 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 291-297 Original Article An evaluation of the effect of atorvastatin on memory and psychomotor functions in hypertensive patients S Prajapati1, CK Desai2, RK Dikshit2 1 Medical Advisor, Cadila Healthcare Ltd., Ahmedabad, Gujarat, India Date of Submission: 27-Jan-2011 Code Number: jp11084 PMID: 22120857 Abstract Background : The effect of statins on memory and psychomotor function has been controversial and needs further evaluation. Keywords: Amlodipine, atorvastatin, enalapril, hypertension, memory, psychomotor function Introduction Statins are effective and commonly prescribed drugs for hypercholesterolemia. They have received considerable attention in recent times due to their beneficial effects on multiple physiological systems. After realization of pleiotropic effects of statins, [1] they are being prescribed to patients suffering from cardiovascular disorders like hypertension and ischemic heart disease, irrespective of the lipid profile. Atorvastatin is the most commonly prescribed statin in the world. [2] Cholesterol reduction using statins improves memory in some cases but not others. Controversy exists over use of statins to alleviate memory problems in Alzheimer′s disease (AD). Correlations of cholesterol and cognitive function are mixed and association studies find that some genetic polymorphisms are related to cognitive function but others are not. [3] Recently, some concerns are raised regarding effects of atorvastatin (and all statins) on memory and psychomotor functions. A total of 23 cases of memory loss and psychomotor dysfunction have been reportedly associated with atorvastatin therapy. [4] However, reports from other studies are contradictory. For example, a prospective study in India has shown beneficial effects of atorvastatin on memory and psychomotor functions. [5] A retrospective case-control study has also demonstrated protective effects of atorvastatin and other statins too on dementia. [6] Hypertension is also known to affect memory and psychomotor functions. [7] Antihypertensive drugs are prescribed for lifetime in most patients and an effect of these drugs on these functions could alter the quality of life of the patients. This study therefore aims to evaluate the effect of atorvastatin on memory and psychomotor functions in hypertensive patients who are prescribed antihypertensive medications. The study involves the use of simple paper and pencil tests that are easy to administer in semi-literate patients in busy outpatient settings of Indian hospitals. Materials and Methods This was a prospective, open-label, parallel group longitudinal study designed to evaluate the effect of atorvastatin on memory and psychomotor functions in patients suffering from hypertension. Healthy volunteers were also enrolled in the study to detect differences, if any in the memory and psychomotor functions between normotensive population and hypertensive patients. The study was carried out at the Medicine outpatient department (OPD of a tertiary care hospital). The study protocol was approved by the Institutional Ethics Committee. Written, voluntary, informed consent was taken from all the patients and healthy volunteers prior to their enrollment in the study. To enable detection of a difference of 10% in mean change in PGI (Post Graduate Institute, Chandigarh) memory score between the Test and Control groups with 90% power at a 5% significance level, it was estimated that 65 patients were required allowing for an 15% withdrawal rate during the study. Patients of 18 to 55 years, of either gender, suffering from hypertension, who were prescribed amlodipine or Angiotensin Converting Enzyme (ACE) inhibitors within last one year, with or without newly prescribed atorvastatin on the day of enrollment, were screened in the Medicine OPD. They had a minimum educational qualification up to 5 th standard of schooling and were able to read and write Gujarati, Hindi, or English, to enable them to perform the tests of memory and psychomotor functions. Patients suffering from neuropsychiatric diseases (depression, Parkinsonism, AD, etc.), those who were prescribed drugs that could affect cognitive functions (benzodiazepines, antihistaminics, etc.), and those who were unwilling to report for regular follow-up were excluded from the study. The patients and healthy volunteers were divided into five groups as follows:
