 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 307-313 Review Article Tuberculosis and female reproductive health K Ghosh1, K Ghosh2, JR Chowdhury3 1 National Institute of Immunohaematology, 13th Flr., KEM Hospital, Mumbai, India Date of Submission: 05-Jan-2011 Code Number: jp11087 PMID: 22120860 Abstract Tuberculosis (TB) is an important cause of mortality and morbidity all over the world and is particularly relevant in developing countries like India where the disease is endemic. Female reproductive system is very vulnerable to this infection and clinical presentation of this disease in female reproductive tract is protean in nature and in a large majority of patients could be completely silent. This disease is an important cause of infertility, menstrual irregularity, pregnancy loss, and in association with pregnancy, morbidity to both the mother and child increases. Some of the effects of TB infection on female genital tract could be remote in nature due to infection elsewhere. Medicines used to treat TB infection can also have adverse effects on contraception and other areas of female reproductive health. HIV coinfection and multidrug-resistant tuberculosis (MDR-TB) and increased population migration from developed to developing countries have now added a whole new dimension to this infection. Though new, finer diagnostic tools of detection of TB are increasingly available in the form of bacterial cultures and polymerase chain reaction (PCR) based diagnostics, suspicion by clinicians remains the main tool for diagnosis of the condition. Hence, doctors need to be properly trained to become "Tuberculosis Minded". Keywords: Endometritis, fetal loss, human immunodeficiency virus infection, hormonal imbalance, menorrhagia, multidrug-resistant tuberculosis, synecheae, tuberculosis Introduction Tuberculosis (TB) is the second leading cause of death worldwide amongst communicable diseases. It kills nearly 2 million people each year mostly in the developing countries. [1] However, TB has a more devious face where it chronically cripples different systems of the body without necessarily killing the patients. Some of the chronic presentations of the infection may resemble other diverse disorders, and diagnosis of TB with such an invidious presentation of deeper tissue infection is extremely difficult. In many parts of the developing world, antitubercular drugs are often given on strong clinical suspicion of TB. TB directly and indirectly affects female reproductive health and clinically can present in different ways to tax the ingenuity of the best diagnosticians. In this review, we are presenting the protean behavior of tubercular infection on female reproductive health. Methodology of Review Process We searched PubMed/Medline with following heads: "Tuberculosis and Pregnancy Loss", "Female Genital Tuberculosis", "Menstrual Disorders and Tuberculosis", "Tuberculosis and Infertility", "Endometrial Tuberculosis", "Multidrug-resistant tuberculosis (MDR-TB) and pregnancy", "Pregnancy outcome and TB". Database between 1980 and 2009 was searched. We limited our search to English literature only. After going through the title of the papers, individual case reports were excluded. Case review involving more than 10 cases were included. Epidemiology and prevalence papers were included. Subsequently, we read PubMed Abstracts in 214 articles and used and read full 56 papers. We also searched Indian Indexing Software Medline for the Journal of Obstetrician and Gynecology. The review is the result obtained from these sources. Prevalence in Developing and Developed Countries In 2006, worldwide, 9.2 million new cases of TB were diagnosed, with 1.7 million deaths in Asia and sub-Saharan Africa, accounting for 84% of the cases. [2] There is a significant total difference in TB rate between individuals born in the USA and those who are immigrating to that country (2.1/10 5 immigrated population). [3] Estimates have been adequately presented by Frieden et al. [1] in [Figure - 1] of their article. Hence, it is not unusual that major reports on the effects of TB on pregnancy outcome and reproductive health have come from developing countries, mostly in the form of isolated case reports. Various studies show genital TB as a cause of infertility to be present in 1-17% of the cases, around 1% in the developed countries and 18% in India. [4],[5] Mycobacterium tuberculosis is