 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 278-285 Original Article Evaluation of eperisone hydrochloride in the treatment of acute musculoskeletal spasm associated with low back pain: A randomized, double-blind, placebo-controlled trial AS Chandanwale1, A Chopra2, A Goregaonkar3, B Medhi4, V Shah5, S Gaikwad4, DG Langade6, S Maroli7, SC Mehta8, A Naikwadi9, DR Pawar8 1 Department of Orthopedics, Grant Medical College and Sir J. J. Group of Hospitals, Mumbai, India Date of Submission: 11-Mar-2011 Code Number: jp11082 PMID: 22120855 Abstract Background : Eperisone hydrochloride is a centrally acting muscle relaxant inhibiting the pain reflex pathway, having a vasodilator effect. Keywords: Eperisone, low back pain, musculoskeletal spasm Introduction Low back pain is a major health and socioeconomic problem [1] and is associated with high costs of healthcare, work absenteeism and disablement. [2] It is associated with higher age, physical fitness, muscle strength [3] and psychosocial factors. [4] There is a vicious cycle of spasm-pain-spasm [5] and observations from clinical practice support the need to eliminate spasm to improve functionality. [6],[7] Eperisone hydrochloride is a centrally acting muscle relaxant acting through poly and mono-synaptic reflexes in the spinal cord, exhibits vasodilator effect, increases blood flow and inhibits the pain reflex pathway. [8] An oral dose of 150 mg/day in three divided doses has been shown to be effective for treatment of various myotonic conditions. [8] The objective of the study was to compare the efficacy and tolerability of eperisone hydrochloride versus placebo in the treatment of patients with acute musculoskeletal spasm (AMSP) associated with low back pain (LBP). Materials and Methods Trial design This was a prospective, randomized, double-blind, placebo-controlled, multi-centric Phase III study conducted at five tertiary care orthopedic centers across India. A prior written approval for conducting the study was obtained from the Indian drug regulatory authorities and the institutional ethics committees of the respective centers. Ethical Committee notifications as per Good Clinical Practice Guidelines (GCP) issued by the Central Drugs Standard Control Organization (CDSCO) of India and ethical guidelines for biomedical research on human subjects, issued by the Indian Council of Medical Research (ICMR) were followed during the conduct of the study. Participants Patients of either sex between 18 and 60 years of age attending the outpatient setting of the orthopedic departments of the study centers were screened for lumbar pain and spasm by clinical and radiological examination, for inclusion. It was planned to enroll 240 patients with confirmed diagnosis of acute musculoskeletal spasm with low back pain due to spondylosis deformans, prolapsed disc or muscle sprain. Those willing to comply with study procedures were included after obtaining written informed consent. Laboratory evaluations were done at baseline to rule out any laboratory abnormalities for hemogram, complete blood count, renal function test (serum creatinine and blood urea nitrogen), hepatic function tests (total serum bilirubin, alkaline phosphatase, aspartate transaminase and alanine transaminase), and random blood sugar. Patients with other associated unrelated spasm conditions like muscle sprains with spasms of hip or knee or ankle, traumatic pain with spasms, cervical spondylitis and pain and spasm associated with fractured bone were excluded. Also, those who had received an investigational new drug in the preceding four weeks or any form of muscle relaxants in the previous seven days, with known hypersensitivity to any of the ingredients of the test and control formulations, pregnant and lactating females, women of childbearing potential not practicing adequate contraceptive measures, and patients unwilling or unable to comply with study procedures were excluded. Patients with history of severe infection, major surgery or trauma, severe metabolic, endocrine or electrolyte disturbances, seizure during the preceding eight weeks, severe renal or hepatic insufficiency, uncontrolled diabetes mellitus, any other metabolic/endocrine disorder, and severe cardiac dysfunction were also not enrolled. Interventions Enrolled patients received either tablets containing either eperisone hydrochloride (50 mg), or identical placebo tablet. Both eperisone and placebo were identical in appearance (size and shape) and were self-administered