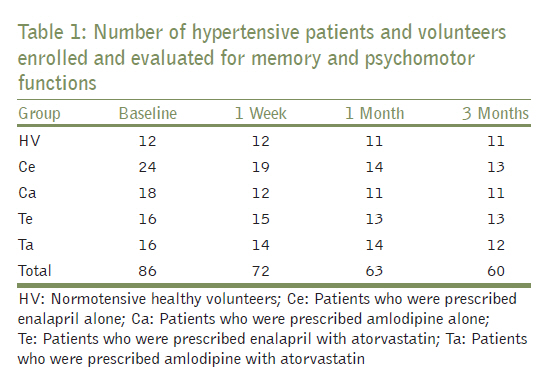
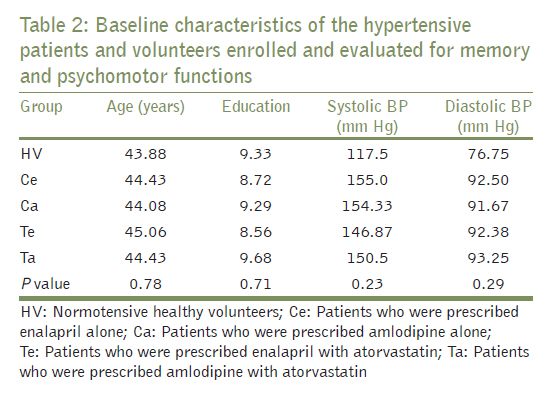
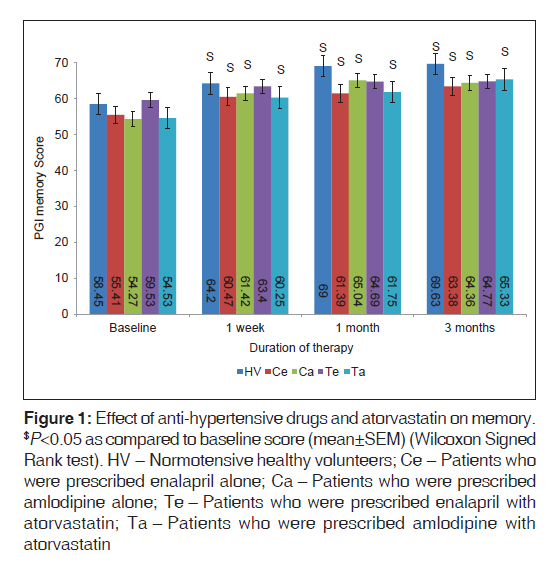
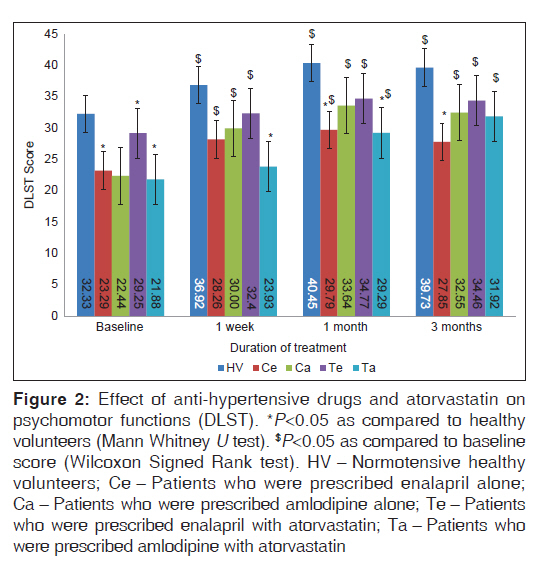
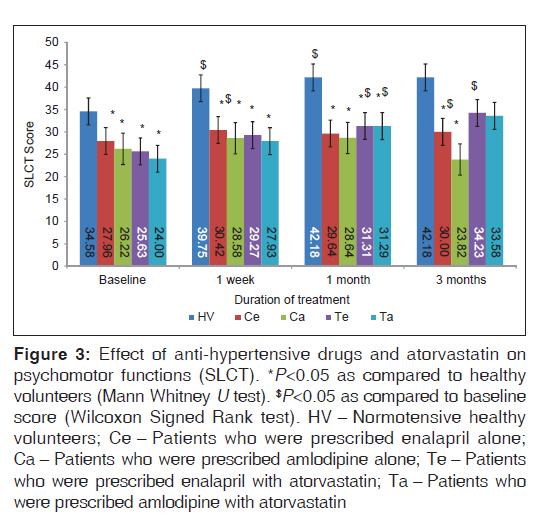
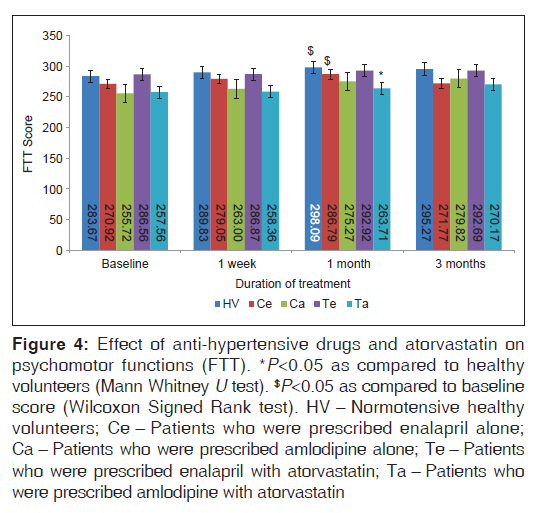
Groups (I) and (II) were considered as test groups, while groups (III) and (IV) were considered as control groups. In the initial visit, complete medical history specially related to inclusion and exclusion criteria was taken and blood pressure (BP) was recorded. All the patients and volunteers were explained the study method and written, Informed Consent Form was signed by them. The patients and HV were evaluated for memory and psychomotor functions on Day 0. The patients in group I and II received atorvastatin after the day 0 tests were performed. They were again evaluated at one week, one month, and three months after their enrollment in the study. Following tests were used for evaluation of memory and psychomotor functions. Post Graduate Institute, Chandigarh, memory scale The Post Graduate Institute, Chandigarh, memory scale was developed by Pershad and Wig. [8] It is a specially designed test for evaluation of memory in semi-literate people suitable for the Indian population. It is comprised of 10 sub-tests to measure different components of memory (remote and recent memory, mental balance, attention and concentration, delayed and immediate recall, verbal retention of similar and dissimilar pairs, visual retention and recognition of common objects). This scale has been validated with internationally acclaimed tests like Wechsler Adult Intelligence Score and Boston Memory Scale. Total maximum score for these tests is 100. Digit letter substitution test It is a simple paper and pencil test used for evaluation of coordination of sensory and motor nervous system. [9] It could be used as an alternative for Digit Symbol Substitution Test. [10] The test sheet consists of a key which has pairs of digits (1-9) and alphabets in English, Gujarati (the commonly spoken language in Gujarat, India), or Hindi. The patient/volunteer substitutes alphabets in place of the digits in the working section. The correct substitutions made during a period of 90 seconds are recorded. Six letter cancellation test This is a simple paper and pencil test that is used to evaluate perceptual processing of sensory information. [9] The sheet is in English, Gujarati, or Hindi. The key is comprised of six target alphabets. The working section displays all alphabets of the respective language arranged randomly in rows and columns. The patients/volunteers are asked to identify and cancel the alphabets. The number of correct cancellations made during a period of 90 seconds is recorded. Finger tapping test It is a test for evaluating psychomotor speed, fine motor coordination, and accuracy. [jp11] Patient/volunteer is asked to tap a fixed key on a calculator as fast as possible for 60 seconds. The number of accurate finger taps in one minute is recorded in the calculator and noted. Statistical analysis Student′s t test was used for comparison of demographic (age and education) and clinical parameters (systolic and diastolic BP) between the groups. Wilcoxon Signed Rank Test was used to compare test scores obtained at one week, one month, and three months in each group with the respective baseline (Day 0) scores. Mann Whitney U Test was used to compare test scores obtained in the respective groups (Test, Control, and HV) at different time periods. Statistical significance was considered at P<0.05. Statistical Package for Social Services (SPSS) 