 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
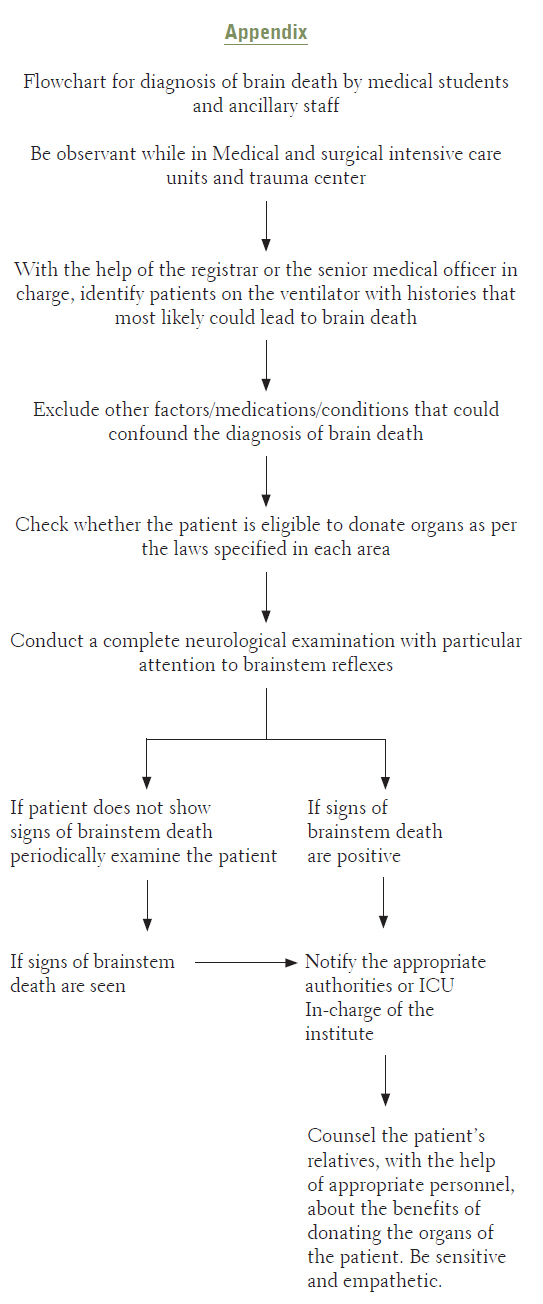
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 347-349 Students Corner Improving the rates of cadaver organ donation in a tertiary care transplant centre: A role for medical students and ancillary staff SS Patwardhan, GV Kulkarni Seth GS Medical College and KEM Hospital, Parel, Maharashtra, India Date of Submission: 15-May-2011 Code Number: jp11097 PMID: 22120870 The concept of death is a void in man′s understanding of the world. Cessation of cardiopulmonary function has been traditionally viewed as a benchmark to declare death. However, it can be artificially maintained for a required duration. Conversely, the functional loss that sets in due to damage caused to the vital centers of the brain is irreversible and hence brainstem death is equivalent to the death of the person. It is characterized by coma, absence of brainstem reflexes and apnea. [1] First proposed by two French scientists, Mollaret and Goulon, it has been a topic of debate [2],[3],[4],[5] and recognition of this state is an essential task for any physician due to its importance in deciding potential donors for cadaver organ transplantation. Cadaver organ donation requires that a person be declared dead in order to procure the organs, as per the dead-donor rule. [6] Efficient and timely diagnosis, and referral of brainstem death, can help support the cause of organ transplantation. [7] Each cadaver donor can save six lives and restore eyesight to two blind individuals. This is particularly relevant in a highly populated country like India, where the demand for organs is always going to exceed the supply. [8] Hence there is a need to increase awareness about brainstem death and its relevance to cadaver organ donation amongst medical students and hospital staff, a fact highlighted by a recent study conducted in Bangalore which showed that the concept of brainstem death was understood by only a small number of medical postgraduate students. [9] An even more worrisome fact is the relative lack of this knowledge amongst the general population in spite of having the willingness and the openness to accept organ donation. [10] The main challenge that stands in the way of a successful transplant program is the next of kin, who, for a large measure, disagree to donate the organs of their deceased relative. Morals, religious beliefs, taboos, a lack of awareness about brain death, an incorrect method of breaking the news of death and putting forth the request for organ donation and a relative lack of trained transplant coordinators come in the way of convincing families about the benefits of organ donation. [11],[12] They need to be educated sympathetically and calmly by physicians and medical social workers alike, to impress upon them the far-reaching effects of their selfless act. Brainstem death is diagnosed, primarily, by clinical methods as it is very difficult to establish the evidence of its accuracy by experimental means. [1],[13] The diagnosis is usually made by a team of doctors, which includes the attending physician, a neurologist or a neurosurgeon, an independent registered medical practitioner, being a specialist, nominated from a panel of names approved by the Appropriate Authority and a doctor on the administrative board of the hospital. The recent amendments proposed in the Transplantation of Human Organs Act have allowed selection of a surgeon/physician and an anesthetist/intensivist, in the event of the non-availability of a neurosurgeon/neurologist, from a panel already approved by the Appropriate Authority as specified by the Act. [14],[15] The examination of the patient must be repeated after 6 h for confirming the diagnosis of brainstem death. [1] As medical students and interns, our role can involve the identification of brain-dead patients to supplement the ongoing transplant program at our institute. The program for renal transplantation has been running for almost a decade now while that for liver transplantation has been initiated last year. We periodically visited the Medical and Surgical Intensive Care Units, including the Casualty and Trauma centre to screen patients who most likely fit into the category of brainstem-dead individuals. We did this by reviewing the histories of all the patients admitted. The following criteria were applied to narrow down the probable individuals:
Following this exhaustive workup, patients who fitted all the criteria were subjected to a complete neurological examination. The following signs were highly suggestive of brain death:
After confirmation by senior medical personnel, the ventilator was disconnected and the apnea test was performed. Once it was confirmed that the person was brain-dead, the necessary authorities were informed who then started the process of counseling the patient′s relatives about the status of the patient and benefits of donating the organs. Thus, it has been an important learning experience and has shown the necessity of involving more students, undergraduates and postgraduates alike, in this program to increase the awareness of brainstem death in the medical fraternity. This will ensure better counseling of the patient′s relatives and a more organized approach towards organ procurement and transplantation, ultimately increasing the yield of such undertakings and saving more lives. [Annex 1] Public awareness, though an important aspect, may not necessarily be the main hurdle in this program. Failure of identification and institutional reporting of brainstem death in the Intensive Care units may also be equally responsible for the limited success garnered by such programs in India. There have been recent positive amendments to the Transplantation of Human Organs Act of India. [15] They have addressed this problem, though there has been a delay in its implementation. Mandatory reporting of such cases to appropriate authorities has to be strictly enforced by the district health services. Acknowledgment We sincerely thank Dr. Sujata Patwardhan and Dr. Avinash Supe for their timely guidance and support in the writing of this article. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11097a1.jpg] |
| |||||||||


{kind=link}