 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
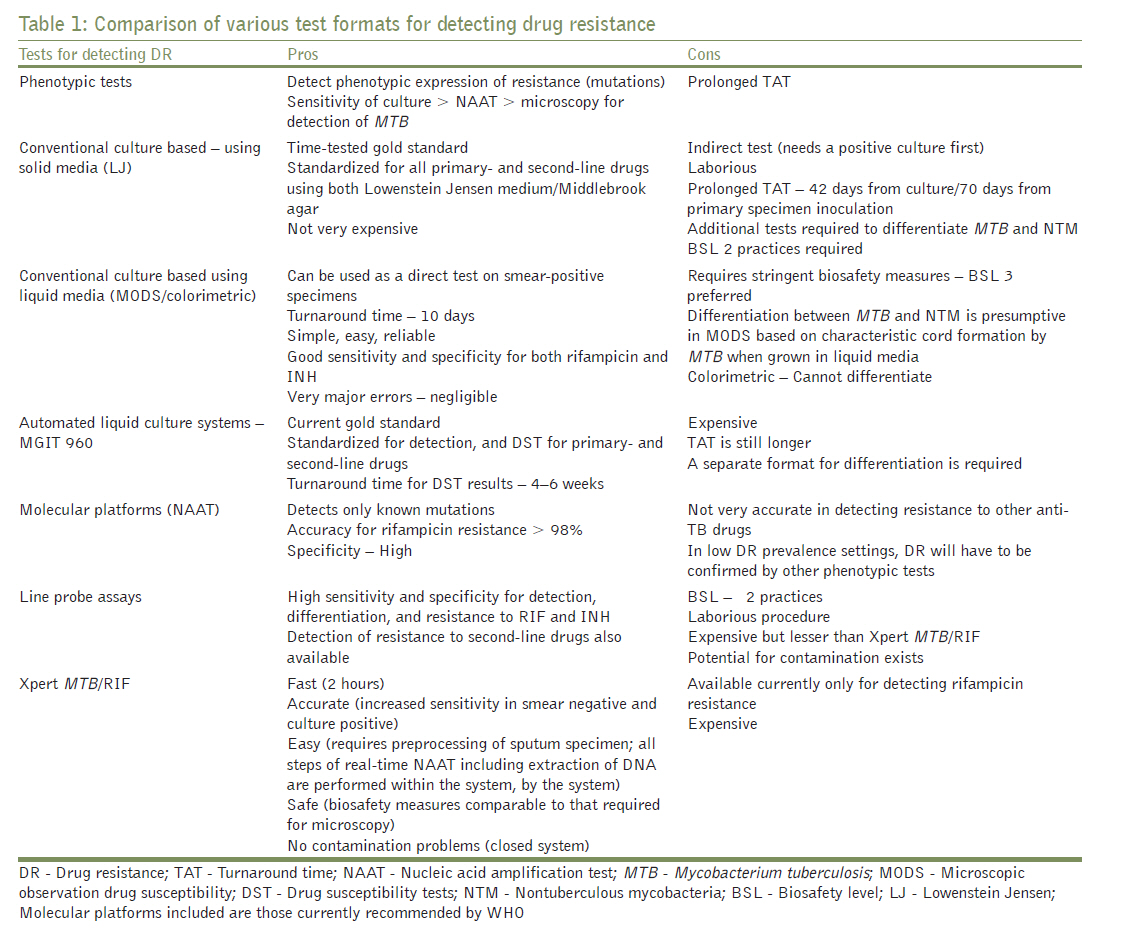
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 267-269 Editorial Newer diagnostics for detection of multidrug-resistant tuberculosis G Nataraj Department of Microbiology, Seth G. S. Medical College and K. E. M. Hospital, Parel, Mumbai, India Drug-resistant TB is a laboratory diagnosis. However, very few diagnostic laboratories perform susceptibility testing for tubercle bacilli. Important reasons for this include the labor-intensive nature of the conventional identification and drug susceptibility tests (DST), the prolonged turnaround time, the lack of adequate quality assurance programs and the need to follow stringent biosafety measures with reference to equipment, practices and ventilation. The phenotypic culture-based methods (indirect susceptibility testing) detect the ability of the clinical isolate to grow in the presence of drug/s and until recently were considered the gold standard. These tests are accurate and inexpensive and can be used for determining susceptibility to both first- and second-line anti-TB drugs. Amongst the various methods available, 1% proportion method was recommended. [3] The high turnaround time of tests employing solid media prompted the development of semi-automated (BACTEC 460TB) and automated (MGIT 960, MBBacT, Versatrek) liquid culture systems capable of rapid detection and DST in half the time. DST using MGIT 960 has been standardized for all primary-line drugs and most second-line drugs. This is the only rapid culture system currently endorsed by WHO for drug resistance surveillance. [4] The automated systems, however, require the use of expensive equipment and reagents, thus increasing the cost per test. Since culture-based systems (both solid and liquid) have been standardized to detect not only the resistance status but also the drugs to which the isolate is susceptible to, in vitro, they provide useful inputs to the clinician for deciding choice of therapy on an individual basis. To further overcome the turnaround time and reduce the cost per test, direct drug susceptibility assays using liquid media on smear-positive specimens with the incorporation of more sensitive methods of growth detection were developed. The most promising amongst these are (i) the microscopic observation drug susceptibility (MODS) assay which relies on microscopic (inverted microscope) demonstration of the characteristic cord-like growth of MTB in liquid media even in the presence of drugs; [5] (ii) the colorimetric tests which rely on the change in color on addition of an oxidation reduction indicator to the drug containing tubes in which mycobacteria continue to grow; [6] and (iii) the nitrate reductase assay. [7] These tests are simple and reliable and can be performed by any mycobacteriology laboratory that is equipped for culture. With the performance characteristics for rifampicin and isoniazid (INH) being excellent, they are primarily recommended for determining the MDR status. [6] Formats for the other anti-TB drugs have either not worked or have not been looked into. Genotypic tests are nucleic acid amplification tests that detect known resistance conferring mutations on the genes that facilitate drug action. Molecular platforms today provide information on presence of MTB and drug resistance in the same assay. Mutations for some anti-TB drugs are well characterized. These include mutations in rpoB gene for rifampicin, inh A and katG gene for INH, and gyr gene for fluoroquinolones. Detecting rifampicin resistance using genotypic methods is useful for two reasons. First, more than 95% of the resistance mutations are present on an 81 bp region of the rpoB gene. Second, rifampicin resistance is considered as a surrogate marker for MDRTB. Resistance to other anti-TB drugs is more complex and requires detection of mutations in multiple genes for good correlation. [8] The most specific amongst the genotypic tests would be sequencing of the complete