 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 329-331 Case Report Neuralgic amyotrophy associated with dengue fever: Case series of three patients R Verma, P Sharma, N Khurana, LN Sharma Department of Neurology, Chhatrapati Shahuji Maharaj Medical University, Lucknow, Uttar Pradesh, India Date of Submission: 29-Dec-2010 Code Number: jp11090 PMID: 22120863
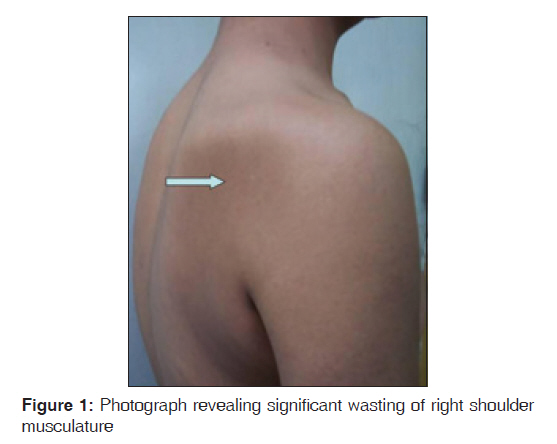
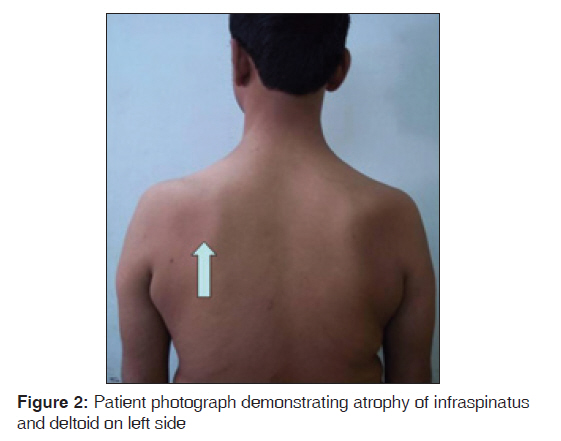
Abstract Keywords: Brachial plexopathy, dengue fever, neuralgic amyotrophy, parsonage-turner syndrome Introduction Dengue is an acute viral infection caused by one of the four distinct serotype of dengue viruses (type 1-4), from the genus flavivirus and transmitted by Aedes mosquitoes. The incidence of dengue infection has increased rapidly in recent decades. The disease is prevalent in more than 100 countries in Africa, the Americas, the Eastern Mediterranean, South-East Asia and the Western Pacific, with an approximately 2.5 billion people (two-fifths of the world′s population) at risk of infection. The World Health Organization (WHO) estimates that 50 to 100 million infections occur annually. [1] The majority of dengue infection is subclinical in nature. In a prospective Cohort study of students conducted in Bangkok, about 85% of the dengue virus infections were subclinical. [2] Dengue fever has been reported to have wide spectrum of neurological complications, such as encephalopathy, myelitis, myositis, acute disseminated encephalomyelitis, Guillain-Barre syndrome, hypokalemic paralysis, encephalitis and stroke. [3],[4] The exact incidence of neurological involvement is still not well known. The calculated incidence of the encephalopathy and encephalitis, the most common reported neurological complications in dengue, was ranging from 0.5% to 6.2% in various studies. [3] In this report, we described three patients of neuralgic amyotrophy associated with dengue fever from tertiary center of Lucknow, India. The neuralgic amyotrophy, also known as brachial neuritis, occurs due to involvement of brachial plexus and characterized by the acute onset of severe unilateral shoulder pain, followed by flaccid paralysis of shoulder and parascapular muscles a few days later. The brachial neuritis associated with dengue infection has not been described so far in the literature. Case Report Case 1 A 27-year-old young male developed acute onset high-grade fever along with generalized bodyache, retroorbital pain, rashes and multiple joints pain. He consulted local physician and became asymptomatic completely after 4 days. One week later, he developed severe excruciating pain at the back of neck and right shoulder. It was followed by weakness and atrophy of right arm musculature [Figure - 1]. There was no history of recent trauma, vaccination and surgery. On examination, he was having MRC grade 3 power in right deltoid, biceps and triceps, with some hypoanesthesia in the distribution of right lateral antebrachial nerve. The right biceps and triceps reflexes were hypoactive. The neurophysiological evaluation was performed after 4 weeks. The right radial SNAP is on the lower side of normal, but markedly abnormal (less than 50% in amplitude) in comparison to left side. The right lateral antebrachial cutaneous SNAP was absent, with normal SNAP on left side. The proximal nerves stimulation from erb′s point showed reduced CMAP amplitudes in right axillary nerve (deltoid), right musculocutaneous nerve (biceps), right supascapular nerve (supraspinatus) and right radial (triceps). The needle EMG study showed denervation potentials in the form of fibrillations in the right C5, C6 and C7 myotomes involving multiple nerve distribution including axillary (deltoid), musculocutaneous (biceps), radial (triceps) and suprascapular nerve (supraspinatus). Magnetic resonance imaging of brachial plexus and cervical spine did not reveal any abnormality. The serum IgM antibody against herpes simplex virus, Japanese encephalitis virus, coxsackie virus, enzyme-linked immunosorbent