 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 286-290 Original Article Clinical characteristics and outcomes of patients with acute lung injury and ARDS RR Bhadade1, RA de Souza1, MJ Harde2, A Khot1 1 Department of Medicine, Topiwala National Medical College and B.Y.L. Nair CH. Hospital, Mumbai Central, Mumbai, Maharashtra, India Date of Submission: 21-Jan-2011 Code Number: jp11083 PMID: 22120856 Abstract Background : Acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) are critical illnesses associated with significant morbidity and mortality. Keywords: Acute lung injury, lung injury score, mechanical ventilation, multiorgan failure Introduction As per American-European Consensus Conference (AECC), acute lung injury (ALI) is a clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure, a ratio of arterial oxygen tension to fraction of inspired oxygen (PaO 2 /FiO 2 ) of 201-300 mmHg, in the absence of cardiac failure. [1] Whereas acute respiratory distress syndrome (ARDS) is progression of the ALI, resulting from diffuse lung injury, which may be direct or indirect, and is characterized by an immunologic reaction leading to a diffuse alveolar damage, intense arterial hypoxemia, radiographic evidence of pulmonary edema and stiff and noncompliant lungs, a ratio of arterial oxygen tension to fraction of inspired oxygen (PaO 2 /FiO 2 ) of <200 mmHg, in the absence of congestive cardiac failure. [1],[2],[3] Various criteria used for the diagnosis ARDS/ALI in critically ill patients are: PaO 2 /FiO 2 as per AECC, lung injury score (LIS), etc. [1],[3],[4] Despite recent advances in mechanical ventilation and numerous clinical trials of novel pharmacological agents, understanding of pathophysiology of the disease; the mortality of ARDS remains very high ranging from 40% to 60%. ALI/ARDS results from direct (e.g. pneumonia, aspiration of gastric contents, pulmonary contusion, etc.) and indirect causes (e.g. sepsis, trauma, fractures, pancreatitis, burns, etc.). [5] Although above factors are potential causes of ARDS, studies showing tropical causes as reasons of ARDS is lacking. Hence, we attempted to study medical causes of ALI/ARDS in a tropical country. Recent reductions in ARDS/ALI mortality are largely the result of general advances in the care of critically ill patients and in ventilatory strategies. [6] Thus, caring for these patients requires close attention to recognition and treatment of the underlying medical and surgical disorders (e.g., sepsis, aspiration, and trauma). Appropriate treatment of any precipitating infection such as pneumonia or sepsis is critical to enhance the chance of survival. In a patient with sepsis and ALI/ARDS of unknown source, an intra-abdominal process should be considered. Timely surgical management of intra-abdominal sepsis is associated with better outcomes. [7] Minimizing procedures and their complications; prophylaxis against venous thromboembolism, gastrointestinal bleeding, and central venous catheter infections; prompt recognition of nosocomial infections, and provision of adequate nutrition. Lung protective ventilation, which is a low tidal volume ventilatory strategy, reduces mortality. A noninvasive ventilator support through a tight-fitting facemask or a nasal mask for pressure support ventilation or bi-level positive airway pressure ventilation is preferred in selected patients. [6],[7]
This observational, prospective study enrolled 58 consecutive cases of ALI/ARDS admitted to a medical intensive care unit (MICU) of a tertiary care hospital over a period of 1 year (July 2008-June 2009). This study aimed to assess various etiologies of ALI/ARDS, to determine the correlation between the diagnostic criteria and need of mechanical ventilation, and to correlate biochemical factors with the outcome of patients. They were assessed, investigated, and treated as per the existing practices without disturbing their routine protocol. Institute′s Ethics committee approval was obtained for this study. After the valid written consent, the following data were recorded: Name, age, sex, address, diagnosis, general, and clinical examination, investigations namely complete blood count, liver function tests, renal function tests, arterial blood gas analyses, chest radiographs, details of ventilatory mode and weaning methods for patients needing mechanical ventilation, development of ventilator-associated pneumonia (VAP), and stay in the MICU. Diagnostic criteria used for ARDS/ALI were as per AECC guidelines. [1] The parameters defined for organ failure were: Circulatory failure as systolic BP<90 mmHg, hematologic involvement as platelet count <100000, hemoglobin of <8.0 mg/dl, renal failure as serum creatinine >2 mg/dl, acidosis (pH < 7.25, bicarbonate <20 meq/l), and hepatic failure as total bilirubin >2 mg/dl. [8] We included all patients with ARDS/ALI in the study and excluded patients with cardiac failure, chronic kidney diseases with fluid overload states and age below 12 years. The data were analysed applying χ2 -test, multivariate logistic regression analysis of significance, using the computer-based program SPSS.