17 was used for statistical analysis. Results Of 74 patients and 12 HVs enrolled in the study, 60(49 patients and jp11 HVs) completed the follow-up at three months. Twenty-one participants (20 patients and one HV) did not report for follow-up regularly. Four patients were prescribed other drugs subsequently due to concurrent diseases and were hence excluded from the study. One patient developed pedal edema with amlodipine and hence the drug was withdrawn. The number of patients followed up in each group [Table - 1]. The baseline characteristics of the patients and volunteers are shown in [Table - 1]. All four groups of patients were comparable with respect to age, education, and BP. A significant reduction was observed in systolic and diastolic BP in all patients throughout the study period suggesting that the prescribed antihypertensive therapy was effective in these patients [Table - 2]. Evaluation of memory in patients and normotensive healthy volunteers (1) HV group: A statistically significant increase in scores of delayed (P=0.01) and immediate recall (P=0.004), recognition (P=0.02), and total scores of memory (P=0.009) was observed in healthy volunteers at three months as compared with the baseline. (2) Ce group: A statistically significant increase in scores of remote memory (P=0.034), immediate recall (P=0.04), verbal retention of dissimilar pairs (P=0.02), and total scores of memory (P=0.008) was observed in hypertensive patients receiving enalapril at three months as compared with the baseline. (3) Ca group: A statistically significant increase in scores of delayed (P=0.016) and immediate recall (P=0.01), visual retention (P=0.041), and total scores of memory (P=0.005) was observed in hypertensive patients receiving amlodipine at three months as compared with the baseline. (4) Te group: A statistically significant increase in scores of immediate recall (P=0.008) was observed in patients receiving enalapril and atorvastatin at three months as compared with the baseline. (5) Ta group: A statistically significant increase in scores of remote (P=0.004) and recent memory (P=0.025), verbal retention of dissimilar pairs (P=0.03), and total scores of memory (P=0.009) was observed in patients receiving amlodipine and atorvastatin at three months as compared with the baseline [Figure - 1]. Evaluation of psychomotor functions in hypertensive patients and normotensive healthy volunteers (1) HV group: A statistically significant increase in Digit Letter Substitution Test (DLST) scores (P=0.016) was observed in healthy volunteers as compared with the baseline throughout the study period. A statistically significant increase in Six Letter Cancellation Test (SLCT) scores (P=0.0jp11) was observed up to one month. A statistically significant increase in Finger Tapping Test (FTT) scores (P=0.04) was also observed at one month. (2) Ce group: A statistically significant increase in DLST (P=0.031) and SLCT scores (P=0.016) was observed in hypertensive patients receiving enalapril as compared with the baseline throughout the study period. A statistically significant increase in FTT scores (P=0.036) was observed at one month. (3) Ca group: A statistically significant increase in DLST (P=0.005) scores was observed in hypertensive patients receiving amlodipine as compared with the baseline throughout the study period. (4) Te group: A statistically significant increase in DLST (P=0.028) and SLCT scores (P=0.04) was observed in hypertensive patients receiving enalapril and atorvastatin up to one month of therapy as compared with the baseline. (5) Ta group: A statistically significant increase in DLST scores (P=0.02) was observed in hypertensive patients receiving amlodipine and atorvastatin at three months as compared with the baseline. A statistically significant increase in SLCT scores (0.003) was observed at one month of therapy [Figure - 2],[Figure - 3],[Figure - 4]. Comparison of memory and psychomotor functions between healthy volunteers and hypertensive patients Test