 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
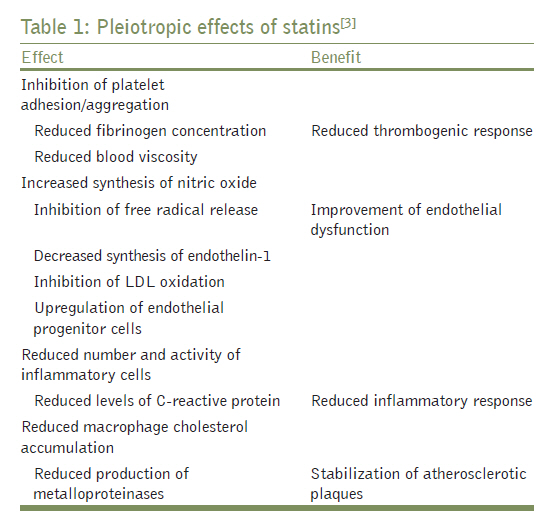
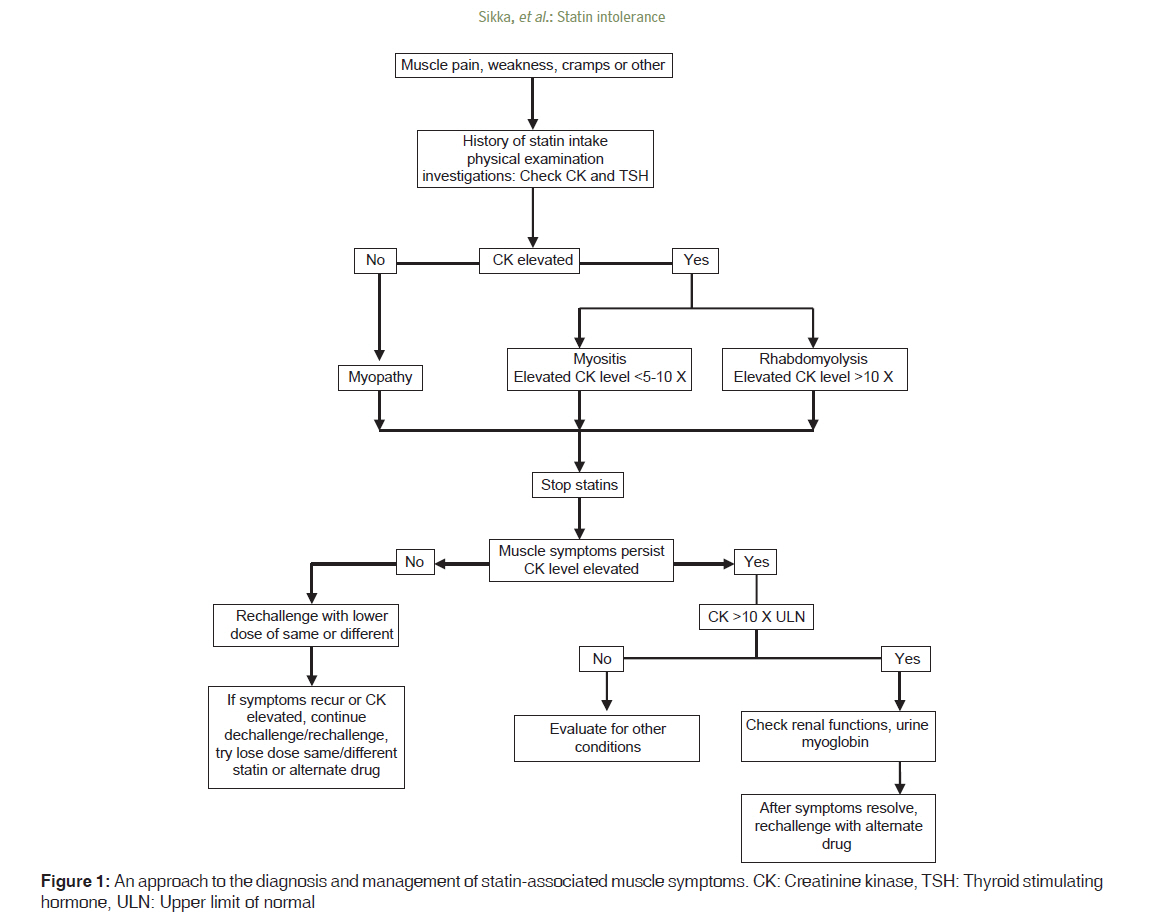
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 321-328 Review Article Statin intolerance: Now a solved problem P Sikka1, S Kapoor2, VK Bindra3, M Sharma1, P Vishwakarma1, KK Saxena1 1 Department of Pharmacology, LLRM Medical College, Muradnagar, Ghaziabad, India Correspondence Address: Date of Submission: 24-Mar-2011 Code Number: jp11089 PMID: 22120862 DOI: 10.4103/0022-3859.90085 Abstract Statins are the most effective and widely used drugs for treating dyslipidemia, a major risk factor for coronary heart disease. These are one of the safest hypolipidemic drugs but many patients are bound to discontinue statins due to their side effects. Hepatotoxicity, myotoxicity and peripheral neuropathy are important out of them. Discontinuation of statins leads to dylipidemia and its grave consequences. Hence, there should be enough strategies for statin intolerant patients, so that they can be saved from these consequences. These side effects can be avoided by the awareness of certain factors viz. potential drug interactions and dose adjustment according to patho-physiology of the patient. Baseline investigations for liver function and muscle toxicity should be done before initiating statin therapy. Here, we are discussing various options for statin intolerant hyperlipidemic patients such as lower and intermittent dosing of statins, alternate hypolipidemic drugs, red yeast rice, supplementation with coenzyme Q10 and vitamin D. A number of hypolipidemic drugs are in trial phases and hold promise for statin intolerant patients.Keywords: Hepatotoxicity, intolerance, management, myopathy, statins Introduction Hyperlipidemia is a major cause of atherosclerosis and associated conditions, such as coronary heart disease (CHD), ischemic cerebrovascular diseases, and peripheral vascular diseases (PVDs). It is estimated that an average of 11.5 years of life are lost as a consequence of having CHD. This underlines the importance of dyslipidemia as a risk factor which led to the development of hypolipidemic drugs. With the advent of highly efficacious hypolipidemic drugs, namely, statins, the CHD events, and finally, total mortality have reduced. [1] However, after the prolonged use of statins, many side effects are reported to occur forcing the discontinuation of the drug, and hence, recurrence of dyslipidemia. Here, efforts are made to discuss statins comprehensively including their adverse effects and their solutions by various strategies. Statins Statins, the most efficacious hypolipidemic drugs, are competitive inhibitors of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, which catalyzes the rate limiting step in cholesterol biosynthesis. [2] Therapeutic Uses Because the mevalonate metabolism generates a series of isoprenoids, vital for different cellular functions, from cholesterol synthesis to the control of cell growth and differentiation, HMG-CoA reductase inhibition has beneficial pleiotropic effects [Table - 1]. [3] Statin-related adverse effects Out of various adverse effects of statins, only liver- and muscle-related toxicity is consistently reported. [4] It must be stressed that about 10 years back, Bayer voluntarily withdrew cerivastatin from the world pharmaceutical market, after 31 patients died by rhabdomyolysis. Adverse effects on muscles Between 1987 and 2001, the FDA recorded 42 deaths from rhabdomyolysis induced by statins, i.e., one death per million prescriptions (30-day supply). Although 5-10% of patients complain muscle symptoms, but only 1-3% are actually statin related. Muscle symptoms usually occur within first 6 months of starting statins but can occur months or years after the initiation of statin therapy [5] which automatically resolve within 2 months of discontinuing statin therapy. Muscle symptoms are mainly categorized as myalgias, myopathy, or rhabdomyolysis. These are categorized according