by the patient thrice daily orally for 14 days. Patients were instructed to use rescue medication (acetaminophen 500 mg) when there was no pain relief after the administration of the study medication. Use of any skeletal muscle relaxant other than study medications, neuromuscular blocking agents, cholinergic drugs and cortiosteroids was not permitted during the study period. Outcomes The efficacy parameters assessed included finger-to-floor-surface distance (FFD) measured as distance in mm when standing with the spinal cord flexed with complete extension of knee joint, [9] Lasegue sign (lumbar pain or exacerbation of existing pain on passive movement of the legs during flexion of hip joint), lumbar and dorsal hypermyotonia (assessed on a four-point scale of 0=Absent or Normal, 1=Mild hypertonia, 2=Moderate hypertonia, and 3=Marked hypertonia), tenderness of paravertebral muscles, need for rescue medication (assessed as number of rescue tablets administered by the patient), and leg tendon reflexes (evaluated as present or absent). The subjective efficacy parameters assessed were lumbar cinesalgia (assessed on a 0-100 mm Visual Analogue Scale (VAS) with ′0′ representing ′No Pain′ and ′100′ representing ′SEVERE intolerable pain′), sensory disturbances of lower limb (assessed as present or absent), pain in lower extremities (assessed on a four-point rating scale of 0=No Pain, 1=Mild Pain, 2=Moderate Pain and 3=Severe Pain), and Global Assessment of Response to Therapy (GART) assessed on a four-point scale of Excellent, Good, Average and Poor. Safety parameters included the adverse events reported by the patients and Global Assessment of Tolerability to Therapy (GATT) assessed on a four-point scale of Excellent, Good, Average and Poor. All clinical assessments were made at baseline visit (Day 1), and then on Day 3, Day 7 and Day 14. There were no changes in the study outcomes during the course of the study. Sample size Sample size estimation was based on the reduction in the FFD from baseline after five days of therapy. The method of testing was ′t′ test (matched treatment groups) with superiority hypothesis of eperisone over placebo. Superiority was defined as a reduction in the mean FFD from baseline by at least >20% compared to the reduction with placebo. With an observed reduction in mean FFD of 14.0, the calculated standardized effect size was 0.4429 at alpha 0.05 and 90% power. [10] A total of 178 completed patients were required to detect a 20% difference between placebo and eperisone in the change in FFD from baseline on Day 5. Considering dropouts and loss to follow-up it was planned to enroll 240 patients (i.e. 120 per treatment arm). Randomization Enrolled subjects were assigned a four-digit Subject Identifier number used to identify each subject during the study. Randomization was done in a 1:1 ratio with a predetermined site-specific computer-generated randomization schedule using Windows-based program Rando Version 1.0. Serially numbered sealed envelopes based on the randomization codes (containing study medication) were given at the sites, which were issued to the patients by a clinician or nurse only after verification of the eligibility criteria, enrolment in the study and assigning the serial number. Envelopes were required to be opened by the patient only after enrolment. Clinician who did the clinical evaluation as well as patients were blinded to the intervention. The packaging and labeling of the medication packs was designed to ensure blinding of the study treatments. Statistical methods Data from all the centers were pooled for analysis. Efficacy analysis was done for per-protocol (PP) population and safety analysis was done for intention-to-treat (ITT) population. Parametric data is expressed as means with standard deviation and discrete data is expressed as numbers with proportions. Two groups were compared for differences in mean values for FFD and lumbar pain by ′t′ test, whereas within treatment change in these parameters was analyzed by one-way ANOVA with time as factor. Between-groups comparisons for hypermyotonia, tendon reflexes, and pain in lower extremities were analyzed using Mann-Whitney ′U′ test (non-parametric), whereas within treatment change in these parameters was analyzed using Kruskall-Wallis (non-parametric) test. Proportions (tenderness, tingling, numbness, paresthesia and need for rescue medication) were compared using Fischer′s (Chi-square) test. For all statistical tests, the significance level was P<0.05.