scores of memory and psychomotor functions in healthy volunteers were compared with those of hypertensive patients to detect effect of hypertension and its treatment on these functions. The demographic parameters were comparable between healthy volunteers and patients. Hence, any observed differences in these functions between the groups could be attributed to effect of hypertension or its treatment. Evaluation of memory (1) Ce group: Scores of verbal retention of similar pairs (P=0.04) and delayed recall (P<0.001) were significantly lower in hypertensive patients treated with enalapril as compared with those of healthy volunteers at one week and one month of treatment, respectively. (2) Ca group: Scores of remote memory were significantly lower in hypertensive patients treated with amlodipine as compared with those of healthy volunteers at one week (P=0.01) and three months (P=0.01) of treatment. (3) Te group: Scores of delayed recall (P=0.04) and remote memory (P=0.03) were significantly lower in hypertensive patients treated with enalapril and atorvastatin as compared with those of healthy volunteers at one month and three months of treatment, respectively. (4) Ta group: Scores of delayed recall (P=0.01) and remote memory (P<0.001) were significantly lower in hypertensive patients treated with amlodipine and atorvastatin as compared with those of healthy volunteers at one month and three months of treatment, respectively. Thus, scores of certain domains of memory in all groups of hypertensive patients were poorer as compared with those of healthy population [Figure - 1]. Evaluation of psychomotor functions Ce group: DLST (P=0.02) and SLCT scores (P=0.018) were significantly lower in hypertensive patients treated with enalapril as compared with those of healthy volunteers at one month and three months of treatment, respectively. There was no significant difference in FTT scores between these groups. (2) Ca group: SLCT scores (P=0.001) were also significantly lower in hypertensive patients treated with amlodipine as compared with those of healthy volunteers at three months of treatment. (3) Te group: SLCT scores were significantly lower in hypertensive patients treated with enalapril and atorvastatin as compared with those of healthy volunteers at one week (P=0.01) and one month (P=0.02) of treatment, respectively. (4) Ta group: DLST (P=0.018) and SLCT scores (P=0.021) were significantly lower in hypertensive patients treated with amlodipine and atorvastatin as compared with those of healthy volunteers at one month of treatment. FTT scores were also significantly lower in them at one month (P=0.02) as compared with healthy volunteers [Figure - 2],[Figure - 3],[Figure - 4]. Thus, scores of certain domains of psychomotor functions in all groups of hypertensive patients were poorer as compared with those of healthy population. Effect of atorvastatin on memory and psychomotor functions The test scores for memory and psychomotor functions in hypertensive patients prescribed enalapril or amlodipine were compared with the scores in patients who were prescribed atorvastatin with enalapril or amlodipine to evaluate the effect of atorvastatin in these patients. These patients were comparable for demographic parameters and there was no significant difference in the baseline scores of memory and psychomotor functions between these groups. Hence, any observed difference in these functions between these groups could be attributed to atorvastatin. Comparison of memory and psychomotor functions between patients treated with enalapril and those treated with enalapril and atorvastatin Memory No significant difference in memory scores was observed between patients receiving enalapril alone and those of patients who were receiving enalapril with atorvastatin throughout the study period [Figure - 1]. Psychomotor functions No significant difference in scores of psychomotor functions was observed between patients receiving enalapril alone and those of patients receiving enalapril