 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
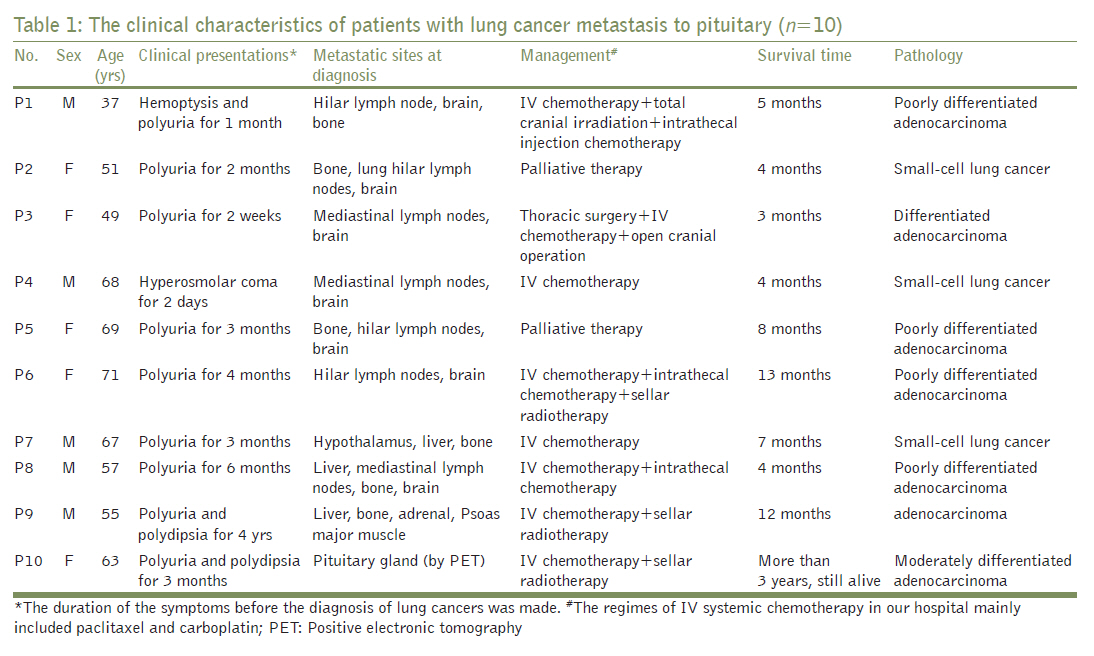
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 302-306 Original Article Diabetes insipidus as the first symptom caused by lung cancer metastasis to the pituitary glands: Clinical presentations, diagnosis, and management JF Mao1, JL Zhang2, M Nie1, SH Lu1, XY Wu1 1 Department of Endocrinology, Peking Union Medical College Hospital (PUMCH), Key Laboratory of the Health Ministry, Beijing, China Aims : To investigate the clinical features, diagnosis, and management of CDI caused by lung cancer metastasis to the pituitary glands. Materials and Methods : We retrospectively reviewed 10 patients who had CDI as their first symptom before their lung cancers were diagnosed. Their clinical presentations, anterior pituitary gland function, sellar magnetic resonance imaging (MRI), management, and prognosis were described. Settings and Design : This retrospective cross-sectional clinical study was conducted in a medical college hospital. Results : The patient's mean age was 58.6±7.8 years. Diabetes insipidus was the main complaint when they were referred to our hospital. MRI revealed specific dumbbell-shaped masses in the sella turcica in five patients. In seven patients whose hormones were measured, the levels of hormones from adenohypophysis were abnormally low in six patients. The main treatments included surgery, systemic chemotherapy, and sellar irradiation. Although nine patients had poor prognoses, one patient has survived for more than 3 years, suggesting benefit from early diagnosis and treatment. Conclusions : New-onset CDI might be the only symptom presented by the patients with pituitary metastasis (PM) from lung cancer. Dumbbell-shaped sellar masses in MRI are prone to the diagnosis of PM. A thorough examination for primary cancer should be carried out in these aged and elderly patients. Keywords: Central diabetes insipidus, lung cancer, metastasis, pituitary gland
Introduction A pituitary metastasis (PM) is an unusual complication of malignancy with an incidence of 1 to 1.5% in all kinds of tumors. [1] Since the first case of PM was reported in 1857, more than 500 patients with metastasis to pituitary from extracranial malignancies have been reported. [1],[2] In recent years, a wide use of sellar magnetic resonance imaging (MRI) and an increasing attention to differential diagnosis in central diabetes insipidus (CDI) have contributed to discovering more cases of PM from primary malignancies. A PM from lung cancer is also a rare clinical situation and less than 20 cases have been reported in recent 5 years. [3],[4],[5],[6] Lung cancer happens insidiously and is difficult to be detected in early stages. [7] CDI might be the only presentation of early-stage lung cancer and special attention should be paid to patients presenting with CDI in the absence of alternative etiology. Here, we report the clinical manifestations, diagnosis, and treatment of 10 patients who were admitted to our hospital with CDI as their first symptom.