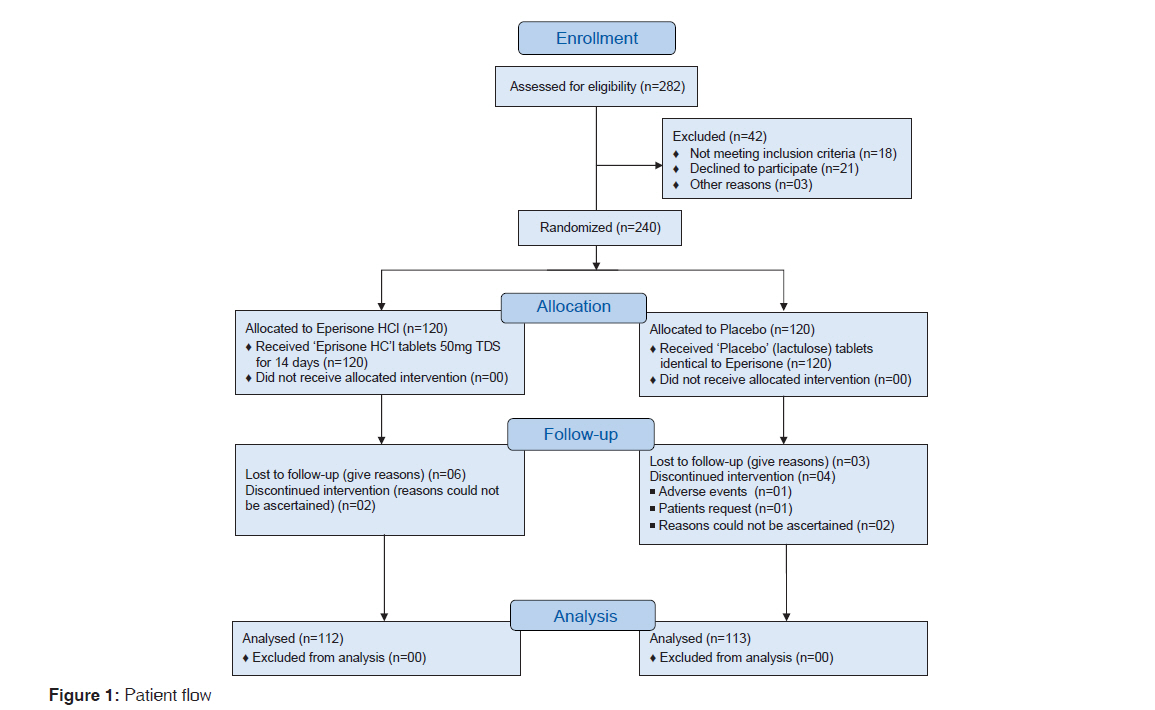
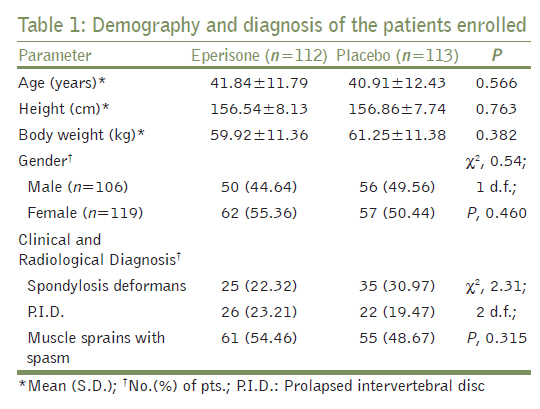
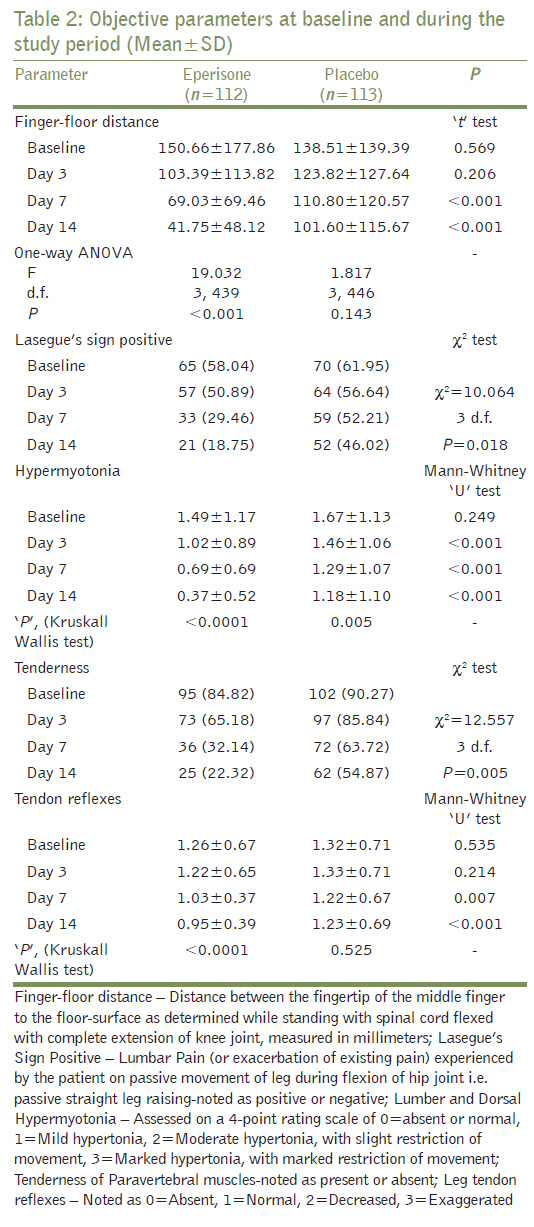
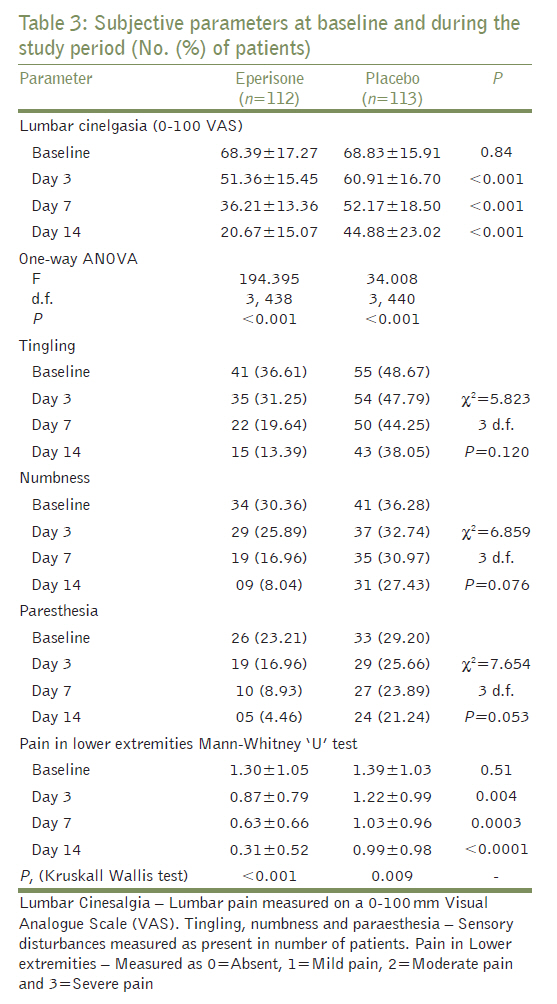
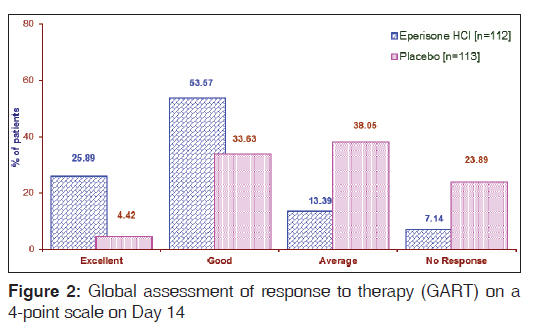
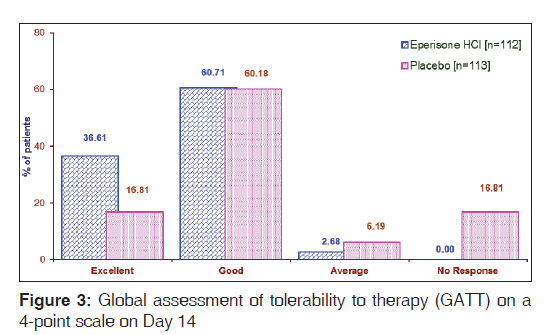
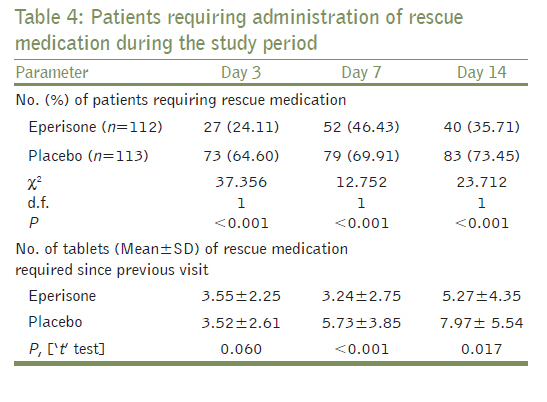
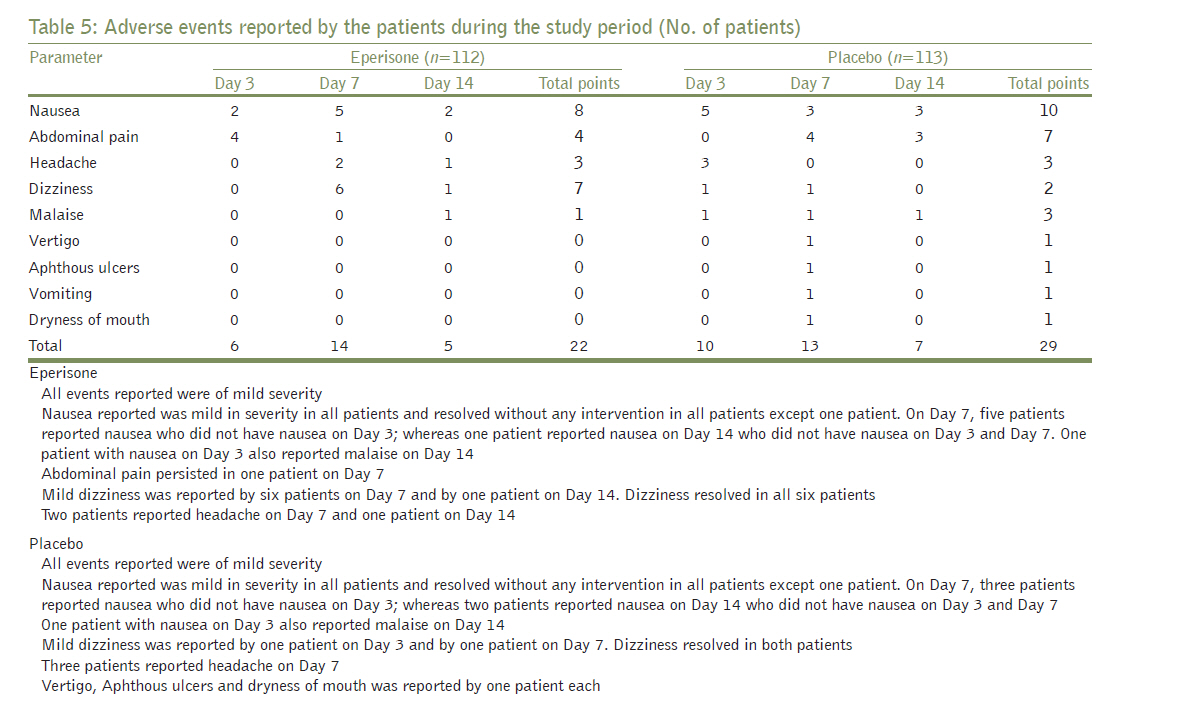
Two hundred and forty patients with confirmed diagnosis of AMSP with low back pain satisfying the inclusion criteria were enrolled from April 2006 to June 2006 after obtaining written informed consent and were randomized to receive eperisone (n=120) and placebo (n=120). [Figure - 1] shows the disposition of the patients. There were 15 dropouts, eight in the eperisone group (five males and three females) and seven in the placebo group (four males and three females). A total of 225 patients (106 males, 119 females) completed the study and were available for ITT analysis. Thus, the final ITT population included 112 patients on eperisone and 113 patients on placebo. With eperisone, six were lost to follow-up, in two cases the reasons were not specified. Of the seven drop-outs in the placebo group, three were lost to follow-up, two withdrew, one due to an adverse event of urticaria and other due to unwillingness to continue, and in two cases the reasons were not specified. For safety analysis, data of all the patients enrolled was included (PP population). [Table - 1] shows the demography and diagnosis of the enrolled patients. The two groups were comparable with respect to the demography and baseline values of parameters (P>0.05). The laboratory values at baseline and at the end of the study were within normal limits for both treatments. Objective efficacy parameters [Table - 2] shows the objective efficacy parameters at baseline and during the study period. There was a 72.53% reduction with eperisone (P<0.001) and 21.62% with placebo (P=0.143) in FFD from baseline on Day 14, at Visit 2 compared to baseline (P=0.0002). Similarly, 75.23% improvement from baseline score for lumbar and dorsal hypermyotonia was seen with eperisone on Day 14, whereas with placebo the improvement was only 29.51%, the difference between the two groups being significant (P<0.001). Improvement in Lasegue′s sign was seen in 44 (39.29%) patients with eperisone and in only 18 (15.93%) patients