with atorvastatin throughout the study period [Figure - 2],[Figure - 3],[Figure - 4]. Comparison of memory and psychomotor functions between patients treated with amlodipine and those treated with amlodipine and atorvastatin Memory No significant difference in memory scores was observed between patients receiving amlodipine alone and those of patients receiving amlodipine with atorvastatin throughout the study period [Figure - 1]. Psychomotor functions No significant difference in scores of psychomotor functions was observed between patients receiving amlodipine alone and those of patients receiving amlodipine with atorvastatin throughout the study period [Figure - 2],[Figure - 3],[Figure - 4]. Thus, treatment with atorvastatin in hypertensive patients treated with enalapril or amlodipine does not have any effect on memory and psychomotor functions. Discussion This study evaluates the effect of atorvastatin on memory and psychomotor functions in hypertensive patients adequately treated with enalapril or amlodipine. Tests involving complex electronic gadgets are used to evaluate drug-induced changes in memory and psychomotor functions in developed countries. These sophisticated tests are impractical in semiliterate population attending our ill-equipped public sector hospitals. Many simple paper and pencil tests for evaluation of memory and psychomotor functions have been found to be as equally sensitive as those used by researchers in developed countries. [8] The results of the study suggest that treatment with atorvastatin does not affect the memory and psychomotor functions in patients of hypertension during initial three months of therapy (primary outcome). The study also suggests that both enalapril and amlodipine improve the memory and psychomotor functions in hypertensive patients (secondary outcome). An improvement in memory and psychomotor functions was observed in all patient groups. A significant improvement in immediate recall was observed in patients receiving enalapril with or without atorvastatin. A similar improvement in overall memory was also observed in patients receiving amlodipine with or without atorvastatin. This improvement can be attributed to the antihypertensive treatment and supported by previous studies, showing that adequate treatment of hypertension can cause improvement in memory and psychomotor functions. For instance, a study showed that elderly patients with mild-to-moderate hypertension and slightly impaired cognitive functions are at increased risk of dementia and cardiovascular events and that effective antihypertensive therapy may reduce cognitive decline and stroke incidence in these patients. [12] Frcka and Lader [13] had observed the effect of administration of enalapril (20 mg/day) for eight days in healthy volunteers using various tests of memory and psychomotor functions like Digit Symbol Substitution Test (DSST), Symbol Copying Test, Critical Flicker Fusion, and Tapping Interval Test. They found that enalapril significantly improved these functions. These findings are corroborated by our study that shows significant improvement in remote memory, immediate recall, verbal retention of dissimilar pairs, overall memory, and psychomotor performance (including DLST) in patients receiving enalapril. A similar improvement in DSST during 12 weeks of enalapril treatment was observed in hypertensive patients in a double blind, parallel study conducted by Herrick et al. [14] A significant improvement was observed in delayed and immediate recall, visual retention, overall memory, and psychomotor improvement in our patients receiving amlodipine. This is supported by a comparison of effect of sustained release nifedipine and amlodipine on psychomotor functions which showed that amlodipine caused significant improvement in scales of Mental Acuity and Detachment/Disorientation as compared with nifedipine group. [15] All hypertensive patients in the present study had some impairment in certain components of memory and psychomotor