the commonest cause of human TB, accounting for more than 99% of the cases in UK. [6] The highest rates of TB infection are reported in London (46.3/10 5 population). Majority of such patients were born abroad and are between 15 and 44 years (reproductive age group). In Africa, TB ravages the country with an incidence of 290/10 5 population, followed by South East Asia where TB accounts for 194/10 5 population. Globally, the new infection is rising by 1.8% per year. [7] Generally the M. tuberculosis gains access through respiratory passage in lungs and then disseminates to different organs via lymphatic drainage and blood circulation. Female genital tract is also an important site in this dissemination process. Once the immunity to M. tuberculosis contains and overrides the growth of small number of disseminated TB bacilli after primary infection, the infection may remain silent throughout the life until lowered immunity or overwhelming re-infection precipitates the disease. [8] Increased circulation, hormone dependence of female genital organs after sexual maturity may in part explain why the genital system is vulnerable to this infection after sexual maturity. [9] Presently, one of the greater concerns is the evolution and increased prevalence of drug-resistant TB across the globe. Resistance to two first-line drugs like Isoniazid (INH) and Rifampicin is called MDR-TB, and when in addition to these drugs, the disease is also resistant to Fluroinolone and second-line injectable drugs, the disease is called extended drug resistant TB. Worldwide, 9.9% of the cultured bacteria are resistant to first-line drugs and 1.4% are MDR-TB. MDR-TB is now prevalent in former Soviet Union, South Africa and China. [10],[11] Smear-positive and culture-positive pulmonary TB in India is observed in 100-160/10 5 population and 100-250/10 5 population, respectively, and the proportion of new MDR-TB is also not insignificant at 0.5-5.3% and in previously treated case. [12] MDR-TB is present at an alarming rate of 8.67%. [3] The problem of extensively drug-resistant TB (XDR-TB) is emerging very fast and is spreading all over the world including India. [13],[14] This is important with respect to TB with pregnancy where many of the second-line drugs are teratogenic and need to be prescribed with great caution and the outcome of the treatment with best of the regimens is suboptimal. The consequences of all kinds of tubercular infection on female reproductive health may lead to the following:
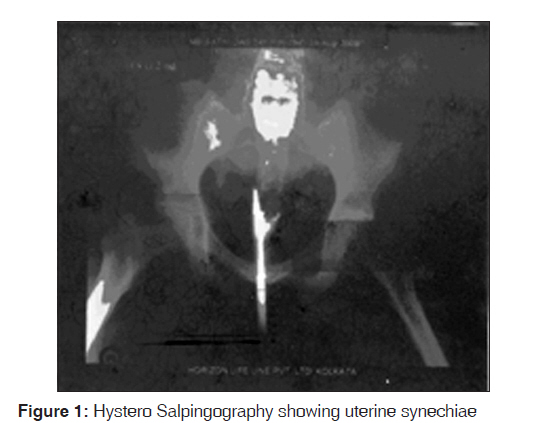
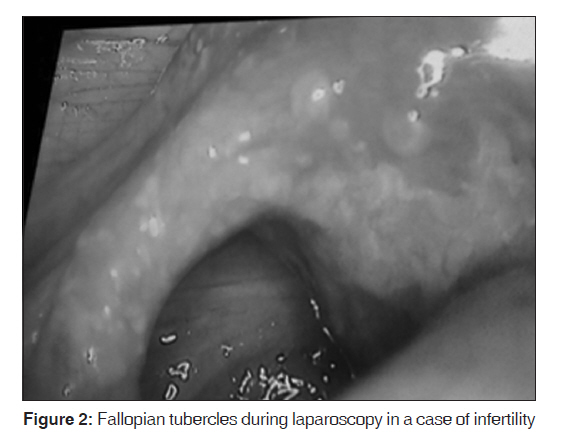
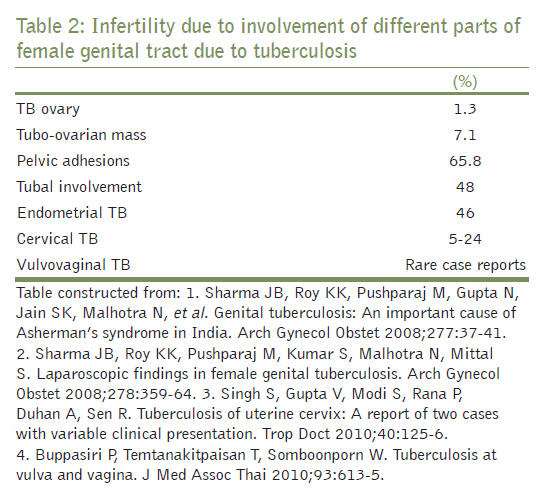
We will be discussing some of these facets of TB in this review TB associated with disordered menstruation Any disease which causes substantial weight loss and is associated with systemic inflammatory response and cachexia can cause amenorrhea. Hence, it is not surprising that advanced extragenic TB can cause amenorrhea. Similarly, on rare occasions when TB affects adrenal gland (used to be one of the common causes of Addison′s disease in the past), pituitary gland and ovaries, [15] disordered menstruation, particularly amenorrhea, is a distinct possibility. However, hypomenorrhea or amenorrhea has been described in a substantial number of patients with extragenital pulmonary TB in case control studies. [16] This finding has also been corroborated by other studies. [17] Why non-genital TB should cause menstrual disturbance is not known with certainty, but hormonal changes which can affect menstruation have been observed in these patients [18] and anti-gonadotrophic effect of M. tuberculosis has been demonstrated in the experimental set-up. [19] Tripathy et al. have shown that 13% of pulmonary TB patients have endometrial involvement. Schaefer [4] opined that all cases of amenorrhea due to TB probably originate due to endometrial involvement. One of the antitubercular drugs, "Rifampicin", has been shown to induce menstrual disturbances. [20] Hence, antitubercular therapy adds other dimensions to the cause of amenorrhea in this condition. Rifampicin-induced increased enzymatic catabolism of estrogens may affect Luteinizing Hormone surge, resulting in an ovulating cycle. Case reports have mentioned amenorrhea to be not infrequent after anti-TB therapy. [21],[22] Though menorrhagia is uncommon, this can follow when TB causes tubo-ovarian mass or Following an ovulatory cycle