to the severity of symptoms and presence of creatinine kinase (CK) elevation. Myalgia is described as stiffness, heaviness, cramping, or weakness that may be persistent, intermittent, or occur only during exertion without CK elevation. [5] Myopathy refers to the presence of muscle symptoms with CK elevation (typically 10-fold higher than the upper limit of normal [ULN]). Symmetrical proximal muscle symptoms are most common, first in the arms and thighs and then in the entire body. [6] Rhabdomyolysis refers to the CK level >10,000 U/L, usually with renal compromise and urinary myoglobin. The incidence of statin-associated myopathy (SAM) is quite low (~0.01%) and rhabdomyolysis is rare (0.002%) but the risk of myopathy and rhabdomyolysis increases in proportion to plasma statin concentrations. [7] Consequently, factors inhibiting statin catabolism are associated with an increased myopathy risk, including advanced age (especially >80 years of age), hepatic or renal dysfunction, perioperative periods, multisystem disease (especially diabetes mellitus), small body size, and untreated hypothyroidism. [8],[9] The concomitant use of drugs that diminish statin catabolism is associated with myopathy and rhabdomyolysis in 50-60% of cases. [9] Fatal rhabdomyolysis has been estimated to occur in approximately 1.5 in 10 million prescriptions. [10] Adverse effects on liver Postmarketing surveillance studies of statins revealed that elevations in hepatic aminotransferases are dose related but are mild and unrelated to LDL lowering [11],[12] and most hepatologists no longer consider statins to have any significant hepatotoxicity. Alanine aminotransferase (ALT) is only one of the specific parameters for drug-related hepatotoxicity and its rise to reflect hepatotoxicity could well be interpreted according to Hy′s rule which states that serum bilirubin twice the ULN with ALT more than three times the ULN with all other causes of liver dysfunction excluded indicates drug-related hepatotoxicity. In placebo-controlled outcome trials (as reported in 2003), where 10- to 40-mg doses of simvastatin, lovastatin, fluvastatin, atorvastatin, and pravastatin were compared with placebo, the incidence of ALT elevation more than three times the ULN was found to be 1.3% with test drugs and 1.1% with placebo with no case of liver failure [13] whereas, four large trials of statins have shown no difference in the frequency or degree of deranged LFT between treatment and placebo groups (involving more than 48,000 patients). Interestingly, out-of-range values, which do occur with statin use, eventually return to normal even if the same statin is continued. [14] Although serious hepatotoxicity is rare, 30 cases of liver failure associated with statin use have been reported to the FDA between 1987 and 2000, the rate being about one case per million person-years of use [13],[15] but the occurrence of acute liver failure (ALF) thought to be caused by statins is well below what is now understood as the background rate of idiopathic ALF in the general population. [14] One estimate determined the idiopathic ALF rate to be from 0.5 to 1.0 cases per million, and the incidence of possible statin-induced ALF to be 0.2 cases per million in the United States. [16] No consistent liver biopsy picture from possible statin-related drug injury has emerged, and there are no reports of chronic carriers of drug-induced liver damage from statins. [14] Thus, an increased ALT in this situation should not be considered a pathology, and also, one cannot tell whether statins are involved in ALF because of background noise. There is no evidence that monitoring reduces the rate of hepatotoxicity. [16] Some other studies have reported only insignificant increase in ALT after starting statins. [1],[17] Madhoun and Bader have shown statins to be safe in hepatitis C patients, [18] and Bader and colleagues have shown fluvastatin to have an anti-HCV activity in chronic carriers of HCV in whom treatment with