functions as compared with those of healthy volunteers. Patients treated with enalapril with or without atorvastatin had poorer delayed recall as compared with healthy volunteers, whereas patients treated with amlodipine with or without atorvastatin had poorer remote memory as compared with healthy volunteers. Psychomotor performance, especially in SLCT, was impaired in all patients. This difference between hypertensive patients and normotensive volunteers may be due to the deleterious effects of hypertension on the central nervous system as similar effects have been observed in other studies too. In a study carried out by Franceschi et al., [16] memory and psychomotor functions were compared between 15 normotensive subjects, 17 newly diagnosed, untreated hypertensive patients, and 22 effectively treated hypertensive patients receiving thiazide diuretics. Different tests were carried out to evaluate memory (Wechsler Memory Scale) and psychomotor functions (DSST, Card Sorting Test, Wechsler-Bellevue Scale and Benton′s Visual Retention Test Form B). It was found that both memory and psychomotor functions were better in healthy volunteers as compared with those in treated and untreated hypertensive patients. The study carried out by Elias MF observed that the level of BP and duration of hypertension were inversely related with the composite scores of attention and memory. [7] Both these studies support the findings of our study. In the present study, three months′ treatment with atorvastatin did not produce any significant alteration in memory and psychomotor functions in hypertensive patients adequately treated with either enalapril or amlodipine. It is difficult to compare the findings of our study with other studies because of difference in variables like population, use of different tests for memory and psychomotor functions, variable age groups, different concomitant therapies, different study designs and study duration. Furthermore, studies evaluating effect of statins on memory and psychomotor functions in hypertensive patients are few. In a randomized, double blind, placebo-controlled, crossover study carried out to compare the effects of simvastatin (20 mg/day), pravastatin (40 mg/day), and placebo on memory and psychomotor functions, it was observed that both simvastatin and pravastatin did not differ significantly in any of the tests of memory (Selective Reminding and Word Recall) or psychomotor functions (DSST, Auditory vigilance, Choice Reaction Time, and FTT) as compared with the placebo. [17] Other clinical trials have yielded inconsistent results regarding the benefits of statins in AD. A 12-week open-label trial was conducted with simvastatin 40 mg/d and then 80 mg/d in 12 patients with AD or amnestic mild cognitive impairment and hypercholesterolemia. A modest but significant inhibition of brain cholesterol biosynthesis after simvastatin treatment was observed, but there were no changes in AD biomarkers. These findings suggest that simvastatin treatment can affect brain cholesterol metabolism within 12 weeks, but did not alter molecular indices of AD pathology during the short-term treatment. [18] On the other hand, a study carried out in aged Familial Hypercholesterolemia patients receiving long-term statin therapy showed that these patients exhibited better episodic memory than population controls, and this association became even more pronounced with longer statin therapy. [19] A population-based study was carried out in 137 participants who were receiving statins and 4jp11 matched controls in Central Spain. The subjects underwent a neuropsychological assessment, including tests of global cognitive performance, frontal-executive function, verbal fluency, and memory. Median duration of statin treatment was 2 years. Of 137 participants receiving statins, 53 (38.7%) were taking pravastatin, 38 (27.7%) were taking simvastatin, 37 (27.0%) were taking lovastatin, 6 (4.4%) were taking fluvastatin, and 3 (2.2%) were taking atorvastatin. It was