on placebo on Day 14, the difference between the two groups being significant (P<0.002). Similarly, the improvement in tenderness of paravertebral muscles was seen in 70 (62.50%) patients with eperisone on Day 14, improvement with placebo was seen only in 40 (35.4%) patients on Day 14, the difference between the two groups being significant (P<0.001). There was a 24.29% improvement in mean score for leg tendon reflexes in eperisone-treated patients on Day 14 as against 6.71% improvement with placebo, the difference between the two groups being significant (P<0.001). Subjective efficacy parameters The values for subjective parameters at baseline and during the follow-up are reported in [Table - 3]. There was a 68.88% reduction from baseline in the VAS score for lumbar pain on Day 14 with eperisone whereas with placebo the reduction was only 33.47%, the difference between the two groups being significant (P<0.001). Improvement in the sensory disturbances was greater with eperisone compared to placebo on Day 14; however it failed to reach statistical significance. Reduction in percentage of patients with paraesthesia was 18.75% with eperisone compared to 7.96% with placebo (P=0.018) on Day 14. Global assessment [Figure - 2] shows the global assessment of response to therapy (GART) and [Figure - 3] shows the global assessment of tolerability to therapy (GATT) on Day 14. Eperisone showed a better GART and GATT profile compared to placebo throughout the study period (P<0.001). The therapy was well tolerated in both the treatment groups. Rescue medication Rescue medication was needed by 27 (24.11%) and 73 (64.60%) patients on eperisone and placebo respectively on Day 3; whereas on Day 7, 52 (46.43%) and 79 (69.91%) patients on eperisone and placebo respectively needed rescue medication [Table - 4]. On Day 14, 40 (35.71%) patients on eperisone and 83 (73.45%) patients on placebo needed rescue analgesic. Thus, eperisone was superior compared to placebo (P<0.001). Mean number of tablets required by patients on eperisone was 5.27 tablets compared to 7.97 with placebo (P=0.017). Adverse events [Table - 5] shows the adverse events reported by the patients during the study period. All the adverse events in the eperisone and placebo-treated patients were mild to moderate in severity. Nausea (8 