 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 298-301 Original Article Severe and critical cases of H1N1 influenza in pregnancy: A chinese perspective J Liu, Q Li, H Cui, C Liu Department of Obstetrics and Gynecology, Shengjing Hospital, China Medical University, China Date of Submission: 24-Mar-2011 Code Number: jp11085 PMID: 22120858 Abstract Context : In 2009, an outbreak of A/H1N1 influenza spread worldwide. Following the start of winter in Liaoning province in China, the number of pregnant women infected with influenza increased significantly. Some of them developed respiratory failure and multiple organ failure. Keywords: China, H1N1 influenza, pregnancy, severe and critical cases Introduction In early April 2009, an outbreak of A/H1N1 influenza that began in Mexico spread worldwide. [1],[2] In patients affected with influenza, pregnant women had increased morbidity and mortality compared with women who were not pregnant. [3] This strain of influenza affected Northern China relatively late. Following the start of winter in the Liaoning province, the number of pregnant women infected with H1N1 influenza increased significantly. Furthermore, for some, their condition deteriorated very quickly after they came to our hospital, and soon developed critical infection with respiratory failure and multiple organ failure. Prevention and treatment of critical cases became a social focus. So, it is very important to find the high-risk factors for critical illness. Materials and Methods This retrospective cohort study was carried out in the department of Obstetrics of a large general hospital after being approved by the institutional medical ethics committee. The department is a tertiary care unit for the surrounding areas and it undertakes a large number of high-risk pregnancies. The department caters to over 7000 admissions and conducts over 6000 deliveries per year. Approximately, 48% of these cases are high-risk pregnancies. In the study, clinical data of H1N1-infected pregnant women hospitalized during 2009 to January 2010 was reviewed. The patients were classified into severe and critical grades based on their condition, according to the H1N1 influenza treatment guidelines. [4] The patients were included for analysis if they were pregnant and presented with fever or acute respiratory illness, and were confirmed positive for A/H1N1 by a pharyngeal swab. Pharyngeal swabs of suspected cases visiting hospitals were collected and sent to the corresponding laboratories to detect 2009 H1N1 virus by a real-time reverse transcriptase polymerase chain reaction (RT-PCR) assay according to the US CDC protocol recommended by the World Health Organization (WHO). [5] Cases were classified as mild, severe and critical according to the following case definitions: [6] Severe cases: Included those having at least one of the following criteria:
Critical cases: Included those having at least one of the following criteria:
Mild cases: Included those infected cases not meeting any of the above criteria. The mild cases received antiviral treatment (using antiviral drugs) in the outpatient clinic and were advised isolation at home. The severe or critical cases were hospitalized and isolated. Statistical analyses were performed with SPSS software (Version 17.0, SPSS). We selected maternal age, gestational age, interval between symptom-onset and hospital admission as risk factors. A logistic regression analysis was conducted to determine risk factors for critical cases. The analysis compared severe and critical cases. Frequencies and percentages were used to describe the distributions of cases.
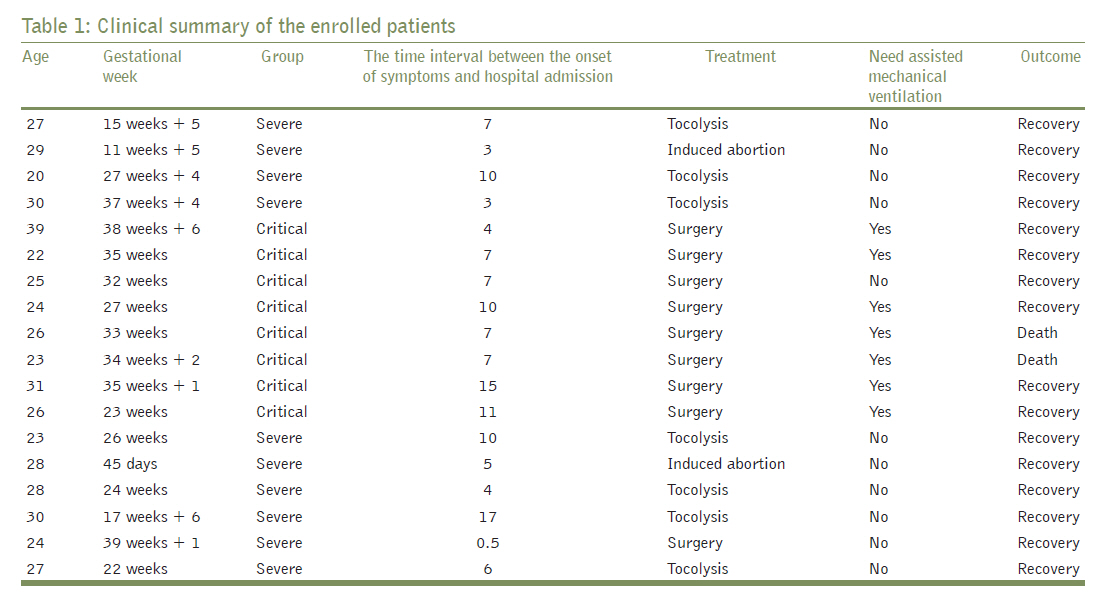
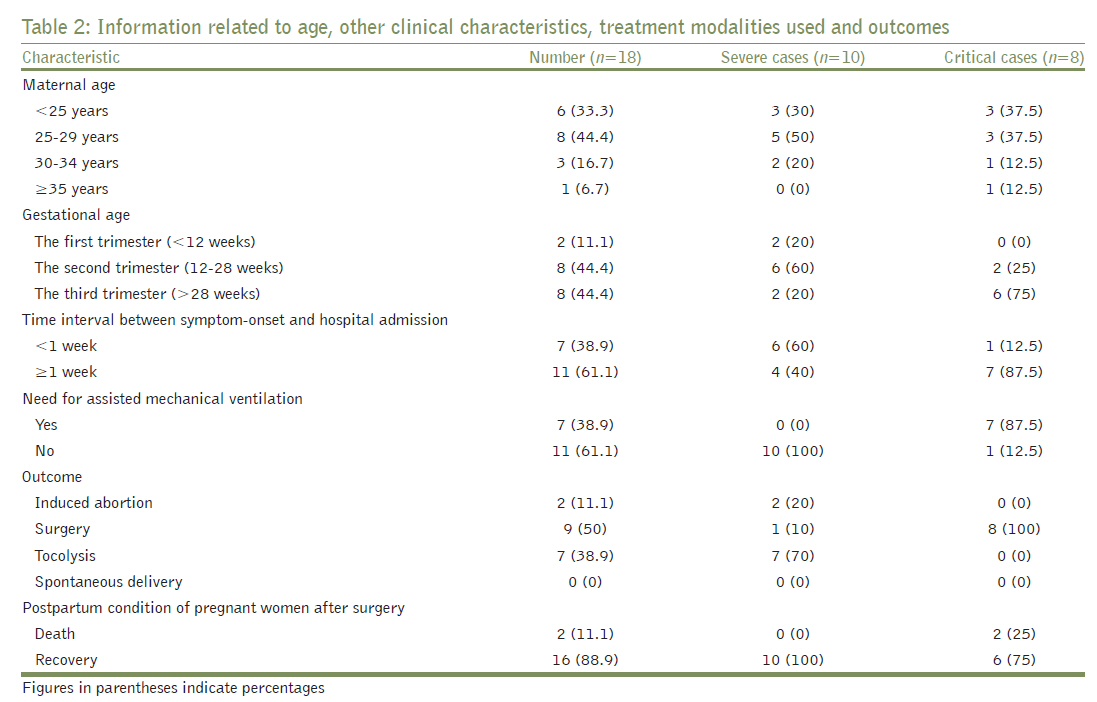
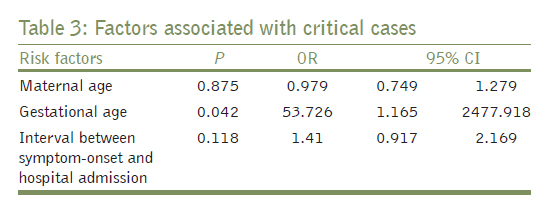
Eighteen cases of A/H1N1 influenza pregnant women were admitted during the period of review [Table - 1]. Information regarding their clinical characteristics, treatment details and outcome are summarized in [Table - 2]. Ten pregnant women were severe cases and eight pregnant women were critical cases. Their age ranged from 20-39 years (median 26.8). Two (11%) of them presented in the first trimester, eight (44%) in the second trimester, and the remaining eight (44%) in the third trimester. The interval between symptom-onset and hospital admission was 0.5-15 days. Seven patients (39%) required mechanical ventilation. Three patients underwent Caesarean section with the aim to improve symptoms and oxygen saturation, although their fetuses had died in utero (at 27, 33 and 38 weeks of gestation) before coming to hospital. Six patients underwent Caesarean deliveries. All infants survived, and none of the babies had evidence of influenza. Two (11%) patients in this series died and the remaining were discharged home. After discharge, two patients underwent induced abortion for the termination of pregnancy. Other patients who did not deliver continued their pregnancy. We evaluated maternal age, gestational age, and the time interval between symptom-onset and hospital admission as related factors of susceptibility [Table - 3]. The trimester was determined on the basis of the last menstrual cycle in patients with regular cycles and on the basis of ultrasound evidence in those with irregular cycles. In binary logistic analysis, the significant risk factor associated with critical cases compared to severe cases was gestational age (OR=53.726, 95% CI: 1.165~2477.918). But in this study, the maternal age (OR=0.979, 95% CI: 0.749~1.279)and the time interval between symptom-onset and hospital admission (OR=1.41, 95% CI: 0.917~2.169) were not found to be risk factors for critical cases. We chose hospitalized non-pregnant female cases of A/H1N1 infected in this period as the reference group to find the relationship between gestation and critical illness. There were thirty cases of hospitalized non-pregnant female patients with A/H1N1 infected. Of the thirty patients, only one presented critical illness. We found that the risk of critical illness varied by weeks of gestation, with an odds ratio of 1.034 (95% CI: 0.968-1.106) during the first trimester, 9.667(95% CI: 0.750-124.59) during the second trimester, and 87 (95% CI: 6.750-1121.39) during the third trimester [Table - 4]. Discussion H1N1 influenza has been identified as a cause of febrile respiratory infection. It spread throughout a world population infecting almost entirely the population susceptible