observed that statin users and controls performed similarly on all neuropsychological and cognition tests. These results do not support a positive benefit of statins on cognition. [20] In a large cohort study carried out over a period of two years, psychomotor functions in 315 elderly patients (age >65 years) receiving statins were compared with 441 patients not using statins. No significant difference in psychomotor performance as measured by Trail Making Test (Part B) was observed between statin users and non-users. [21] In a meta-analysis of 60 case reports (of which 23 were associated with atorvastatin) of suspected statin-induced memory loss, it was concluded that there was no prospective evidence of either neurocognitive risks or benefits with statin therapy, [4] a finding that is corroborated by our study. On the other hand, altered neuronal activation while taking atorvastatin and reduced performance on established cognitive tests assessing memory and learning have been reported in a case report. [22] The patient in this case reported subjective resolution of his cognitive adverse effects, demonstrated improved cognitive test performance, and showed functional magnetic resonance imagingpatterns similar to those expected in a healthy individual. Based on the findings of this study and corroborative findings of other studies, it is therefore concluded that therapy with antihypertensive drugs can improve memory and psychomotor functions in hypertensive patients. Atorvastatin does not produce significant change in memory and psychomotor functions in adequately treated hypertensive patients. We studied the effect of atorvastatin on memory and psychomotor functions in Indian patients of uncomplicated hypertension. These functions were evaluated by simple pencil and paper tests which are easily applicable to the Indian population. We also demonstrated beneficial effects of antihypertensive therapy on memory and psychomotor functions in patients who are recently (within last one year) diagnosed with hypertension. The healthy volunteers in our study made a good control group representing the normotensive population. Our study suggests that use of atorvastatin (irrespective of lipid profile) for primary prevention of cardiovascular diseases is safe in hypertensive patients as far as memory and psychomotor functions are concerned. But, some limitations of our study cannot be overlooked. We studied the effect of atorvastatin on memory and psychomotor functions in a small number of patients, for a selective indication and for a short duration in an open-label study, whereas in clinical practice, atorvastatin is prescribed for longer durations, with multiple drugs in most patients. Our study, however, has important future implications. Recently, the beneficial effects of statins in hypertension have been observed. [23] These findings may increase utilization of statins in hypertensive patients for prophylaxis of cardiovascular morbidities like ischemic heart disease and peripheral vascular diseases. Hence, it is necessary to critically evaluate the safety of these drugs in these patients. Although the findings of our study suggests the safety of atorvastatin in hypertensive patients, as far as memory and psychomotor functions are concerned, similar findings should be replicated in studies with larger number of patients carried out for longer duration. Other adverse effects of statins (myopathy and hepatotoxicity) should also be considered before prescribing these drugs for prophylactic purposes. Acknowledgment We thank the faculty of Department of Medicine, Civil Hospital, Ahmedabad specially Dr. B. D. Mankad, Dr. A. N. Shah, Dr. B. K. Amin, Dr. U.J. Jani, Dr. N. M. Kadri, and Dr. B.B. Solanki for their expert advice in study design and cooperation in enrollment of patients. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11084t2.jpg] [jp11084f4.jpg] [jp11084t1.jpg] [jp11084f1.jpg] [jp11084f3.jpg] [jp11084f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}