Subjects We performed a retrospective analysis of 10 lung cancer patients with CDI as their first symptom in our hospital between January 1998 and December 2008. These patients were referred to the endocrinologists for new-onset polydipsia, polyuria, or hyperosmotic coma. We also included 1 639 patients with lung cancers and 306 patients with CDI admitted to our hospital between January 1998 and December 2008 to calculate the incidence of PMs. Methods In each patient, a contrast agent-enhanced sellar MRI and a thoracic computer tomography (CT) were conducted. Hormones from the anterior pituitary glands and their target glands, such as serum insulin-like growth factor-1, prolactin (PRL), glucocorticoid (F), adrenocorticotropic hormone, follicular-stimulating hormone, luteinizing hormone, estradiol, testosterone, thyrotropin, and thyroid hormones were measured in seven patients. The diagnosis of CDI was confirmed by the clinical manifestations and water restriction test. The symptoms of polydipsia and polyuria resolved after the administration of desmopressin. Lung cancers were diagnosed by CT-guide needle aspiration biopsy and bronchoscopy biopsy and confirmed pathologically after thoracotomy. Other imaging studies, such as whole-body CT scans, cranial MRI, bone scintigraphy, octreotide take-up scintigraphy, and positive electronic tomography (PET), were performed to locate the possible metastases. Follow-ups were conducted by telephone at intervals of 6 months. The procedures in this study were in accordance with the Helsinki Declaration of 1975. The written informed consents were obtained from the patients or their family members. This study was approved by the ethics committee in our hospital.
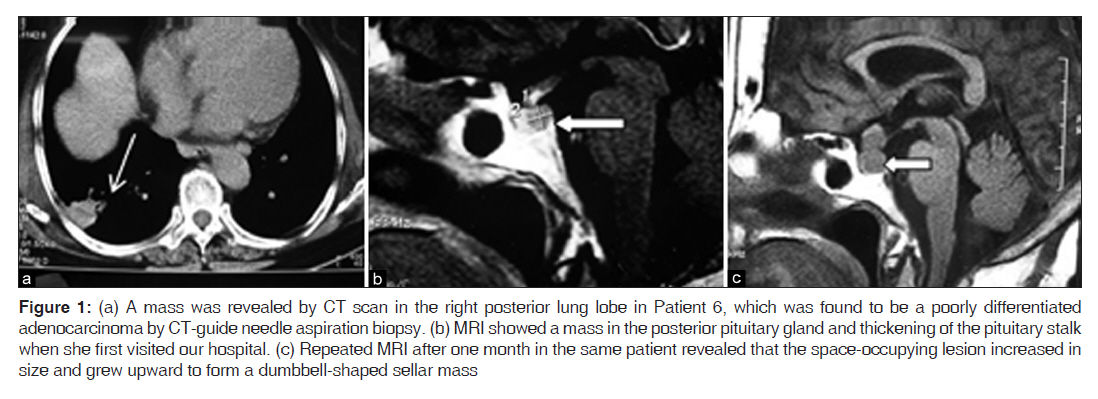
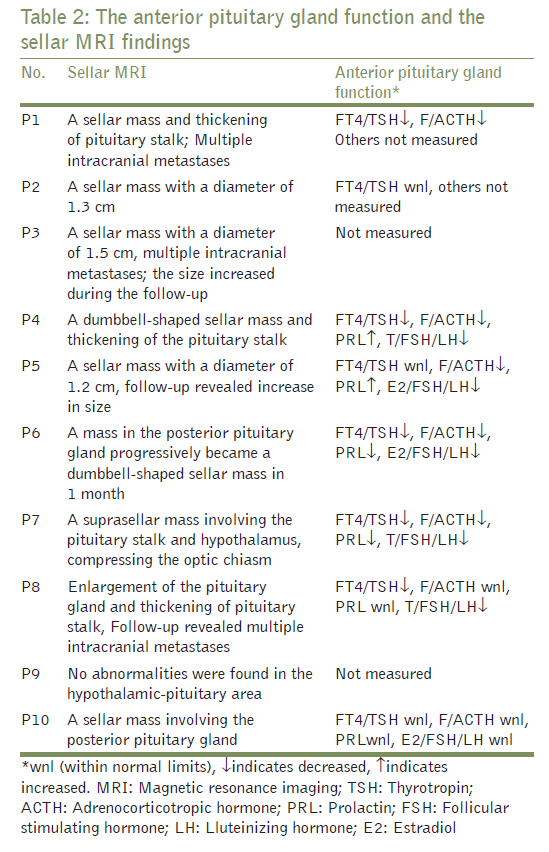
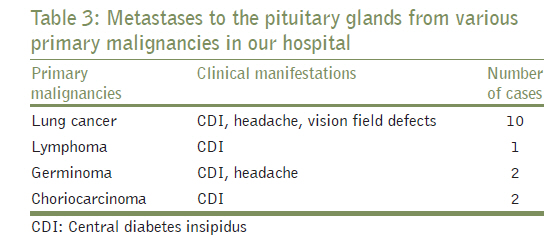
General demographic features A total of 1 639 patients with lung cancer were admitted to our hospital between January 1998 and December 2008. Ten of them (0.61%) had CDI as their first manifestation. During the same period, 306 patients were diagnosed as CDI; hence, the incidence of lung cancer metastasis-induced CDI was 3.27%. Their average age was 58.6±7.8 years (range from 37 to 71 years) and half of them were males. Presenting symptoms and signs Sudden onset of polyuria and polydipsia were the primary manifestations in eight patients. The symptoms started 3.2±1.2 months (from 2 weeks to 6 months) before the diagnosis of lung cancer. The main clinical features are summarized in [Table - 1]. Patient 3 had progressive visual field defects after the diagnosis of lung cancer. Patient 4 presented with a hyperosmotic coma with his serum sodium of 167 mmol/l, suggesting that the PM simultaneously had invaded the posterior pituitary gland and the thirst center. Patient 9 was diagnosed with CDI 4 years before the diagnosis of lung cancer. To our surprise, no abnormalities were found in sellar MRI. Other chief complaints in these patients were headache (5/10) and hemoptysis (1/10). Diagnostic procedure for lung cancer Lung cancers were diagnosed