 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
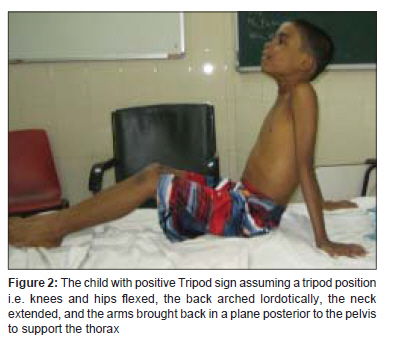
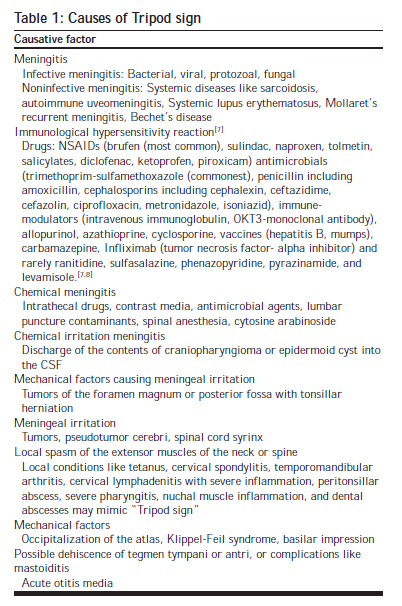
Journal of Postgraduate Medicine, Vol. 55, No. 3, July-September, 2009, pp. 211-213 Clinical Signs Tripod sign Suvarna JC, Keskar VS Department of Pediatrics, Seth GS Medical College and KEM Hospital, Parel, Mumbai - 400 012, India Date of Submission: 25-Feb-2008 Code Number: jp09065 PMID: 19884752 DOI: 10.4103/0022-3859.57408 Abstract "Tripod Sign" or "Amoss's Sign" is a sign of meningeal irritation. Although useful in diagnosing meningitis, it is not pathognomic and may be seen in a variety of clinical conditions. Infants < 1 year of age and immunocompromised individuals may not demonstrate signs of meningeal irritation. Since elicitation of the sign requires voluntary sitting up, it is of limited use in patients with marked altered sensorium and young infants.Keywords: Meningeal signs, meningeal irritation, Tripod sign, Amoss' sign, meningism, meningismus Tripod sign, also known as the "Amoss's sign," is a useful sign of meningeal irritation. It is used for diagnosing conditions like meningitis, subarachnoid hemorrhage, and poliomyelitis. Cerebral and meningeal inflammation were first described in detail by Willis (1685) and Morgagni (1761). [1] The Tripod sign, a sign of meningeal irritation, was first described by the American pathologist Harold Lindsay Amoss (1886-1956) from Kentucky, also known for his renowned work on infectious diseases including poliomyelitis, meningitis, erysipelas, brucellosis, encephalitis, and on vaccines for meningitis and poliomyelitis. [2] It is interesting to note that the word "tripod" is used in other clinical contexts as well. "Tripod position" is used to describe the classic position assumed by the patient with advanced lung disease or severe respiratory compromise, who is desperate for more air (e.g., chronic obstructive pulmonary disease). The patient leans forward resting his/her outstretched hands on the knees anterior to the frontal plane. This provides a position that optimizes and improves the mechanical advantage of the muscles moving the chest wall and the diaphragm. It may also ease the upper airway obstruction by moving the inflamed and swollen epiglottic structures forward. The classic picture of a toxic febrile child or an adult with a rapidly progressing clinical picture, stridor, sore throat, odynophagia and respiratory distress, sitting in a "tripod position," and drooling saliva, would suggest a diagnosis of acute epiglottitis, peritonsillar, or retropharyngeal abscess. It is a red flag indicating severe inflammation and impending upper airway obstruction and should be treated as a medical emergency and confirmed with the help of neck radiography and direct laryngoscopy. [3] The milestone of sitting with support, at about six months of age in a normal infant is often referred to as sitting in the tripod position (leaning forward on the hands) or tripod sitting. [4] The "tripod position" is also used to describe the position in which the patient stands when using crutches or begins walking with crutches. The term "Tripoding" is used to denote the use of three points of support, as adopted by paralyzed patients when changing from a sitting or standing position. [5] Elicitation of the 'Tripod' Sign The patient is asked to sit up in bed. This action requires active movement involving flexion of the neck. Although a normal patient sits up without supporting himself, a patient with meningeal irritation tries to sit up by supporting himself with his hands placed far behind him in the bed (like a tripod), in order to take the weight off the spine and prevent its flexion. Severe meningeal irritation may result in the patient assuming the tripod position with the knees and hips flexed, the back arched lordotically, the neck extended, and the arms brought back in a plane posterior to the pelvis to support the thorax [Figure - 1] and [Figure - 2]. This sign can be elicited only in patients who are old enough and conscious enough to sit up on their own. Causes and Genesis The genesis of the Tripod sign is best explained on the basis of mechanical factors. [6] The spinal canal is posterior to the vertebral bodies. When the spine is flexed, it lengthens, stretching its contents. [6] O'Connell (1946) in his study on cadavers has shown that the tension on the intradural nerve roots as well as extradural spinal nerves increases as the head is moved from full extension to flexion. [1] As the brainstem is relatively immobile, the cord gets pulled upward when it is stretched. The stretch is felt maximally at the lower structures, viz. the femoral and sciatic nerves along the cauda equina. In patients with meningeal inflammation and irritation, this stretch of the inflamed structures due to spine flexion leads to the stimulation of the afferent nerve roots and intraspinal reflex centers, causing tonic motor impulse to the posterior axial musculature. This results in a protective reflex spasm in the extensor muscles of the spine to prevent its active flexion. [1] In addition, Brain (1962) stated that the flexion of the neck increases the cerebrospinal fluid (CSF) pressure in the cisterna magna. In the setting of meningeal irritation and inflammation, this results in an increased pressure on the inflamed meninges, which is prevented by reflex extensor rigidity. [1] Thus, maneuvers that stretch the inflamed neural elements and meninges of the spinal canal (like neck flexion, trunk flexion while sitting up) lead to postures