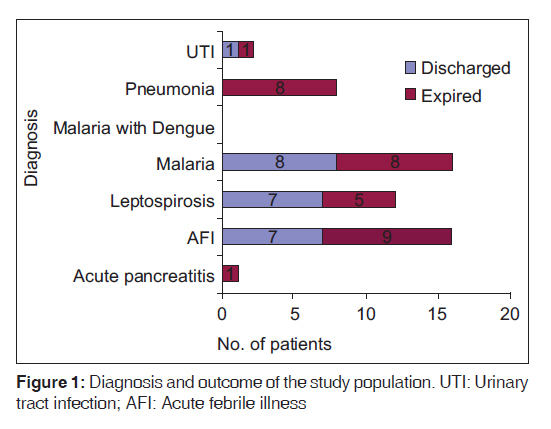
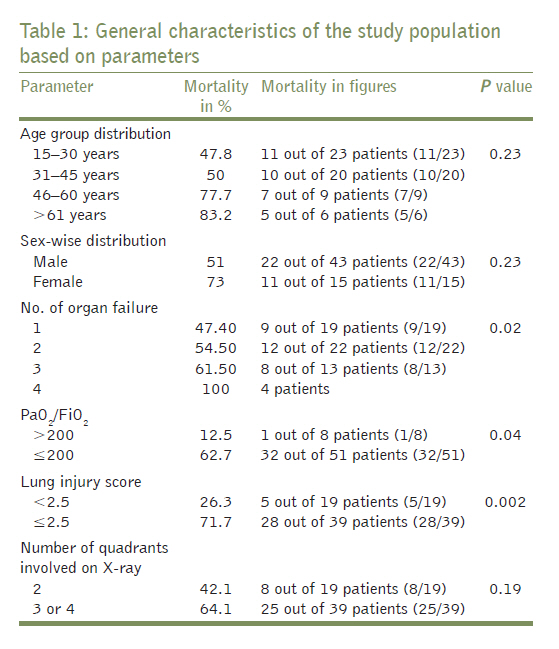
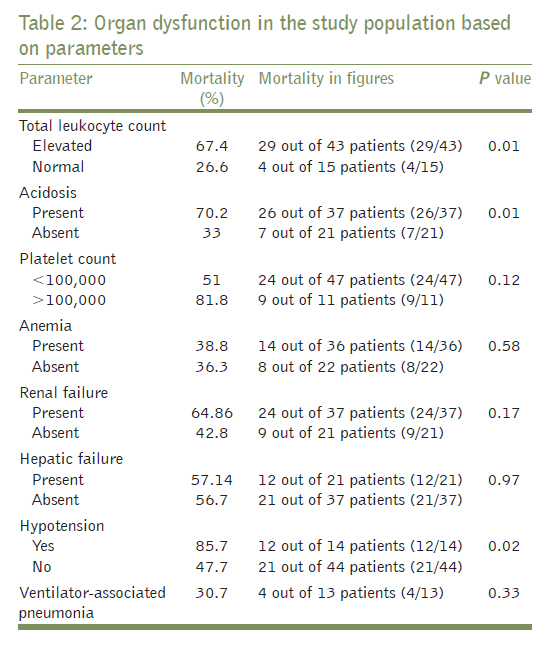
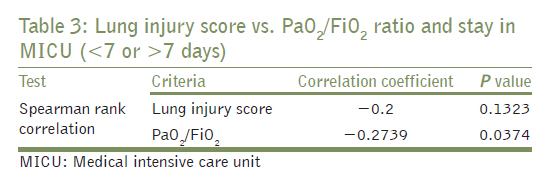
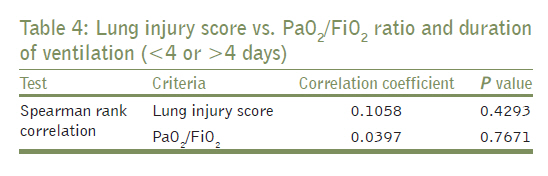
Since its recognition in 1967, a lot of clinical studies and trials have been conducted in the field of ALI/ARDS. This study attempts to establish the correlation between the clinical profile and outcome of patients with ALI/ARDS in an Indian perspective. We enrolled 58 patients, 43 males (74%) and 15 females (26%). Out of them 22 males (51%) and jp11 females (73.3%) expired, with a total mortality of 57% (33 out of 58). Although apparently mortality was more in females, it was statistically not significant. Factors attributable for ALI/ARDS were: Malaria in 16 patients (27.6%), leptospirosis in 12 (20.7%), malaria with dengue in 3 (5.2%), undiagnosed fever in 16 (27.6%), pneumonia in 8 (13.8%), urinary tract infection in 2 (3.4%), and pancreatitis in one (1.7%) patient [Figure - 1]. Out of 41 patients with PaO 2 /FiO 2 <200, 40 patients required invasive ventilation, and out of 17 patients with PaO 2 /FiO 2 >200, jp11 though initially managed on noninvasive ventilation (NIV) subsequently required invasive ventilation, and remaining six were successfully managed on NIV. Out of 41 patients requiring mechanical ventilation, 36 had LIS >2.5, whereas only 3 out of 17 patients with LIS <2.5 required mechanical ventilation. Details of biochemistry and general characteristics of the study population based on parameters are provided [Table - 1] and [Table - 2]. Discussion This study comprised of 58 patients, 43 males (74%) and 15 females (26%). The National Heart, Lung and Blood Institute ARDS Clinical Trials Network, a large multiple centre trial carried out at 10 university centers with 861 patients of ARDS, had 60% males, while a cohort study, the King County Lung Injury Project (KCLIP), Washington, was spread over 21 hospitals and covering 1.74 million people, had 61% males. [9],[10] Although one Indian study, by Aggarwal and Gupta in 2005, reported the female gender as a risk factor for mortality. Hudson et al. found that gender had no effect on likelihood of development of ALIARDS and the mortality rate was similar in men and women. [jp11],[12] The mean age of the patients in this study was 37.9 years, much lower than that in Network and KCLIP studies (51 and 61 years, respectively). The reason behind predominant involvement of males (74%) and young patients (15-45 years, 73%) in this study would be higher environmental exposure in working males, causing more vector borne tropical infections such as malaria, leptospirosis, dengue, and undiagnosed febrile illnesses-in them with ALI/ARDS as a complication. In this study, the etiology of ALI/ARDS is mainly tropical infectious diseases, i.e. malaria (27.6%), leptospirosis (20.7%), malaria with dengue (5.2%), and undiagnosed fever (27.6%), while pneumonia (13.8%), urinary tract infections (3.4%) and pancreatitis (1.7%) contributing to the remaining [Figure - 1]. As this study was carried out in medical ICU, patients with