by chest imaging and pathological biopsy. The masses could be readily seen in chest CT images [Figure - 1] in all patients, whereas in four patients, no abnormalities could be found in their chest X-ray plain films. Patient 3 turned out to be a differentiated adenocarcinoma after operation. Then, an open-brain surgery, aiming at restoring her visual field, found that the pathology of sellar mass was identical to the primary lung cancer. Patient 8 had a diagnosis of poorly differentiated adenocarcinoma by fibrous bronchoscopy biopsy. Characteristics of sellar magnetic resonance imaging All patients had sellar masses in their MRI, except Patient 9 who had no obvious space-occupying lesions or thickened stalk in hypothalamus pituitary region. The high bright signals of posterior pituitary lobe in T1-wighted MRI were all lost in the patients. In five patients, the sellar masses appeared like dumbbells and larger than 1 cm in size. During the follow-up, the size of masses increased in Patients 3, 4, 5, 6, and 8. As an exception, Patient 9 had no obvious abnormalities in sellar MRI from the beginning to the end. Hormone secretion from anterior pituitary gland We evaluated the levels of hormones secreted from the anterior pituitary gland in seven patients. Six of them had panhypopituitarism [Table - 2]. The other three patients did not have their hormones measured and no obvious symptoms and signs of hormone deficiency were manifested. Patient 4 had hyponatremia which returned to normal after administration of glucocorticoids. Management and outcomes Nine patients died, with a median survival period of 5.6±2.2 months (from 3 to 13 months). Eight patients received systemic chemotherapy. Some patients also received adjuvant treatments, such as thoracotomy operation, intrathecal chemotherapy, and sellar irradiation [Table - 1]. Patient 3 suffered from a progressive visual field loss after open lung surgery and the decompression surgery on optic chiasm partially restored her visual capacity. Whole-body PET scan for Patient 10 revealed that only the pituitary gland and the right lung lobe had enhanced glucose metabolism. An open lung radical surgery was performed, followed by sequential multiple systemic chemotherapy and sellar radiotherapy with a total dose of 5 000 cGy. She has been alive for 3 years without any signs of tumor recurrence. Discussion Our data showed that the incidence of PM caused by lung cancer was 0.61% in our hospital, which is a tertiary academic hospital. The incidence might have been underestimated because only those patients with CDI as their first symptoms were included in our retrospective study. One review analyzed 380 cases with PM and found that breast cancer (39.7%) and lung cancer (23.4%) were the most common primary malignancies. [1] Other less common primary malignancies include the tumors from gastrointestinal tract, kidney, and leukemia. [1] In our hospital, the other five PM cases were caused by lymphoma, germinoma, and choriocarcinoma [Table - 3]. Our findings are remarkable because 10 of 15 of cases with PMs were caused