i.e., the cycle in which ovulation occurs when the period is likely to be heavy. [23] Menstrual disturbances are more likely when female genital tract is involved in tubercular process. [4] The disease most commonly affects fallopian tubes (92-100%), ovaries (10-30%), endometrium (50%), cervix (5%) and rarely vagina or vulva (<1%). [4],[24],[25] In a series of 120 patients with genital TB, Samal et al. [26] showed oligomenorrhea in 54%, menorrhagia in 19.0%, amenorrhea in 14.3% and postmenopausal bleeding in 1.6% of cases. Tubo-ovarian mass was detected in 19.8% of cases. Similar prevalence of menstrual disturbance has been described by other authors. [4],[9] Uterine synechiae is also an important cause of secondary amenorrhea associated with TB. [27] TB and pregnancy It is generally believed that pregnancy does not influence the course of pulmonary or extrapulmonary TB. [28],[29] But there are some reports of the aggravation of the condition during pregnancy. [30] In advanced countries when TB is diagnosed early and treated, TB rarely influences the outcome of pregnancy. [31] However, the same cannot be said for a vast majority of the population in developing countries where 90% of TB occurs and pregnant woman with TB often presents late to the Gynecologist for management. Moreover, in some countries, MDR-/XDR-TB increasingly involves pregnant woman and this disease with or without concomitant HIV infection immensely complicates the management of the cases. In developing countries, prevalence of TB parallels its prevalence in the general population and kills more women of reproductive age than all the combined causes of maternal mortality. [32] Incidence of TB with pregnancy in certain ethnic groups in London approaches 1%. [33],[34] TB in pregnancy can present as pulmonary or extrapulmonary TB. In two UK studies, [33],[34] 53% and 77% of pregnant women were reported to have extrapulmonary TB similar to that reported in a Mexican study, [35] though case control studies from India and USA both reported lower (9% and 13%, respectively) rates of extrapulmonary disease. [36],[37] Early diagnosis of TB may be difficult when associated with pregnancy as it may mimic some of the physiological changes that occur during pregnancy, i.e. increased respiratory rate fatigue, [30] cough (74%), weight loss (41%), fever (30%). Malaise and fatigue (30%) was found to be a common presenting manifestation of TB with pregnancy. [28] It can be easily seen that except weight loss (which to some extent can be compensated by weight gain during pregnancy), none of the other symptoms can warn the caregiver that they may be dealing with associated TB. TB test also has its higher pitfalls and fallacies when used during pregnancy; early studies showed false-negative skin tests, [38] whereas later, more tightly controlled studies with adequate controls suggested that pregnancy may not measurably affect the response to TB skin test. [39] Moreover, in those areas of the world where TB is common and BCG vaccination is universal, tuberculin test more often confuses than contributes to the diagnosis. One of the important diagnostic tools is chest X-ray and this is usually avoided during pregnancy. Maternal complication rates with both pulmonary and extrapulmonary TB are increased and include pregnancy associated hypertension (8.6%), respiratory failure (5.8%) and oligohydramnios (2.9%). Relative risk of overall maternal complication was 3.1 and preterm labor was increased eightfold. [35] Higher frequency of toxemia, abortion and intrapartum complications has also been reported. [40] Studies conducted in the North Indian city of Chandigarh showed increased complication rate similar to that described above (except in lymph node TB) in both pulmonary and extrapulmonary TB. [41],[42] Fetal growth retardation was noted in several studies. [33],[35],[41],[42],[43] In the North Indian study, for cases with pulmonary TB, the risk of babies small for gestational age was 2.6 (P<0.005) and occurred in 20.2% of cases, [42] whereas among patients with non-lymph node extrapulmonary TB, 33% babies were of low birth weight (P<0.01). Average difference in birth weight between babies born to mother with pulmonary TB and controls was 215 g (P<0.0001) [41] and for extrapulmonary cases it was 251g. Overall incidence of perinatal mortality is high where TB has affected pregnancy. The rates were 10% in the North Indian study [41],[42] and 8.6% in the Mexican study. [35] No maternal mortality was reported from different case studies, except one report from Papua New Guinea [43] in which 110 patients of TB associated with pregnancy were studied between 1995 and 1999. 