve growth factor increases connexin43 phosphorylation and gap junctional intercellular communication. J Neurosci Res 2005;82:788-801. Back to cited text no. 90 [PUBMED] [FULLTEXT] |
| 91. | Turner MS, Haywood GA, Andreka P, You L, Martin PE, Evans WH, et al . Reversible connexin 43 dephosphorylation during hypoxia and reoxygenation is linked to cellular ATP levels. Circ Res 2004;95:726-33. Back to cited text no. 91 [PUBMED] [FULLTEXT] |
| 92. | Eugenin EA, Branes MC, Berman JW, Saez JC. TNF-alpha plus IFN-gamma induce connexin43 expression and formation of gap junctions between human monocytes/macrophages that enhance physiological responses. J Immunol 2003;170:1320-8. Back to cited text no. 92 |
| 93. | Oviedo-Orta E, Howard Evans W. Gap junctions and connexin-mediated communication in the immune system. Biochim Biophys Acta 2004;1662:102-12. Back to cited text no. 93 [PUBMED] [FULLTEXT] |
| 94. | Branes MC, Contreras JE, Saez JC. Activation of human polymorphonuclear cells induces formation of functional gap junctions and expression of connexins. Med Sci Monit 2002;8:BR313-23. Back to cited text no. 94 |
| 95. | Navab M, Liao F, Hough GP, Ross LA, Van Lenten BJ, Rajavashisth TB, et al . Interaction of monocytes with cocultures of human aortic wall cells involves interleukins 1 and 6 with marked increases in connexin43 message. J Clin Invest 1991;87:1763-72. Back to cited text no. 95 |
| 96. | Kwak BR, Veillard N, Pelli G, Mulhaupt F, James RW, Chanson M, et al . Reduced connexin43 expression inhibits atherosclerotic lesion formation in low-density lipoprotein receptor-deficient mice. Circulation 2003;107:1033-9. Back to cited text no. 96 [PUBMED] [FULLTEXT] |
Copyright 2009 - Journal of Postgraduate Medicine
The following images related to this document are available:
Photo images
[jp09040b2.jpg]
[jp09040b1.jpg]
[jp09040f1.jpg]
[jp09040f2.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}