peginterferon/ribavirin had failed. [19] Abraldes and colleagues have extensively investigated simvastatin as an agent to treat portal hypertension. [20] Moreover, there are some reports showing an additional benefit of statins in reducing cardiovascular events in patients with abnormal liver function tests. Other adverse effects Evidences from four cohort studies and case reports suggest that statins cause reversible peripheral neuropathy, but the attributable risk is small (12 per 100,000 person-years). No change in the cognitive function was found in randomized trials of statins in elderly patients. [10] Statins do not appear to influence the risk of cancer. [11] The safety of statins during pregnancy and lactation has not been yet established. [2] Risk factors for statin adverse effects The factors which increase the serum or muscle concentration of statins increase liver and muscle susceptibility for toxicity. The American College of Cardiology/American Heart Association/National Heart, Lung and Blood Institute (ACC/AHA/NHLBI) clinical advisory propose that risk factors can be categorized into patient related and treatment related. Patient-related factors are advanced age, female sex, small body size, multisystem disease (particularly involvement of liver, kidney, or both), hypothyroidism, alcoholism, grapefruit juice consumption (1 qt/day), major surgery or perioperative period, excessive physical activity, history of myopathy while receiving another lipid-lowering therapy, history of CK elevation, family history of myopathy, and family history of myopathy while receiving lipid-lowering therapy. [21] Treatment-related factors are high-dose statin therapy, and interactions with concomitant drugs, such as fibrates, cyclosporine, antifungals, macrolide antibiotics, nefazodone, amiodarone, verapamil and anti-HIV drug-protease inhibitors. [22] Because simvastatin, lovastatin, and atorvastatin are primarily metabolized through the cytochrome P450 3A4 (CYP3A4), [23] and protease inhibitors are potent CYP3A4 inhibitors, so, these statins should be avoided in patients receiving protease inhibitors. [2],[24],[25] Cyclosporine, an inhibitor of CYP3A4 and several membrane transporters, increases the pharmacokinetic area under the curve of statins by 2- to 25-fold, with many reported cases of rhabdomyolysis. [26] Statin dosages in patients receiving cyclosporine should therefore be limited to 5 mg/day for rosuvastatin, 10 mg/day for simvastatin and atorvastatin, and 20 mg/day for lovastatin. [22] Gemfibrozil administration is associated with about a twofold increase in plasma levels of several statins. [27],[28],[29] The adverse effect reporting system (AERS) rate of rhabdomyolysis for the fenofibrate plus statin (other than cerivastatin) combination is about 15 times lower than that for gemfibrozil plus statin (0.58 vs. 8.6 cases per 1 million prescriptions). [30] Thus, gemfibrogil should be cautiously coadministered with statins. Amiodarone dramatically increases plasma levels of simvastatin but not pravastatin [31] and is associated with a relative risk of about 10 for myopathy when combined with simvastatin. [32] Of importance, pravastatin is not metabolized by the CYP450 system and instead undergoes renal metabolism, although fluvastatin and rosuvastatin are primarily metabolized by CYP2C9. [23] These statins may have a lower myopathy risk, especially in the context of polypharmacy. The atorvastatin, pravastatin, and rosuvastatin uptake in hepatocytes is mediated by the organic anion transporter 2 (OATP2). [33],[34] As more than 70% of statin metabolites are excreted by the liver, [35] various drugs inhibiting OATP2 and patients with billiary tract disease are at increased risk for statin toxicity. [2] Doses of rosuvastatin, simvastatin, and lovastatin, which have significant renal excretion, should be reduced whereas atorvastatin and fluvastatin, which have less than 6% urinary excretion, are useful in chronic kidney disease. [6] Genetic contributions to statin