with eperisone and 10 with placebo) and abdominal pain (four with eperisone and seven with placebo) were the most common adverse events reported. With eperisone, nausea was mild in severity in all patients and resolved without any intervention in all patients except one patient. On Day 7, five patients reported nausea who did not have nausea on Day 3; whereas one patient reported nausea on Day 14 who did not have nausea on Day 3 and Day 7. One patient with nausea on Day 3 also reported malaise on Day 14. With placebo, nausea reported was mild in severity in all patients and resolved without any intervention in all patients except one patient. On Day 7, three patients reported nausea who did not have nausea on Day 3; whereas two patients reported nausea on Day 14 who did not have nausea on Day 3 and Day 7. One patient with nausea on Day 3 also reported malaise on Day 14. Abdominal pain persisted in one patient on Day 7 with eperisone. Among the patients who were dropouts in the eperisone group one patient experienced nausea which was however mild in intensity, not requiring dose modification or withdrawal of study medication. Among the patients who were dropouts in the placebo group one patient experienced mild ecchymosis not requiring any dose modification of the study medication. One patient experienced mild urticaria and he then withdrew from the study. The said adverse event in this patient resolved on stopping of study medication. Discussion This study compared the efficacy and tolerability of eperisone hydrochloride versus placebo in the treatment of patients with low back pain caused by acute musculoskeletal spasm. Lumbar pain and other subjective parameters like tingling, numbness, paresthesia, and tenderness were used as variables in the study and hence, the study was designed with a placebo control rather than a standard control to eliminate the bias due to placebo effect. However, there was a provision of rescue analgesics as and when needed to avoid any suffering to the patient. Low back pain may be attributed to various degenerative changes of the vertebrae, strain on the dorsolumbar muscles, poor posture, herniated lumbar intervertebral disc, spondylosis deformans, and muscle sprains with spasms. [9] Lumbar and dorsal hypermyotonia is observed in most of these