trauma, multiple fractures, etc. were not admitted and hence could not be evaluated. In an analysis of 160 deceased patients in Mumbai, due to monsoon-related illnesses in September 2008, Bajpai et al. noticed a male:female ratio of 4:1 with a mortality of 22% due to malaria, 22% due to leptospirosis, and 54% due to undiagnosed fevers. A significant proportion of these patients had ARDS (28.2% clinically and 48.6% postautopsy). [13] These findings, closely related to this study,; may explain the male dominance and remarkable etiological contribution of tropical infections in this study. Among the Indian studies, a three and half year retrospective study of 98 patients died of ARDS at Apollo Hospital during January 1999 to June 2002, Dr. Avanti Vigga and Dr. S. Mantri found that the primary pulmonary infection was associated with ARDS in 25% of patients and sepsis was a significant risk factor. [14] Polytrauma (12 patients), postabdominal surgery, and pancreatitis (10 patients each) were other etiologies. Pepe et al., Fowler et al., and Hudson et al. have documented sepsis as a major etiological and prognostic factor, ranging from 38% to 75% of the cases. [12],[15],[16] In the current study, sepsis was noted in 43 out of 58 patients (74%) with a mortality of 88% (29 of 43 patients), hence the presence of sepsis was one of the most important aspect of the outcomes in patients presenting with ARDS/ALI (P=0.0146). A lot of controversies exist about the use of PaO 2 /FiO 2 ratio and more comprehensive LIS as prognostic markers of the outcome in patients with ALI/ARDS. In our study, mean PaO 2 /FiO 2 was 167 among discharged and jp115 among those who expired. Out of 51 patients with PaO 2 /FiO 2 <200, 32 expired (67.2%), while only 1 patient out of 8 (12.5%) with PaO 2 /FiO 2 >200 expired. Among 41 patients who needed mechanical ventilation, 40 had PaO 2 /FiO 2 <200, whereas out of 17 patients with PaO 2 /FiO 2 >200, jp11 patients who were initially given a trial of NIV, eventually progressed to ARDS with worsening arterial saturation, and increasing PaO 2 /FiO 2 ratio, ultimately requiring mechanical ventilation. Hence PaO 2 /FiO 2 is a significant predictor of mortality and need of mechanical ventilation [Table - 3] and [Table - 4]. Zilberberg and Epstein found similar mortality in patients with PaO 2 /FiO 2 <200 and those between 201 and 300 at presentation. [17] Doyle et al. observed that PaO 2 /FiO 2 at the time of onset of ARDS did not affect the outcomes. [18] On the other hand, the KCLIP study demonstrated significantly less mortality (P<0.001) in patients with PaO 2 /FiO 2 >200 on day 3 (28.6%) as compared to those with the ratio <200 (41.1%). [10] Similar to PaO 2 /FiO 2 ratio, LIS was not found to be useful as a predictor of outcomes. But one study done by Vasilyev et al. showed that the initial LIS correlates with mortality. [19] In this study, LIS was ≥2.5 in 39 patients (67.2%), out of which 28 patients expired (71.8%) as compared to 19 patients with LIS <2.5, out of which 5 expired (26.3%). Out of 41 patients requiring mechanical ventilation, 36 had LIS ≥2.5, as