assay (ELISA) for human immunodeficiency virus and Epstein-Barr virus were negative. The serum IgM antibody to dengue virus was positive. The serum IgM antibody were analysed by ELISA method using IgM ELISA Kit by Panbio Invernis Medical Innovations, Australia Gnbh. We performed serum IgM ELISA testing twice at 1 week apart to reconfirm the dengue infection in all these patients. Vasculitic markers including antinuclear antibody, rheumatoid factor were negative. Other metabolic parameters including blood sugar, serum creatinine, blood urea, liver function test, T3, T4, TSH (thyroid profile) were in normal range. Diagnosis of neuralgic amyotrophy associated with dengue fever was considered and oral prednisolone in dosage of 1 mg/kg body weight along with amitriptyline was prescribed. He responded to treatment well and pain was relieved completely within 7 days and there was no further progression of weakness after 3-4 days of initiation of treatment. The objective improvement in power was noted at 3 weeks as his MRC power grade increased to grade 4. After 3 months of follow-up, he was completely asymptomatic. Case 2 A 35-year-old male presented with severe pain in left shoulder since 12 days. Later on, he developed weakness and atrophy of musculature of the left arm region [Figure - 2]. He complained of difficulty in elevating the left upper limb. He had also suffered from moderate to high-grade fever associated with severe myalgia and petechial rashes 5 days prior to onset of pain. The fever lasted for 3-4 days and subsided with the treatment. The power was MRC grade 4 at left shoulder abduction, elbow flexion and extension, MRC grade 3 power in finger flexors. The deep tendon reflexes, biceps and triceps were hypoactive. The sensations were diminished in left antebrachial nerve region and over left shoulder. The rest of the neurological examination was unremarkable. The routine laboratory parameters including complete hemogram, liver function test, renal function test, thyroid profile (T3, T4, TSH) were within normal range except thrombocytopenia (platelets count 82 thousand/cumm). The study for vasculitic markers, screening for various viruses were negative except dengue virus. The serum IgM antibody to dengue infection was positive. Magnetic resonance imaging of cervical spine and brachial plexus studies revealed normal findings. The electrophysiology was done at 4 week which revealed patchy axonal damage suggestive of brachial neuritis. Nerve conduction studies showed decreased CMAP amplitudes in axillary, musculocutaneous and suprascapular nerves. Electromyographic studies demonstrated spontaneous activity (positive sharp waves, fibrillations) and reduced interference in deltoid, supraspinatus and first dorsal interosseus muscles. He was treated with steroids (prednisolone 1 mg/kg body weight) for 4 weeks and then tapered over next 2 weeks. The pain decreased in intensity over 3-4 days of initiation but did not subside completely until about 3 weeks. The strength started improving after 3 weeks and the clinical recovery was satisfactory at follow-up after 3 months. Case 3 A 36-year-old male presented with complaints of severe pain at back of the neck radiating to left shoulder region. Over subsequent days, he developed weakness in the left upper limb, prominently in arm abduction. One week prior, he had moderate to high-grade fever with arthralgia, which subsided with certain medications after 3 days. The family history was not significant. Examination findings were restricted abduction on left side with decreased sensation on left shoulder region. Mild to moderate atrophy was evident in deltoid, supraspinatus and infraspinatus. The electrophysiological evaluation was consistent with brachial neuritis. The serum IgM antibody against dengue was positive. The steroids were prescribed in dosage of 1 mg/kg for 4 weeks. Patient showed remarkable recovery. Discussion Neuralgic amyotrophy was first described by a French physician, Joffroy in year 1879. [5] Parsonage and Turner in 1948, were