myopathy Common DNA polymorphisms in genes encoding CYP450 enzymes, intestinal P-glycoproteins, OATP2, metabolism of coenzyme Q10, and serotonin pain receptors are inconsistently associated with SAM. [32],[36],[37],[38],[39],[40],[41],[42] Recently, a common DNA polymorphism in the SLCO1B1gene, encoding OATP2 is found to be strongly associated with simvastatin-associated myopathy, [32] but this association was not seen in patients with atorvastatin-associated myopathy. [38] A genomewide association study using approximately 300,000 markers in 85 subjects with definite or incipient myopathy and 90 controls, all of whom were taking 80 mg of simvastatin daily as part of a trial involving 12,000 participants, was carried which yielded a single strong association of myopathy with the rs4363657 single-nucleotide polymorphism (SNP) located within SLCO1B1 on chromosome 12 (P=4 × 10 -9 ). [33] Knoblauch et al. discovered, in a case series of three patients, that statins unmask myotonic dystrophy type 2. Some investigators [43] have associated genetic variants in myotubularin-related protein 4 with plasma cholesterol levels, which may be a link between myotonic dystrophy type 2 and lipid metabolism, and some [44] have shown unprecedented somatic instability of the (CCTG)n expansion, with substantial increases of 2000 base pairs over 3 years. The mechanism of somatic instability or the time required for the alteration of muscle histologic characteristics is still not known, but a possible explanation is CCTG expansion by statins. Management of Muscle Toxicity [Figure - 1] describes an approach for the diagnosis and management of SAM. [45] The first step in determining causality is to discontinue the statin. Statin-related muscle symptoms will partially or completely resolve within 2 months of drug discontinuation. Once symptoms have resolved, the patient should be rechallenged with a lower dose of the same or other statin. If muscle symptoms have not begun or at least partially resolved after 2 months, the patient should be evaluated for other contributing conditions. If symptoms recur after rechallenge, the cycle of dechallenge and rechallenge should be repeated with different statins. The ACC/AHA/NHLBI and National Lipid Association (NLA) have issued guidelines for managing SAM. NLA recommends baseline CK levels only in patients with a high risk for myopathy. [46] Meanwhile, the ACC/AHA/NHLBI advise measuring the baseline CK level for all patients before starting statins because asymptomatic CK elevations are common and could affect later clinical decisions. [21] If a patient develops myopathy symptoms while receiving statins, ACC/AHA/NHLBI and NLA recommend serum CK level estimation. The ACC/AHA/NHLBI also advise the measurement of thyroid stimulating hormone (TSH) levels because hypothyroidism can present with same symptoms. [21] For a symptomatic increase in serum CK levels greater than 10 times the ULN or greater than 10,000 IU/L, the ACC/AHA/NHLBI advise immediate suspension of statin therapy. Reinitiation, preferably with a lower dose of statin, is advocated only after CK levels have returned to normal. [21] Meanwhile, among patients with asymptomatic CK elevations 3-10 times the ULN, careful monitoring of symptoms and more frequent CK determinations should be performed. For asymptomatic patients with CK elevations less than five times the ULN while receiving therapy, we should continue to titrate the statin dose to achieve LDL level targets while closely monitoring the symptoms or further serum CK increases, every 3-6 months. For symptomatic patients either with or without CK elevations greater than five times the ULN, or asymptomatic patients with isolated CK elevations greater than five times the ULN but with no other cause identified, we should either discontinue the current statin or decrease its dose and then monitor levels to ensure complete resolution. Once symptoms or CK levels return to baseline, a trial of a different statin may be