
|
Journal of Postgraduate Medicine
Medknow Publications and Staff Society of Seth GS Medical College and KEM Hospital, Mumbai, India
ISSN: 0022-3859 EISSN: 0972-2823
Vol. 57, Num. 4, 2011, pp. 338-339
|
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 338-339
Case Snippet
Atypical presentation of joint infection by an unusual organism
SP Roy, AP Singla, SK Jain, ON Nagi
Department of Orthopaedic, Joint Replacement and Reconstruction Center, Sir Ganga Ram Hospital, New Delhi, India
Correspondence Address: S P Roy, Department of Orthopaedic, Joint Replacement and Reconstruction Center, Sir Ganga Ram Hospital, New Delhi, India, roy_sp27@yahoo.co.in
Code Number: jp11093
PMID: 22120866
DOI: 10.4103/0022-3859.90089
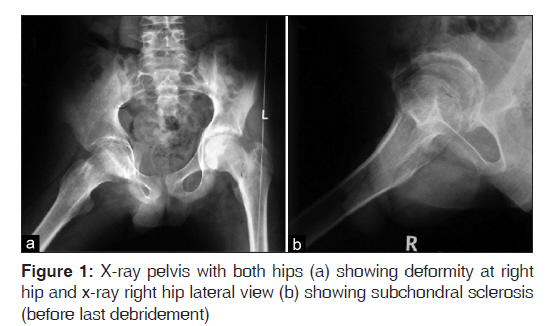
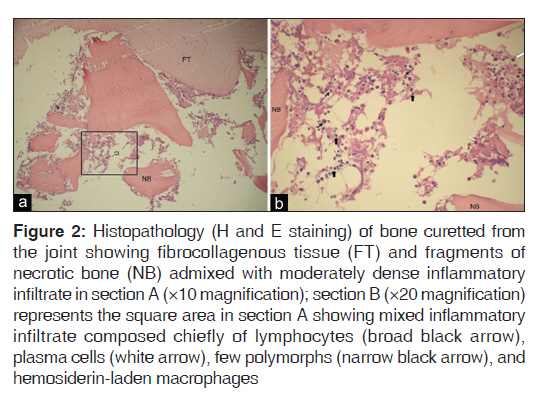
A 14-year-old boy came to our centre with painful and crippling flexion and abduction deformity of right hip without local signs of inflammation and with a two-year history of antitubercular (ATT) treatment. At presentation, there was no pyrexia, other joint involvement, and personal or family history for tuberculosis or inflammatory arthritis. Radiograph of right hip revealed deformity, diminution of joint space with subchondral sclerosis, and cyst formation, which were consistent with arthritic changes [Figure - 1]. He had a history of diagnostic arthrotomy done in the beginning and arthrofibrolysis done one year after the arthrotomy. We performed debridement and sent the pathological tissue for histopathological and microbiological (pyogenic, tubercular, fungal) examination. Tissue culture revealed growth of Staphylococcus hominis which was identified using microbial identification kit (VITEK 2 system, bioMe΄rieux, Marcy l′Etoile, France). [1] The organism was sensitive to Clindamycin and Oxacillin; histopathology revealed signs of chronic inflammation, but no granuloma was detected [Figure - 2]. Systemic intravenous antibiotic therapy with Clindamycin (600 mg twice daily) and Cloxacillin (500 mg four times daily) for 6 weeks rendered the boy pain free and the inflammatory markers came to normal. Uncemented total hip arthroplasty (THA) was done three months after the debridement to correct the crippling deformity and provide a functional life. Twelve months after the THA, he was walking pain free with an acceptable functional outcome.
S. hominis is a Gram-positive coagulase-negative bacterium, a commensal of human body. The mode of transmission of S. hominis is through intravenous cannula, breach in the skin, direct inoculation into the surgical wound, or through implantation of foreign body. This microorganism was generally considered a contaminant in the microbiologic cultures until it was reported to cause sepsis in the neonatal intensive care units and prosthetics. [2],[3],[4] Recently, it has been implicated in osteomyelitis and pyomyositis in a immunocompetent patient, [5] but never has been reported to cause non-prosthetic joint infection as per our knowledge. The organism could have been inoculated from the skin surface during the previous interventions and lead to secondary joint infection. Rifampicin, one of the most important first-line chemotherapeutic drugs in ATT, is also a broad-spectrum antibiotic. It also acts against Gram-positive organisms, but monotherapy is not recommended due to the development of resistance. [6] This prolonged rifampicin therapy probably suppressed the S. hominis growth to a very low level of multiplication but failed to eradicate it, leading to an indolent chronic clinical course. Cellular infiltration as evidenced in the histopathology [Figure - 2] also supports this chronic nature of infection.
In our case, we considered it to be the causative pathogen because (i) the patient′s disease did not improve with ATT and previous surgeries, (ii) Acid-fast Bacilli or granuloma were not identified in any of the histological evidence, (iii) S. hominis grew in the primary culture from different samples (bone and granulation tissue), which were collected with aseptic protocol, and (iv) histopathology of the necrotic bone was suggestive of chronic osteomyelitis. Furthermore, the inflammatory markers reverted to normal and the patient improved symptomatically with antibiotics which were selected according to the standardized sensitivity testing antibiogram. This case emphasizes that S. hominis, which is a part of normal body flora and otherwise considered as culture contaminant if identified in culture, should be considered as an pathological agent of joint infection, especially when there is doubtful and atypical presentation.
Acknowledgment
We thank Dr. Neeraj Goel, Microbiologist of our institute, for his critic editorial help in presenting basic science information regarding Staphylococcus hominis and Dr. Fauzia Siraj, Pathologist of our institute, for providing the histopathology evidence.
References
| 1. | Layer F, Ghebremedhin B, Moder KA, König W, König B. Comparative study using various methods for identification of staphylococcus species in clinical specimens. J Clin Microbiol 2006;44:2824-30. Back to cited text no. 1 |
| 2. | Chaves F, Garcia-Alvarez M, Sanz F, Alba C, Otero JR. Nosocomial Spread of a staphylococcus hominis subsp. novobiosepticus strain causing sepsis in a Neonatal Intensive Care Unit. J Clin Microbiol 2005;43:4877-9. Back to cited text no. 2 |
| 3. | Palazzo IC, d'Azevedo PA, Secchi C, Pignatari AC, Darini AL. Staphylococcus hominis subsp. novobiosepticus strains causing nosocomial bloodstream infection in Brazil. J Antimicrob Chemother 2008;62:1222-6. Back to cited text no. 3 |
| 4. | Teterycz D, Ferry T, Lew D, Stern R, Assal M, Hoffmeyer P, et al. Outcome of orthopedic implant infections due to different staphylococci. Int J Infect Dis 2010;14:e913-8. Back to cited text no. 4 |
| 5. | Rodríguez NG, Muñoz OD. Pyomyositis, sacroiliitis and spondylodiscitis caused by Staphylococcus hominis in a immunocompetent woman. An Med Interna 2006;23:582-4. Back to cited text no. 5 |
| 6. | Thornsberry C, Hill BC, Swenson JM, McDougal LK. Rifampin: Spectrum of antibacterial activity. Rev Infect Dis 1983;5(Suppl 3):S412-7. Back to cited text no. 6 |
Copyright 2011 - Journal of Postgraduate Medicine
The following images related to this document are available:
Photo images
[jp11093f2.jpg]
[jp11093f1.jpg]
|

{kind=link}
{kind=link}