diseases. Symptoms such as pain and stiffness associated with lumbago are caused by fatigue and poor posture. There is strong evidence that muscle relaxants relieve spasm and break the spasm-pain-spasm cycle significantly more than placebo, however side-effects like drowsiness and gastric irritation limit the use of these useful agents. [11],[12],[13] A systematic review of randomized and/or double-blinded controlled trials of muscle relaxants in the management of non-specific low back pain, has shown that there is strong evidence that these drugs are more effective than placebo in short-term pain relief. The pooled relative risk for nonbenzodiazepines vs. placebo after two to four days was 0.80 (95% CI: 0.71 to 0.89) for pain relief and 0.49 (95% CI: 0.25 to 0.95) for global efficacy. However, adverse events with a relative risk of 1.50 (95% CI: 1.14 to 1.98) were significantly more prevalent in patients receiving muscle relaxants (mostly, benzodiazepines), and especially the central nervous system (CNS) adverse effects (relative risk 2.04; 95% CI: 1.23 to 3.37). Thus, muscle relaxants are effective in the management of non-specific low back pain, but compounds with no effect on the CNS would be welcome. [14] FFD is considered to be an index of mobility of the spinal cord. As a result of paravertebral muscle spasm the flexion of the vertebral column is restricted. [15] There was significant improvement in the FFD, hypermyotonia, Lasegue′s sign positive, tenderness of paravertebral muscles and leg tendon reflexes with eperisone. In the present study eperisone also demonstrated significant efficacy on subjective parameters like lumbar cinesalgia, paraesthesia and pain in the lower extremities but not on tingling and numbness. Eperisone administration has shown to cause prompt reduction in FFD, both spontaneous and provoked pain, and rigidity in an open study. [16] In this study only four (4%) patients reported minor gastrointestinal adverse events. These findings are consistent with the study reported by Hanai et al., [9] where 30 outpatients with lumbago were treated with eperisone hydrochloride for four weeks in a dose of 150 mg/day in three divided doses. The patients showed a significant improvement in lumbar and dorsal hypermyotonia, Lasegue′s sign positive, tenderness of paravertebral