considered, because about 40% of patients will tolerate another statin [47] especially a statin associated with less risk for myopathy, such as fluvastatin [48] or rosuvastatin. [49] A randomized, double-blind, double-placebo trial recently evaluated the safety and efficacy of 12 weeks of treatment using fluvastatin, 80 mg/day alone, ezetimibe, 10 mg/day alone, or their combination, among statin intolerant patients and found that in patients with previous statin intolerance, fluvastatin alone or with ezetimibe was well tolerated and efficacious. [48] Results of Prediction of Muscular Risk in Observational Conditions (PRIMO) study proved that patients receiving fluvastatin had fewer myopathy symptoms than those receiving lovastatin, simvastatin, or atorvastatin. [50] Also, no case of fatal rhabdomyolysis has ever been reported with fluvastatin. [51] The management of rhabdomyolysis consists of early aggressive hydration. Rhabdomyolysis recovery is usually uncomplicated with adequate supportive care, with the majority of patients recovering completely from acute kidney injury. [52] Furthermore, because a high statin dose is an important risk factor for SAM, rosuvastatin is a better choice because it comparably decreases LDL levels at approximately 50% of the dose of atorvastatin [53] and is metabolized by CYP2C9, which means less drug-drug interactions in cases of polypharmacy. [23] In a prospective, open-label pilot study of 61 statin intolerant patients, rosuvastatin, 5 or 10 mg/day, was given and only 1 patient discontinued treatment because of myalgia; none had CK elevation. Thus, results suggest that low-dose rosuvastatin is safe in patients with statin intolerance. [49] Management of Hepatotoxicity According to United States Food and Drug Administration (USFDA), a baseline LFT should be done before starting statins except lovastatin for which liver-function monitoring is no longer requested for asymptomatic patients without a history of liver disease. Nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, muscle relaxants, numerous other over-the-counter (OTC) and prescription medications, alcohol consumption, and intercurrent illness are other frequent causes of elevated aminotransferases (with 20% of high-ALT patients because of fatty liver and nonalcoholic steatohepatitis [NASH]). Interestingly, the ALT status has improved or normalized after starting statins in fatty liver or NASH patients. [54] Although elevations in ALT or aspartate aminotransferase (AST) less than three times the ULN may occur during statin therapy, such elevations are usually transient, asymptomatic, and do not require interruption of therapy. Statins should be discontinued in cases having unexplained, persistent elevations of aminotransferases more than three times the ULN. Although decompensated cirrhosis, ALF and worsening obstructive biliary disease remain contraindications for statin therapy, low doses of statins can be used with careful monitoring in compensated cirrhosis, chronic liver disease, and partial obstructive biliary disease. [15] Mild to moderate alcohol consumption (up to 1-2 drinks/day) is not a contraindication but statins should be used with caution in patients who consume substantial quantities of alcohol. Statins can be used safely in patients with either nonalcoholic fatty liver disease or NASH. Large trials support statin therapy in patients with cardiac, kidney, or liver transplants. [7] In those who need statins for their hypercholesterolemia, statins may be the most life-preserving therapy in the entire pharmacopeia. In large 5- to 10-year trials, statins prevent about 33% of major cardiovascular events when compared to placebo. In other words, the number needed to treat (NNT) is 3. If statins cause serious liver disease, it may be on the order of 1 in a million. The number needed to harm (NNH) is 1 million. Estimates of patients who fail to receive statins out of fear of hepatotoxicity range from 10% to 30%. Thus, the anxiety over this possible