compared to 3 out of 17 (17.6%) requiring NIV. Hence, LIS was an individual predictor of mortality and necessity of mechanical ventilation. In our study, acidosis was present in 63.8% of patients (37 out of 58 patients), with a mortality of 70.2%. Therefore, acidosis was an individual predictor of mortality. Mean hemoglobin in this study was 9.66 mg/dl, which was not significant as a mortality predictor. Fowler and colleagues showed that pH <7.25, low bicarbonate (<20 meq/l), and anemia were indicators of worse prognosis and each of these factors individually increased relative risk of death at least two folds. [20] Thrombocytopenia (platelet count <1 lakh per cumm) was present in 81% (47) patients with PaO 2 /FiO 2 <200, out of which 41% (24) patients expired; however, there was no correlation with development of ARDS. Thommasen et al. found that about 51% patients with risk of developing ARDS had thrombocytopenia but still did not progress to ARDS. [21] Renal failure was observed in 37 patients, of which 24 (64.8%) expired, as compared with 21 patients without renal involvement, out of which 9 (42.8%) patients expired. Kraman et al. observed that a rise in creatinine over 2 mg/dl in patients with ARDS due to all causes led to 80% mortality. [22] In this study, 12 patients (85.7%) out of 14 with hypotension expired, as compared to 21 patients out of 44 (47.7%), without hypotension. In a study done by Gachot et al. of 40 patients with complicated malaria, 8 patients out of 12 who developed ARDS had hypotension at presentation, as compared to only 2 out of 28 who did not progress to ARDS. [23] Hepatic involvement was present in 21 patients out of whom 12 expired (57%), among 37 patients without hepatic failure, 21 patients (56.8%) expired. In a study by Brogan et al. of 490 patients with ARDS with multi-organ failure, mortality was 56%, 72%, 84%, and 100% depending upon whether 1, 2, 3, or 4 nonrespiratory organs were involved. [24] In this study, the mortality was 47.7%, 54.5%, 61.5%, and 100% in similar groups (P=0.0286). Therefore, multi-organ failure is significantly associated with mortality. In a Network trial, mean non-respiratory organ involvement was 1.8. In our study, it was 2.03 overall, 2.21 in expired patients and 1.8 in survivors. In this study, 17 patients were selected to be ventilated in a noninvasive manner. The criteria used for patient selection for NIV were hemodynamic stability, not intubated before presenting to ICU, were well compliant to the use the NIV mask and PaO 2 /FIO 2 200 at the time of admission. NIV failure was defined as increased severity of illness clinically, and SpO 2 <90% on the pulse-oximeter after a 1-h trial of NIV. In a prospective multiple center cohort study from March 2002 to April 2004, Antonelli et al. were successful in avoiding intubation in 54% patients (79 out of 147) using NIV. [25] This also decreased the VAP significantly (2% vs. 20% in intubated patients; P<0.001) and ICU mortality (6% vs. 53%). In this study, though apparently all 17 patients who were ventilated in a non-invasive manner survived, the patient