responsible for recognition of this syndrome as a distinct clinical entity and labeled it as shoulder girdle syndrome. Their original description denotes clinical presentation of acute onset shoulder pain, followed by flaccid paralysis of the shoulder girdle arm musculature as pain resolves. [6] Parsonage and Turner syndrome has multiple nomenclature, out of them acute brachial neuritis, neuralgic amyotrophy, brachial neuropathy or neuritis of the shoulder girdle are well-recognized terms. It can be confused with various neurogenic and non-neurogenic conditions, including rotator cuff abnormalities, acute calcific tendinitis, adhesive capsulitis, cervical spondylosis, entrapment neuropathies and tumors. [7] It is an uncommon clinical condition, with reported incidence of 1.64 cases per 100,000 population. The exact etiology of Parsonage-Turner syndrome is controversial. Various factors have been postulated including viral infections, trauma, strenuous exercise, recent surgery, immunization and autoimmune disorders. [8] The history of trauma, preceding heavy exercise, recent surgery, immunization and clinical or investigative workup for autoimmune disorders were absent in all three of our patients. They presented with brachial neuritis and IgM ELISA was positive for dengue infection in all three patients. The neurological complications of dengue infection can be classified into three categories. Neurotropic effect of virus caused encephalitis, meningitis, myositis, myelitis: Systemic complications manifesting as encephalopathy, stroke, hypokalemic paralysis and postinfectious immune-mediated complications includes acute disseminated encephalomyelitis, myelitis, neuromyelitis optica, optic neuritis and Guillain-Barre syndrome. [3],[9] Neuralgic amyotrophy had been reported with various micro-organisms including viruses, bacterial and fungal agents. [10] Various viruses known to cause neuralgic amyotrophy are Epstein-Barre virus, varicella zoster, coxsackie virus, herpes simplex, cytomegalovirus, hepatitis B, hepatitis E, West nile virus, parvo B 19 virus, vaccinia virus and HIV virus. The bacterial infections associated with neuralgic amyotrophy includes Chlamydophila pneumonia, Leptospira species, Mycoplasma pneumoniae, Escherichia coli, Borrelia burgdorferi, Bartonella henselae, Neisseria gonorrhoe, Coxiella burnetti, Salmonella panama, Yersinia enterocolica, Staphylococcus aureus, Streptococcus group A and Brucella species. Brachial neuritis had also been reported with Aspergillus fungi. Neuralgic amyotrophy had not been described with dengue viral infection. The available evidence suggests immune-mediated mechanisms in the pathogenesis of brachial neuritis. The antiganglioside antibodies had been demonstrated in the patients of brachial neuritis. [11] The presence of inflammatory changes in the brachial plexus biopsy of these patients also suggests immune-related injury. [12] The brachial neuritis used to occur after a few days to weeks of an infectious illness, which again can be corroborated as postinfectious immune-mediated event. [11] Similarly, the dengue virus may lead to immune-mediated injury and brachial amyotrophy. The molecular mimicry may be responsible for immunogenic injury in brachial neuritis as explained in Guillaine-Barrι syndrome. The good response to steroids in our patients also suggest role of inflammation and immune-mediated injury in the pathogenesis of brachial neuritis. The association of the dengue infection with brachial neuritis may further help in delineating the pathophysiology of brachial neuritis which might affect the treatment strategy. Dengue fever leads to various neurological complications, causing significant morbidity and mortality. Neuralgic amyotrophy had never been reported in association with dengue fever. This report will also add dengue infection to the list of various infections associated with brachial neuritis. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11090f2.jpg] [jp11090f1.jpg] |
| |||||||||


{kind=link}
{kind=link}