toxic effect causes thousands of patients to suffer fatal cardiovascular events for what, even if the drug-induced liver injury from statins exists, is an extremely rare side-effect. So, we should set a very high bar to establish the possibility of a liver injury, since failure to do good is harming a much larger group of patients. Hence, it would be prudent to think twice before interrupting statin therapy out of fear of hepatotoxicity. Alternate Treatment Plans for Hypercholesterolemia Dyslipidemic statin intolerant patients can be treated using various strategies: (1) decreasing statin dose, (2) nondaily dosing of statins, (3) other hypolipidemic drugs, (4) LDL apheresis, (5) life style modifications, (6) red yeast rice, (7) coenzyme Q10, (8) vitamin D supplementation in deficiency states, and (9) other potential new therapies. Decreasing statin dose Patients usually tolerate lower doses of same or other statins when they are rechallanged with statins. In general, a lower dose of a statin of similar efficacy would be the next choice. An approximate comparable efficacy can be obtained from 5 mg of rosuvastatin, 10 mg of atorvastatin, 20 mg of simvastatin, 40 mg of pravastatin or lovastatin, and 80 mg of fluvastatin. [5] As already mentioned, fluvastatin has been recommended by some experts because of its relatively low incidence of myalgia due to low lipophilicity, which may contribute to its slower rate of passage into muscle cells and thus, less myotoxicity. [6] Nondaily dosing regimens of statins Atorvastatin and rosuvastatin, being longer acting, are useful for nondaily dosing regimens. Alternate day, three times a week, twice a week, and once a week regimens have been tried and results are encouraging. A double-blind, placebo-controlled trial of 35 patients receiving atorvastatin, 10 mg daily, versus alternate day regimen showed LDL cholesterol reductions of 38% and 35%, respectively, without any myopathy. [55] Out of 51 statin intolerant patients, who received rosuvastatin, 5 or 10 mg on alternate days, 80% of patients had no recurrence of myalgia. [56] Once weekly rosuvastatin, 5-20 mg, resulted in a mean LDL cholesterol reduction of 29% among 8 intolerant patients without any incidence of SAM. [57] Thus, nondaily rosuvastatin and atorvastatin seem tolerable and may help lower LDL cholesterol levels in patients with statin intolerance. Other hypolipidemic drugs Other substitute drugs can be ezetimibe, bile acid sequestrants, niacin, and fibrates. Ezetimibe Ezetimibe inhibits the absorption of dietary and biliary cholesterol by blocking transport proteins, Niemann-Pick C1-Like 1 (NPC1L1), at jejunal enterocytes. [53] Ezetimibe reduces the LDL level by 15-20% [58],[59] and triglyceride (TG) levels by 5%, and increases the HDL level by 1-2%. [60] In clinical trials, ezetimibe used alone or in combination with a statin, does not increase the risk of myopathy. When used alone, ezetimibe does not increase liver aminotransferase levels, and to date, no cases of liver failure, liver transplantation, or death have been reported with ezetimibe but questions have been continuously raised about its cardiovascular benefits. So, it seems reasonable to consider ezetimibe as an option in statin intolerant patients. Bile acid sequestrants Bile-acid sequestrants or resins (cholestyramine, colestipol, and colesevelam) bind bile acids in the intestine, thereby preventing the enterohepatic recirculation of cholesterol. As a result, the hepatic cholesterol content declines, stimulating the production of LDL receptors which leads to increased LDL clearance, and thus, low LDL levels. In Coronary Primary Prevention Trial, cholestyramine reduced total cholesterol by 13%, LDL by 20%, and CHD events (fatal and nonfatal) by 19%. Colesevelam has greater specificity for bile acids, and thus, has less drug interactions and gastrointestinal adverse effects as compared to cholestyramine and colestipol. Recently, colesevelam has also been shown to decrease hemoglobin A1c