by lung cancer, but not by breast cancer, whereas other reports showed that breast cancer was the most common primary malignancy for PMs. In our hospital, more than 400 cases of breast cancer were diagnosed per year, but no PM has been documented. It was presumed to be caused by the following reasons: (1) The breast cancer metastasis appears to have a higher affinity for the adenohypophysis, and the symptoms of hormone deficiency are not easy to be detected; [2] (2) The detection and treatment of breast cancer in early stage, especially with the use of aromatase inhibitors, significantly decreases the possibility of distal metastases to the pituitary; and (3) Ethnic variation may have an influence on MPs caused by breast cancer metastasis. [8],[9] CDI is a disease involving lack of arginine vessopressin caused by impairment of neurohypophysis, pituitary stalk, and hypothalamus. Polyuria and polydipsia are the chief complaints; hence, the patients usually first visit the endocrinologists. Local inflammations, traumas, and tumors such as craniopharyngioma, germinoma, and meningioma are the main pathologies for CDI. However, the differential diagnosis of CDI is far beyond this scope and PM should come into consideration when the underlying etiologies are not determined. [10] It is taken for granted that pituitary adenomas are the dominant causes for CDI. In fact, only 1% of them are large enough to block the pituitary stalks and cause CDI. However, metastases to the pituitary glands would directly invade the posterior pituitary lobe, resulting in diabetes insipidus at early times. [11] It is difficult to detect lung cancer in its early stage. In some patients, it is the distant metastases, not the respiratory symptoms, which lead to the final diagnosis. [3] In such a circumstance, CDI might be the first and only clue to the diagnosis of lung cancer. In our patients, polyuria and polydipsia were their first symptoms leading them to the endocrinologists. Only Patient 1 showed hemoptysis with polyuria. The other nine patients did not have any respiratory symptoms even after the diagnosis was made. Therefore, the extrapulmonary symptoms are important and the PMs from lung cancer should be considered when common etiologies for CDI have been excluded. [12] PMs impair the hormone secretion from anterior pituitary glands by compression or by blocking pituitary stalks, and the latter will increase the serum PRL levels. [11] An analysis including 201 patients with PMs showed that 50.6% of PMs involved the neurohypophysis alone, and 15.4% infringed adenohypophysis alone, and 33.8% destroyed both the anterior and posterior pituitary glands. [2] In our patients, 6/10 cases had confirmed impairment of adenohypophysis. Lung cancer mainly metastasizes by lymph node invasion or hematogenous spread. [13] The neurohypophysis is directly supplied by the posterior pituitary artery. Such an anatomic structure would well explain why PMs would damage the neurohypophysis and the hypothalamic infundibulum more directly than the adenohypophysis. Accordingly, this may also explain