to infection. [1],[2],[7] H1N1-infected pregnant women were shown to have increased frequency of complications and greater morbidity than the general population. [8],[9] This study summarizes the severe and critical cases of 2009 H1N1 influenza in pregnancy. The study noted that gestational age was associated with higher risk of developing critical infection in our province in China. The risk increased with the weeks of gestation. Influenza increases the risk of severe respiratory diseases in pregnancy. [9],[10],[11] In our study, the women in the second or third trimester of pregnancy had a higher rate of developing critical infection, which is similar to that reported in the USA. [3] It may be related to specific immune suppression, decreased resistance and physiological changes in pregnancy. [12],[13],[14] If lung inflammation occurs, breathing is restricted and lung function is reduced. Blood volume increases in late pregnancy, increasing the burden on the lung, which may lead to easier deterioration. [15],[16] For these reasons, we performed surgery on patients whose condition did not improve with symptomatic treatment. The purpose was to terminate the pregnancy and to ease the symptoms of hypoxia. And we found that immediate and dramatic relief of symptoms was achieved after the Caesarean section. Similar to other studies, this study also did not find a significant association between the maternal age and critical illness. Delayed presentation to the hospital and delayed institution of anti-virus treatment have been associated the development of severe illness. [3],[6],[17],[18] When these patients have flu-like symptoms, they do not pay much attention to them and are worried about the impact drugs could have on the fetus. These concerns delay institution of treatment with disastrous consequences. As we studied only severe and critical cases in a retrospective study, we were unable to confirm this notion through our study. Our study has some limitations. As a referral center, this department receives more sick and severely ill patients. This may have introduced a selection bias. Our data, therefore, cannot be used to estimate the overall mortality of Critical 2009 H1N1 Influenza. Secondly, the patients who died at home or at the referring hospitals were not reported, so these were lost to enumeration in the study. Moreover, there is not enough power in the study, as there were only two cases in the first trimester. This has resulted in the statistical confidence intervals being too large. It may, however, be stated that critical infection cases were associated with increasing gestational age, and the risk increases with number of weeks of gestation. Close attention should be paid to pregnant women in their second and third trimester of pregnancy to decrease associated morbidity and mortality. For critical infection cases, Caesarean section can improve the symptoms of hypoxia quickly. Acknowledgment Funding support for this research by the Peak Medical Research Construction Projects of Liaoning Province. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11085t3.jpg] [jp11085t1.jpg] [jp11085t4.jpg] [jp11085t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}