by about 0.5% in patients with diabetes. [61] Niacin Niacin inhibits the lipolysis of TG by hormone-sensitive lipase, thereby decreasing hepatic TG synthesis. Also, in the liver, niacin reduces TG synthesis by inhibiting both the synthesis and esterification of fatty acids. Niacin reduces TG by 35-50% and LDL by 25%, and increases the HDL level by 15-30%. Side effects include flushing, dyspepsia and hepatotoxicity, and caution is advised in diabetes patients. [62],[63],[64] Fibrates Pharmacological actions of fibrates (gemfibrogil, fenofibrate, benzafibrate, and ciprofibrate) are mediated by their interaction with peroxisome proliferator-activated receptor alpha (PPARa). [63] Fibrates decrease TG levels by up to 50% and LDL by 15-20%, and increases HDL by 15%. Most of the fibrates have potential antithrombotic effects, including inhibition of coagulation and enhancement of fibrinolysis. These salutary effects could also alter cardiovascular outcomes by mechanisms unrelated to the hypolipidemic activity. [66] LDL apheresis It is a procedure, resembling dialysis, to eliminate LDL from the blood stream. Multiple clinical studies have confirmed its effectiveness and have demonstrated an average reduction in LDL by 60%. [67] LDL apheresis may be considered necessary when patients have failed 6-months trial of dietary therapy with maximum tolerated combination drug therapy and meet one of the following criteria: 1) homozygous familial hypercholesterolemia (LDL >500 mg/dL), 2) heterozygous familial hypercholesterolemia with LDL ≥300 mg/dL, 3) heterozygous familial hypercholesterolemia with LDL ≥200 mg/dL and documented coronary artery disease which includes a history of myocardial infarction, coronary artery bypass surgery, percutaneous transluminal coronary angioplasty or alternative revascularization procedure, or progressive angina documented by exercise or non-exercise stress test. [68] Life style modifications All patients who meet the criteria for lipid-lowering therapy should receive instructions about therapeutic life style modifications. The National Cholesterol Education Program (NCEP) Adult Treatment Panel III supports two complimentary approaches: One is population-based approach, which includes increasing exercise (to expend ~2000 calories/week) and dietary recommendations - reduce total calories from fat to less than 30% and from saturated and trans fats to less than 7%; consume less than 300 mg of cholesterol per day; eat a variety of oily fish twice a week [69],[70] and oils/foods rich in a-linolenic acid (canola, flaxseed, soybean oils, and walnuts); and maintain desirable body weight. The second is the patient-based approach that focuses on lowering LDL levels as the primary goal of therapy. [69],[71] Dietary restrictions include less than 7% of calories from saturated and trans fatty acids, up to 10% of calories from polyunsaturated fat, and total fat calories ranging between 25% and 35% of all calories. Weight loss of 4.53 kg can lower the LDL by 5-8%. Low-fat, low-carbohydrate, plant-based diets may provide an additional 5-10% LDL lowering over high-carbohydrate, low-fat diets. [72] So, patients having an unfavorable lipid profile may benefit from consultation with a dietitian. Red yeast rice Red yeast rice is a dietary supplement and has been used in various trials as an alternative to statins. The first randomized, double-blinded, placebo-controlled trial to evaluate red yeast rice in 62 patients with a history of SAM was done by Becker et al., using red yeast rice 1800 mg twice daily for 24 weeks, which significantly decreased LDL (11 mg/dL at 12 weeks and 15 mg/dL at 24 weeks) and total cholesterol levels compared with placebo without increasing the incidence of myalgias. [73] Another study compared a regimen of life style changes with red yeast rice (1200-1800 mg twice daily, depending on the baseline LDL) and fish oil to 40 mg of simvastatin. [74] LDL reductions of 40% were observed in both the red yeast rice and simvastatin