muscles and reduction in FFD. However, unlike the present study there was no improvement in leg tendon reflexes. A randomized, double-blind, clinical trial in patients with cervical spondylosis showed that eperisone had a beneficial activity on pain in the arms and shoulders, stiffness, and other symptoms related to cervical spondylosis. [17] Eperisone (n=40) has been compared with baclofen (n=40) in a double-blind, randomized study in patients with spastic palsy for a period of six weeks. [18] Both drugs reduced muscular tone from Week 2 whereas only eperisone improved the joint range of motion (−32.5%, P<0.01 vs. −14.6%, P=NS). For tolerability, no differences were observed between eperisone and baclofen in any parameters and eperisone was judged as "good" by a higher number of physicians and patients than baclofen. Eighteen adverse events (15 patients), most of mild intensity, were reported with eperisone. These included asthenia, hyposthenia of lower limbs and sleepiness. In contrast, none of the patients in the present study reported sleepiness or sedation. In another double-blind comparative study versus thiocolchicoside, eperisone showed comparable analgesic and muscle relaxant efficacy. [19] Spontaneous pain and pain on movement/pressure were significantly reduced by both treatments. Clinically evident muscle relaxation was observed in the form of a progressive reduction in the "finger-to-floor" distance and improvement in Lasegue′s sign. The incidence of adverse events was only 5% with eperisone in this study. However, in our study the incidence of adverse events was 25.6% (29/113) with abdominal pain (10) and nausea (7) being the most common events. The differences in the incidence could not be explained and further exploratory studies are needed. Eperisone inhibits the spinal reflex pathway and causes vasodilatation resulting in increased blood flow leading to inhibition of pain reflex pathway. [8] This helps in reducing the intensity of pain with eperisone and possibly contributes to its analgesic activity. Sakai et al., (2008) have reported the improvement in intramuscular oxygenation and increased paraspinal muscle blood flow after oral administration of the eperisone hydrochloride during lumbar extension and flexion in patients with chronic LBP during four weeks of