nucleotide sequence of the amplified target DNA. This is not carried out routinely. Instead, line probe assays (reverse hybridization assays) have recently been recommended by WHO for DST. INNO-LiPA Rif.TB® (Innogenetics, Ghent, Belgium) and GenoType® MTBDRplus kit (Hain Lifescience, Nehren, Germany) are the widely recommended test formats. [9] Each test strip has multiple probes for mutant (resistant) and wild-type (susceptible) strains. These tests have excellent specificity and sensitivity, especially in smear-positive patients, and the results are available on the same day or within 48 hours. They require expensive equipment, reagents, expertise and biosafety measures and are currently recommended only for smear-positive specimens though studies have demonstrated their utility even in smear-negative patients. [10] The most promising and exciting molecular platform for detecting MTB and rifampicin resistance in recent times is Xpert® MTB/Rif (Cepheid, California, USA), a nucleic acid amplification test (NAAT) using a real-time format for M. tuberculosis detection and MDRTB screening. [10] It is fast, accurate, easy and safe to operate with minimal biohazard component, but is expensive. Other than sputum processing (decontamination and digestion), all other steps which include extraction, amplification and detection are automated within the machine, thereby reducing cross contamination, a problem often faced by molecular diagnostic laboratories. No expertise is thus required, and on the same day results can be obtained. It appears to be the most field-friendly of all the tests currently available, with very high sensitivity and specificity, and is currently recommended by WHO in settings with high MDRTB burden. [11] In low prevalence settings, drug resistance data generated by molecular platforms would need a conventional backup. By providing a same day diagnosis and data on resistance to some of the more important anti-TB drugs, molecular platforms provide useful inputs to clinical decision making. Culture and DST may still be required to decide the choice of therapy, especially in XDRTB cases. [Table - 1] shows a comparison of the different test formats for detecting drug resistance. Molecular platforms included are those currently recommended by WHO. Drug-resistant TB is a problem that needs to be addressed on a war footing, especially in settings with high burden or high resistance rates such as in patients attending tertiary care hospitals. Screening for drug resistance is woefully inadequate. Currently, under the Revised National Tuberculosis Control Programme (RNTCP), DST is recommended for those who experience treatment failure after 5 months of treatment. [12] The delayed diagnosis is a detriment both to the patient as well as for preventing transmission. One case detected and treated early can potentially prevent further 15-20 persons from getting DRTB annually. Also, only a few laboratories have been accredited for carrying out DST. A wider capacity building is the need of the day and this should include major referral hospitals and medical colleges. Capacity building for DRTB detection should go hand in hand with upscaling provision for MDRTB treatment. If the limited rolling out of accredited laboratories has been due to constraints of biosafety, this can be easily overcome with systems like GeneXpert or similar platforms, even if they are initially costlier. Smear microscopy will continue to be the initial test for detection of TB in resource-constrained settings. But where the possibility of MDRTB/XDRTB is high, efforts to detect MTB and its resistance should be made at the outset itself, using a combination of a molecular platform and the conventional culture-based platform such as MGIT 960, which provides information on choice of drug for therapy and would also confirm resistance. These tests are available in India in some major laboratories, but are expensive. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11079t1.jpg] |
| |||||||||

{kind=link}