11/40 (26%) patients were not diagnosed to have TB until after delivery. There were six maternal deaths in this study mainly due to pulmonary, meningeal and miliary TB. 45% of the children born were growth retarded and a perinatal mortality rate has been recorded at 137/1000 births. This study shows how the neglected TB with pregnancy can play havoc with both the mother and the newborn baby, whereas studies in developed and developing countries have shown that if the diagnosis is made early and adequate treatment given, there should not be much difference in the outcome of pregnancy with and without TB. [30],[36],[44],[45],[46] It may not be out of place to mention here that active TB of spine can cause deformation of pelvis or obstructed labor. [23] TB of spine can also cause paraplegia and may be associated with delayed progression of labor due to loss of Fergusson reflex. [23] Vaginal delivery is not contraindicated in such cases, but spinal nursing in a patient with rapidly enlarging uterus can pose a challenge. [42],[47],[48] TB itself mimicking pregnancy and pregnancy associated complications Abdominal TB coupled with amenorrhea in females may mimic pregnancy superficially. In modern times when pregnancy tests are extensively available and sonography machines have reached the remote corners of many developing nations, it is unlikely that except superficial resemblance of abdominal distension, pain, amenorrhea of abdominal TB with pregnancy, there is any chance of misdiagnosing abdominal TB with pregnancy. Certain TB related complications with associated pregnancy may mimic pregnancy complications, for example, increased urinary frequency with pyuria of renal TB may mimic urinary tract infection of pregnancy and repeated vomiting during pregnancy may be confused with hyperemesis gravidarum (HG). [42],[49] TB in the neonate A fetus can get TB infection from the mother either through ingestion or aspiration of infected amniotic fluid or from ulcers in the lower genital tract during delivery or by hematogenous spread through umbilical vein to fetal liver via placental TB. [30],[50] True congenital TB seems to be rare, but infection after birth from the mother, particularly if mother has open cavitary TB and has been on anti-TB drug for less than 2 weeks, is more likely. [50],[51] Less than 300 cases of congenital TB have been described in the literature along with the criteria (Cantwell criteria) for confirming fetal/neonatal TB. [52] The criteria comprise demonstrating (i) either primary hepatic complex or caseating granuloma by percutaneous liver biopsy at birth or (ii) the presence of maternal genital tract lesion due to TB or (iii) TB placentitis or (iv) the presence of tubercular infection in the neonate in the first week of life where postnatal transmission has been ruled out by proper investigation of contacts including the attendants. [52] A neonate presenting with TB may present with respiratory distress, fever, poor feeding, lethargy, irritability, abdominal distension, lymphadenopathy or hepatosplenomegaly. These symptoms are nonspecific, and if favorable response is not obtained with broad-spectrum antibiotics and investigation for other congenital infections are negative, then TB should be high on the list. Unusually, chest radiography is abnormal in most of the patients and 50% of such patients have military TB. [45] The overall mortality for neonatal TB is high (38% in untreated and 22% in the treated). [45],[50],[52] TB test results are not helpful in diagnosing TB in the neonatal service; they are always negative in the first 1-3 months in developed countries, [45] but where BCG vaccination is given at birth, it may take another 3-4 weeks before hypersensitivity to TB develops. Once TB is diagnosed, standard treatment with antitubercular drugs may be initiated. INH prophylaxis (5 mg/kg) can be given to exposed neonates, and in developed countries, BCG vaccination may be given at 3 months of age if the child is still tuberculin negative. In India, BCG vaccination is usually given at birth. Hence, if INH prophylaxis is initiated, BCG vaccine should be delayed and given at 3 months if