 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
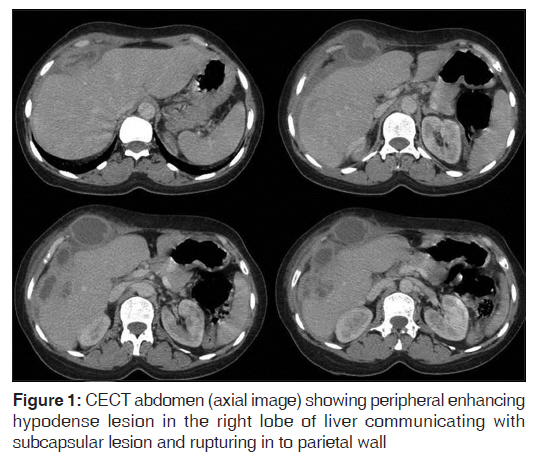
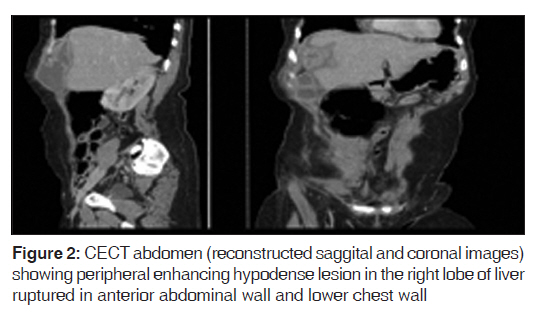
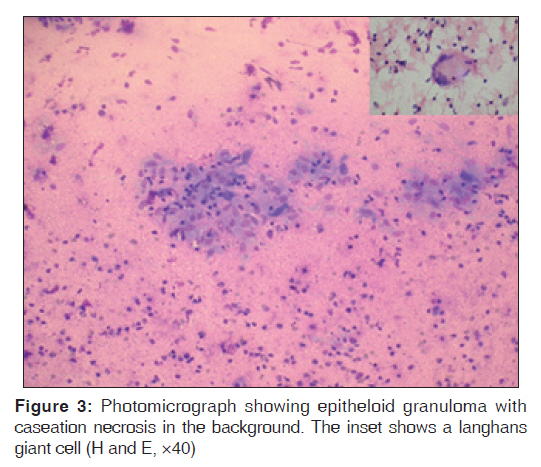
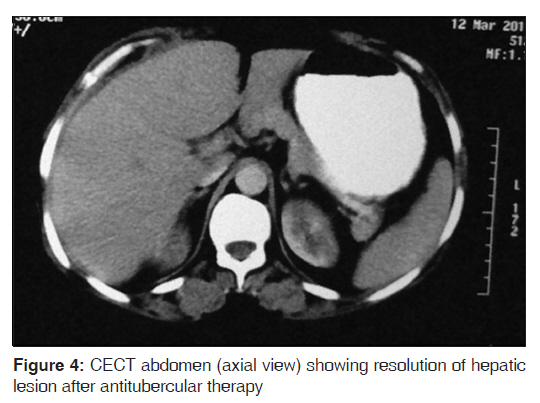
Journal of Postgraduate Medicine, Vol. 57, No. 4, October-December, 2011, pp. 350-352 Letter Primary tubercular liver abscess rupture leading to parietal wall abscess: A rare disease with a rare complication G Gupta, S Nijhawan, P Katiyar, A Mathur Department of Gastroenterology, SMS Medical College and Hospital, Jaipur, Rajasthan, India Code Number: jp11099 PMID: 22120872 Sir, Tuberculosis presenting solitary, as liver abscess is rare and the prevalence of tubercular liver abscess is 0.34% in patients with hepatic tuberculosis. [1] A 35-year-old woman presented with continuous dull pain in the right hypochondrium, anorexia and weight loss for 5 months. Physical examination revealed a tender, cystic, fluctuant lump 5×5 cm on the right anterior lower chest wall extending to upper abdominal wall. Investigations showed hemoglobin 7.8 gm/dl; total leukocyte count 7290/mm 3 ; erythrocyte sedimentation rate 52 mm/h; total bilirubin 0.7 mg%; serum alkaline phosphatase 107 IU; AST 23 IU; ALT 107 IU; serum protein 7.7 g/dl and serum albumin 3.9 g/dl. HIV serology was negative. Chest X-ray was normal. Ultrasonography (USG) of the abdomen revealed two cystic space occupying ill-defined, heterogeneous hypo-echoic lesions both measuring 3×3 cm and one solid lesion measuring 2.5×3 cm in the right lobe of liver. Contrast-enhanced computed tomogram of abdomen revealed a hypodense peripherally enhancing lesion measuring 2.8×3.2 cm in the right lobe of the liver communicating with the subcapsular lesion and parietal wall abscess [Figure - 1] and [Figure - 2]. USG guided FNAC revealed epithelioid granulomas, caseation necrosis and occasional langhans giant cells [Figure - 3]. No acid-fast bacilli were detected. PCR of the aspirate was positive for M. tuberculosis. Patient was treated with four drug anti-tubercular therapy (ATT) and showed symptomatic response and on follow up after 5 months hepatic lesions resolved [Figure - 4]. Hepatobiliary tuberculosis is classified as Miliary, granulomatous, and localized. [2] Primary localized involvement as a tuberculous abscess alone is rare. Clinical manifestations of tubercular liver abscess are nonspecific. Common complaints include vague/localized right upper quadrant pain, fever, and anorexia. Ruptured tubercular liver abscess presenting as a parietal wall swelling is an extremely rare presentation. There are two similar case reports, one had liver abscess ruptured in chest wall [3] and another in abdominal wall. [4] Accurate diagnosis is often delayed and high index of suspicion is required for diagnosis and is commonly misdiagnosed as malignancy, pyogenic, and amoebic liver abscess. Radiologic examination is a useful tool to diagnose hepatic tuberculosis. Plain radiographs may show hepatic calcifications and concomitant pulmonary tuberculosis in 10-86% of cases. [5] USG and computed tomography (CT) will detect masses, their extent and local complications. Etiological diagnosis requires tissue sampling by FNAC or biopsy and diagnosed by characteristic granuloma ± caseation necrosis and presence of AFB, culture or PCR. Except for PCR which has sensitivity up to 100%, [6],[7] all other methods have low sensitivity. Some clinicians accept a good response to ATT as an evidence of tuberculosis, but this approach may waste the crucial time especially in malignancy; hence, this should be deferred in the present era of modern diagnostics. These cases should be treated with ATT under category I of DOTS. Therefore, one should keep possibility of tubercular etiology in case of liver abscess with indolent course and TB-PCR is an important tool for its diagnosis. References
Copyright 2011 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp11099f3.jpg] [jp11099f1.jpg] [jp11099f4.jpg] [jp11099f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}