selection might had been responsible for this difference, as these patients were not as ′sick′ as those were ventilated by an invasive manner. More studies are required for determining criteria for using NIV. It must not be overlooked that only 20% (8 out of 41) patients those who were invasively ventilated survived. VAP was seen in 13 (25.4%) out of 51 patients who were mechanically ventilated, out which 4 patients expired; VAP in ARDS patients was late-onset and was caused by highly antibiotic-resistant microorganisms. Wunderink et al. and Philippe et al. observed that VAP in ARDS patients is usually late-onset and therefore caused by highly antibiotic-resistant microorganisms. Somewhat surprisingly, the mortality of ARDS patients with VAP is not significantly greater than that of ARDS patients without VAP, although subsequent duration of mechanical ventilation is consistently prolonged in patients with VAP. [26],[27] In this study, 8 (42%) out of 19 patients expired had 2 quadrants involvement on X-ray, as compared to 25 (64%) out of 39 patients with three or four quadrants involved. X-ray pictures of patients with ALI/ARDS were studied by Hudson and Steinberg. [28] They found that even involvement of three or four quadrants with fluffy shadows did not correlate with mortality. Mean stay in MICU for the survived patients was 10.44 days and 4.55 days for those who expired. Also the survived patients were ventilated for more days (mean of 5.24) than those who expired (mean of 3.85 days). Although neither PaO 2 /FiO 2 nor LIS was a predictor of duration of ventilation (P value = 0.767 and 0.429, respectively), PaO 2 /FiO 2 was a better indicator than the LIS was when the duration of stay in the MICU was concerned (P value: 0.037 vs. 0.132). Finally, the mortality of our study was 56.8% which was more than that observed during recent studies (32-45%). Exclusion of trauma-related ARDS cases which usually have better prognosis would be the possible explanation for this result.
In conclusion, from the experience of this study, we put forth the following: Malaria, leptospirosis, and undiagnosed fever were the main etiologies followed by pneumonia, urinary tract infections, and pancreatitis. Both PaO 2 /FiO 2 ratio and LIS at the time of admission were significant predictors of the outcome of the patients with ALI/ARDS and of necessity of mechanical ventilation. Although neither PaO 2 /FiO 2 nor LIS was significantly related to the duration of mechanical ventilation, PaO 2 /FiO 2 was a better predictor of duration of stay at the intensive care unit than the LIS was. Sepsis, acidosis, hypotension, and multiorgan failure were individual predictors of mortality in patients with ARDS while age, sex, anemia, thrombocytopenia, renal failure, hepatic failure, and X-ray picture were not predictors of the outcome. The overall mortality was 57%. More studies are required for determining criteria for using NIV. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11083t1.jpg] [jp11083t4.jpg] [jp11083t3.jpg] [jp11083t2.jpg] [jp11083f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}