tuberculin test is still negative. Side effects of antitubercular drugs Antitubercular drugs are not without side effects. They can cause a host of symptoms like gastric irritation, neuropathy (if given without vitamin B6), drug fever, thrombocytopenia, neuropsychiatric manifestations, optic neuropathy (Ethambutol) and the most dreaded complication of fulminant hepatitis. Second-line drugs also have many major complications like deafness, convulsion, neuropsychiatric changes, etc. A single study has shown that there is a 2.5 times increased risk of INH related hepatitis and fourfold increased risk of death in Hispanic women treated for TB during pregnancy. [53],[54] This study was largely unconfirmed. [45],[55] However, treatment with first-line drugs during pregnancy is considered safe for both mother and the fetus. [45],[56] Similar experience has also been reported from developing countries. [57] Rifampicin and INH freely cross placenta and Rifampicin has been associated with 4.4% fetal malformation rate. [58] Similarly, Ethambutol is associated with 2.2% malformation rate. [45] Not much data are available about the teratogenic effect of Pyrazinamide. Certain second-line drugs, particularly aminoglycosides, poses a very high risk of fetal deafness. One in six fetuses may be affected; hence, this group of drugs should be avoided in pregnancy. [56] The babies born of mothers taking antitubercular drug are at higher risk of hemorrhagic disease of the newborn and may need additional dosage of vitamin K. [59] All the first-line antitubercular drugs are compatible with breast feeding. [45],[60],[61] Ethionamide, Proethionamide, and Cycloserine should not be used for pregnancy either because of lack of information or possible teratogenic effect. [62] MDR-/XDR-TB associated with pregnancy Recent worldwide increase in MDR-/XDR-TB as described in the beginning of this discussion affects pregnancy and its outcome adversely. Because of the very nature of the disease, second-generation anti-TB drugs, avoiding aminoglycosides, need to be given. Even then, the effectiveness of second-line drugs is only 60-70%, with a large number of drop-out rates due to increased toxicity or resistant disease. However, acceptable fetal outcome has been reported in several small studies. [63],[64] In a larger study conducted on 38 pregnant women treated for MDR-TB, 61% were cured, 13% were dead, 13% defaulted, 5% combined treatment and 5% had resistant disease. Five of the pregnancies terminated in abortion and one was still born (~15.5% fetal loss). Other study with lesser number of patients showed better result with five cured (72%) and with no fetal death or abortion, but long-term effect on the children with second-line anti-TB drug was negligible. [65] However, limited number of studies on MDR-/XDR-TB with pregnancy show that the results are far from acceptable and need further improvement. Infertility and subfertility associated with tb of the genital tract There are a large number of studies attesting to the role of genital TB in subfertility and infertility. [4],[8],[9],[27],[66],[67],[68],[69],[70],[71],[72] Genital TB invariably affects the fallopian tube, and in 50% of the cases of genital TB, endometrium is also involved. [4],[8] It is estimatedthat a large number of infertile women worldwide have genital TB, but this prevalence varies to less than 1% in USA to nearly 18% in India. [4],[66],[67] However, incidence of infertility in genital TB varied from 10 to 85%. [4],[68],[69] Genital TB not only causes tubal obstruction, but also impairs implantation due to endometrial involvement and ovulatory failure from ovarian involvement. [15] In a proportion of cases, synechiae of the uterine cavity can be the cause of infertility. [27],[70] Hysteroscopy and hysterosalpingography [Figure - 1] are two important investigations to evaluate the anatomical abnormality of the female genital tract in infertility and suspected genital TB. The features in hysterosalpingography in cases of genital TB patients presenting with infertility have been comprehensively presented by Chavan et al. [71] TB peritonitis was seen in combination with genital TB in 45-50% patients with genital TB. Extensive adhesion caused by abdominal TB also interfered with successful pregnancy. [66],[67] Successful pregnancy is extremely low in patients with genital TB even after complete treatment of TB. [4],[66],[67],[68] The