some imaging characteristics of PMs in the sellar MRI: Cancer cells are transported to the posterior lobe directly by systemic circulation. This infiltration will grow up forward and upward [Figure - 1]b, breaking through the sellar diaphragm. Finally, a dumbbell-shaped mass would come into being [Figure - 1]c. Therefore, dumbbell-shaped sellar masses in MRI are prone to the diagnosis of PMs. [2],[14] Other diseases, such as germinoma, craniopharyngioma, and Rathke′s cyst, may also manifest as dumbbell-shaped mass and CDI, but they often happen in children and young adult. Large pituitary adenoma also looks like dumbbell, but it grows up slowly, taking several months or years to break through the sellar diaphragm and seldom causing CDI. In our series of patients, polyuria as the first clinical presentation also indicates this transferring route of PMs. However, to our surprise, Patient 9 had no visible sellar mass in MRI and had a normal chest CT scan when he just had the symptoms of CDI. Four years later, he was diagnosed of lung cancer with multiple metastases. We deduced that his CDI was caused by the lung cancer metastasis or small tumor embolisms, considering the rarity of these two clinical conditions, but the accurate underlying mechanisms were not clear. The pathologies of our patients were adenocarcinomas and small-cell lung cancers, not squamous carcinomas. This is consistent with the other reports and indicates that adenocarcinomas and small-cell lung cancer are more prone to metastasize by blood vessels. [5],[6],[14] The effective treatments for PMs with lung cancer are limited. [1],[10] The patients are almost all in advanced stages when the diagnoses are made. Tumor resection surgery, systemic chemotherapy, sellar radiation therapy, [15] optical chiasm decompression operation, [10] and intrathecal chemotherapy are the main choices. Hormone replacement and desmopressin may help to improve quality of life. Therapeutic regimens in our patients are listed in [Table - 2]. Generally speaking, the malignancies might have had multiple metastases when PMs happen. However, in Patient 10, the MP was the only extrapulmonary metastasis confirmed by PET scan. After a pulmonary lobectomy, sequential systemic chemotherapy, and sellar irradiation, she has lived for more than 3 years and is still alive without any signs of recurrence. In summaries, systemic malignancy should be taken into consideration when the endocrinologists come across an elderly patient with new-onset CDI. A chest CT and a sellar MRI are necessary and a dumbbell-shaped masses in MRI are prone to the diagnosis of PMs. Multiple comprehensive therapeutic regimes, including tumor section, systemic chemotherapy, sellar decompression operation, local irradiation, hormone replacement, and desmopressin may prolong the survival and improve the life qualities. Acknowledgment The first two authors contributed equally to this work. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11086f1.jpg] [jp11086t2.jpg] [jp11086t3.jpg] [jp11086t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}