therapy. [20] In the present study, a significantly less number of patients required rescue medication in the eperisone group compared to the placebo group throughout the study period demonstrating the intrinsic analgesic activity of eperisone. The average consumption of rescue medication was significantly higher in the placebo group in the present study as compared to eperisone, which could possibly explain the slightly more number of patients in the placebo group (29 patients) experiencing adverse events as compared to patients receiving eperisone (22 patients). It is noteworthy that the analgesic and muscle relaxant effects were achieved with eperisone monotherapy, although it is a common practice in rheumatology to combine an analgesic with a muscle relaxant. The double-blind randomized, placebo-controlled design of the study was the main strength of the study. However, we did not evaluate the patients of musculoskeletal spasm in conditions other than low back pain. Also, a small sample size limits the generalization of these observations. Both, eperisone and placebo were well tolerated and common adverse events noted with eperisone were nausea, abdominal pain, headache and dizziness. The profile of adverse events with eperisone was more than the incidence reported in the post-marketing surveillance study of eperisone hydrochloride in Japan (unpublished observations), [21] in which the common adverse events reported were nausea, vomiting, gastrointestinal discomfort, anorexia, insomnia and somnolence. This study clearly demonstrates eperisone hydrochloride to be an effective and well-tolerated option in the treatment of patients with acute musculoskeletal spasm associated with low back pain, with an added advantage of intrinsic analgesic activity. However, these findings may not be generalized to the patient population and studies are needed in different etiologies of muscular spasm to substantiate the efficacy of eperisone hydrochloride in muscular spasm. Acknowledgment The authors would like to thank Eisai Pharmaceuticals India Pvt. Ltd. for their support. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11082t2.jpg] [jp11082t4.jpg] [jp11082f3.jpg] [jp11082f2.jpg] [jp11082f1.jpg] [jp11082t1.jpg] [jp11082t3.jpg] [jp11082t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}