groups. This shows that red yeast rice may be a treatment option for dyslipidemic statin intolerant patients. Coenzyme Q10 Coenzyme Q10 is a compound central to the process of making energy within mitochondria and quenching free radicals. Statins block the pathway of the production of coenzyme Q10, thereby causing loss of cell energy and increased free radicals. Furthermore, DNA polymorphisms involving genes for coenzyme Q10 has been proven to be associated with SAM. So, coenzyme Q10 should be added as cotreatment with statins but further studies are needed for its role in statin intolerant patients as results of recent randomized trials are somewhat conflicting. Vitamin D supplementation in deficiency states Myalgias are generally the first manifestation of vitamin D deficiency. Lee et al. proposed SAM to be related with vitamin D deficiency, and repletion of vitamin D levels predictably improves or resolves SAM. [75] There are only anecdotal reports and nonrandomized studies to date, and thus, randomized clinical trials are needed to further evaluate its safety, efficacy, and dose and dosing schedule in statin intolerant patients. Potential new therapies Apolipoprotein B-100 (apoB-100), the principal apolipoprotein of LDL, is associated with increased cardiovascular disease risk. Crooke et al. hypothesized that the suppression of apoB-100 mRNA by an antisense oligonucleotide would reduce LDL. The lead apoB-100 antisense compound, ISIS 147764, reduces apoB-100 mRNA levels in the liver and serum apoB-100 levels in a dose- and time-dependent manner. It decreases total cholesterol and LDL levels by 25-55% and 40-88%, respectively. It does not produce hepatic steatosis or elevate plasma aminotransferase levels. [76] These findings, as well as those derived from interim phase I data with a human apoB-100 antisense drug, suggest that antisense inhibition of this target may be an effective approach for the treatment of dyslipidemia. Mipomersen, an approved antisense drug, given in a randomized placebo-controlled trial, reduced the LDL level by 24.4-31.6% compared to 3.3% in the placebo group. [77] Microsomal transfer proteins play an important role in the lipidation of apoB and in the formation of chylomicrons and very low density lipoproteins. Lomitapide, the microsomal TG transfer protein inhibitor, has entered phase III study in 2007. It has been shown to reduce LDL by 35% as monotherapy and up to 66% in combination with atorvastatin but it led to elevated aminotransferase levels and fat accumulation in the liver in phase II study. [78] The development of the cholesterol ester transfer protein (CETP) inhibitor torcetrapib has been halted due to idiosyncratic blood pressure elevation; clinical trials evaluating other CETP inhibitors anacetrapib and dalcetrapib continue. Anacetrapib lowers LDL by 15% and increases HDL by about 40%. [79] Mutations in the proprotein convertase subtilisin/kexin type 9 (PCSK9) protease gene, which prevent the degradation of LDL receptors, are associated with lower lifetime levels of LDL. [80] Clinical studies have not yet initiated.
Dyslipidemic patients on statins face various adverse effects including hepatic and muscle toxicities. These side effects can be avoided by the awareness of risk factors such as drug interactions and dose adjustment according to physique and physiology of the patient. Baseline liver function and CK levels should be obtained in patients accordingly. Various other causes of aminotransferase and CK level elevations should be ruled out before blaming statins. Intermittent low-dose statins is a better option for statin intolerant patients. Further, alternate hypolipidemic drugs and supplementation with coenzyme Q10 and vitamin D can also be done in addition to life style modifications. A number of hypolipidemic drugs are in trial phases and hold promise for statin intolerant patients. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11089f1.jpg] [jp11089t1.jpg] |
| |||||||||

{kind=link}
{kind=link}