which minimize tension on the inflamed structures. These phenomena characterize all meningeal signs like Tripod sign, neck stiffness, Kernig's sign, and Brudzinski's sign. In Tripod sign, on attempting to sit up, the patient adopts the tripod posture with back and neck extended (to prevent flexion of the spine) with hips and knee flexed. [6] Hip flexion relaxes the femoral nerve and although it stretches the sciatic nerve, the knee flexion relaxes it. Thus, both these nerves are maximally relaxed by keeping the hips and knees in intermediate flexion. [6] The Tripod sign may be seen as a part of the clinical profile of meningism or meningismus. Meningism is when signs of meningeal irritation are seen and are due to the infection or inflammation of the meninges whereas meningismus is when these signs are seen even in the absence of infection or inflammation of the meninges. The illnesses most frequently mentioned in association with meningismus are pneumonias, streptococcal sore throat, pyelonephritis, sinusitis, influenza, typhoid fever, typhus fever, and measles. [1] It has been attributed to the disturbance in the osmotic relationship between the blood and the CSF. [1] Hemodilution is said to occur at the onset of acute infectious processes resulting in blood hypotonicity compared to the CSF. A shift of the extracellular fluid from blood to the CSF occurs via the choroid plexus. This coupled with delay in the reabsorption of the CSF leads to an increase in the CSF pressure and leads to signs of meningeal irritation. [1] [Table - 1] enlists the various causes of Tripod sign.
Tripod sign is a characteristic feature in preparalytic and paralytic poliomyelitis (Heine-Medin disease). It causes muscle tenderness, weakness, and spasm in the extensors of the neck and back, and sometimes the hamstring and other muscles. This gives the characteristic Hoyne's sign or head lag (when shoulders are elevated in a supine patient, head will lag). Other Methods for Elicitation of Meningeal Irritation Neck stiffness (nuchal rigidity/rigor nuchalis) is tested by gentle forward flexion of the neck with the patient lying in the supine position. Kernig's sign, described by the Russian physician Vladimir Mikhailovich Kernig in 1884, is elicited with the patient lying supine, one hip flexed at 90° and the other leg remaining in the neutral position on the bed. A positive sign is present when extension of the knee from this position elicits resistance or pain in the lower back or posterior thigh. Brudzinski's neck sign, described by the Polish physician Josef Brudzinski in 1909 is elicited in a supine position. Passive neck flexion or turning it to one side results in flexion of the knees and hips. In Brudzinski's leg sign, passive flexion of one hip and knee causes flexion of the contralateral leg. Meningeal irritation can also be tested by the jolt accentuation of headache which is tested by asking the patient to turn his or her head horizontally at a frequency of two to three rotations per second. Worsening of a baseline headache represents a positive sign. Clinical Approach A high index of suspicion for meningitis should be entertained if the patient has history of fever, headache, vomiting, photophobia, meningeal signs, focal neurological signs, seizures, and altered sensorium. A search for the etiology can be made with the help of CSF studies (cytology, proteins, culture, polymerase chain reaction for certain viruses, lactate levels, etc.). Associated clinical features like rash (e.g., varicella rash, genital lesions in herpes, enterovirus rash), herpangina in coxsackie virus infection, parotid swelling in mumps, petechiae in meningococcemia, history of Koch's contact, handling animals (brucellosis), or dog-bite (rabies) are important pointers to the diagnosis. A history of sudden-onset headache with meningeal signs, altered sensorium, and focal neurological signs would suggest a subarachnoid hemorrhage. Local causes and other causes of meningismus may need to be looked for and ruled out. An acute/chronic complicated otitis media should be looked for. Fundus examination (to rule out papilledema, subhyaloid hemorrhage, or pseudotumor cerebri) and imaging to rule out posterior fossa tumor may be required. Importance of Tripod Sign Although signs of meningeal irritation are highly indicative of meningitis, they are not pathognomonic. Bacterial meningitis may contribute to 30% of the cases with meningeal signs, viral/aseptic meningitis 13%, pneumonia 8%, other serious bacterial infections 2%, and upper respiratory infections and other self-limiting diseases to 46% of the cases. [10] "Tripod sign" and "neck stiffness" as clinical signs of meningeal irritation have been evaluated to be as good as the so-called specific tests for demonstrating meningeal irritation, i.e., Kernig's and Brudzinski's signs. [10] Since infants below one year may not display classical signs of meningeal irritation, irritability, lethargy, and bulging fontanel may be important markers for meningitis in them. [10] Immunosuppressed individuals may not manifest signs of meningeal irritation and a high degree of suspicion should be entertained in these patients. [11] Tripod can be used only in clinical conditions where patients can voluntarily sit up. Therefore, it is not of use in small infants, and where the patient is not compliant due to marked altered sensorium. References
Copyright 2009 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp09065f2.jpg] [jp09065f1.jpg] [jp09065t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}