conception rate in one study was 19.2% and the birth rate was 7.2%. Hence, for many patients, in vitro fertilization and embryo transfer remain the only option for successful pregnancy. However, Bapna et al. [66] evaluated several series including their own for the success rate of such procedures, which varied from 9 to 28% conception rate, and 4.2-30.7% of the conceptions were delivered as live born babies. Ectopic pregnancy rate varied between 3.3 and 10%, showing poor results in cases of in vitro fertilization also. In patients who present with Asherman′s Syndrome (uterine synechiae), the results are poor and surrogacy may remain the only option. [27] Even latent genital TB may be a cause of repeated IVF failure if the disease is not diagnosed beforehand and treated. [72] Review of literature does not allow us to dissect differences in the prevalence of infertility due to different areas of involvement of genital tract because in an overwhelming number, fallopian tube is involved [Figure - 2], making isolated involvement of other parts of female genital tract a rarity. Prevalence of female genital TB as a cause for infertility varies in different parts of the world and in different time periods in the studies were conducted. Summary of the findings is presented in [Table - 1]. However, studies have shown 5-24% patients with genital TB have TB of uterine cervix, of which 50% suffer from infertility. Vulvovaginal TB is generally a rare disease and is usually not associated with infertility. Involvement of other areas of genital tract as a cause of infertility is given in [Table - 2]. Challenges of increased prevalence of TB in immigrant population Immigration has posed an important risk of imported TB for the developing countries. As most of the people who are immigrating belong to reproductive age group, modern physicians in the developed countries are likely to see more patients who present with TB and pregnancy, female genital TB with menstrual disturbances, subfertility and many other complications. In a large proportion of cases, female genital TB is silent and may present as infertility as well as difficulty in conceiving even after In vitro Fertilization-Pre-Embryo Transfer (IVF-ET) techniques. With pregnancy, TB may remain undetected for a longer period of time because of nonspecific symptoms and overlapping symptoms of pregnancy itself. However, reduced fetal growth in minority immigrant population should increase the suspicion for associated TB. TB test was not found to be sufficiently specific or sensitive in detecting genital TB in high prevalence areas like India where the sensitivity of the test was found to be only 55% and specificity 80%. [73] However, TB test was found to be clinically useful in developed countries even during pregnancy. [33],[34],[45],[74] Associated HIV infection is also an important cause for concern. Combination of HIV infection along with TB in pregnancy not only increases the mortality and morbidity of the mother and fetus, but also makes the management of both diseases difficult, [74],[75] and this combination is likely to be seen increasingly in the developing world. A large number of people in the immigrant population in India are from Bangladesh and Nepal and the magnitude of this infection and HIV infection needs to be looked into.
TB is an important cause of reproductive and genital morbidity in women. Increasing migration of population to developed countries from endemic areas of TB has been noted with great concern [1],[2],[3],[5],[6],[7] and appropriate measures are being taken. [76] However, TB, particularly genital TB, remains asymptomatic in many patients and tuberculin test in patients from endemic areas is not highly sensitive to active disease. Hence, alternative methods with improved sensitivity are urgently required. In a suspected case, there are many diagnostic techniques available and they have been discussed adequately elsewhere. [1],[77],[78] Finally, we should understand that TB is a great mimic and may masquerade diverse clinical conditions. One of our revered teacher′s anecdote rings in our ears from the days of undergraduate medicine, "My son tuberculosis can present as everything except a confirmed pregnancy". References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11087t2.jpg] [jp11087f2.jpg] [jp11087t1.jpg] [jp11087f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}