 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
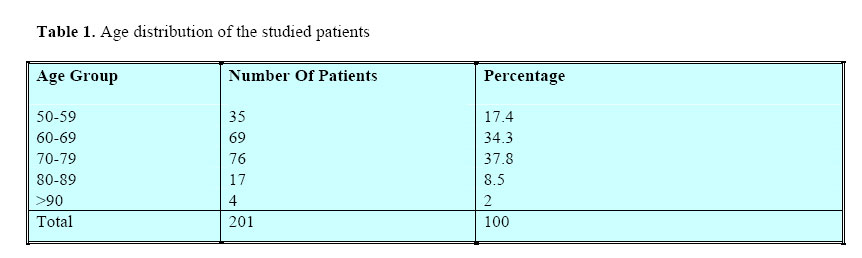
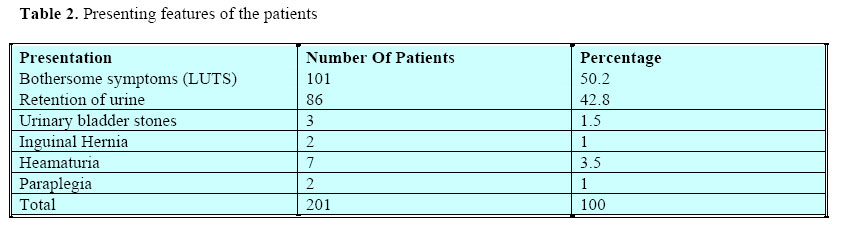
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 17-20 Prostate Cancer Case Finding In Patients With Lower Urinary Tract Symptoms In A Private Hospital In Dar-Es-Salaam.Yongolo CMS Senior Lecturer, Muhimbili University College of Health Sciences. P.O. Box 7845 Dar-es-Salaam, Tanzania. E-mail: syongolo@muchs.ac.tz Code Number: js04030 Objective: To determine the proportion of patients with Carcinoma of the Prostate in patients presenting with Lower Urinary Tract Symptoms. Introduction Patients with prostate cancer may present with voiding symptoms suggestive of bladder outlet obstruction or those related to metastatic disease. The prevalence of prostate cancer continues to increase with age, and after age 50, both incidence and mortality rate from prostate cancer increase at a near exponential rate1 . At present, prostate cancer is the most common cancer diagnosed in men in the United States and the second most common cause of cancer death. Blacks living in the USA have a higher incidence rate of clinical prostate cancer than white men of similar education and socio-economic classes at all ages2 . Furthermore, black men are routinely diagnosed with late stage disease, and survival rates, even when correlated for stage, are uniformly lower for black men. The histological diagnosis of prostate cancer is made, in the majority of cases, by prostatic needle biopsy. Thus, suspicion of prostate cancer is most often raised by abnormalities found on digital rectal examination (DRE), or serum prostate-specific antigen (PSA) elevations. Routine use of PSA increases the detection of prostate cancer over that of DRE, improves the predictive value of the DRE for cancer, and increases the detection of prostate cancers that are organ confined yet significant in terms of size and grade. PSA is the single test with the highest positive predictive value for cancer of the prostate 3 . It has been reported in different studies in screened populations that the approximate chance of cancer on biopsy is 1 in 50 for men with PSA levels below 4.0 ng/ml3 , 1 in 4 for PSA levels of 4.0 to 10 ng/ml, and 1 in 2 to 3 for PSA levels greater than 10 ng/ml4,5 . PSA increases the predictive value of the DRE for cancer of the prostate6,7 . A decrease in the mortality rate of prostate cancer following introduction of screening has been reported8,9 . In developing countries however, health provision is sub-optimal due to poor economy, and screening procedures cannot be done due to cost constraints. It follows therefore that the use of PSA as a screening tool for CP in the community is not feasible10,11 . Introduction of new diagnostic tests in developing countries are delayed and when available are expensive and inaccessible to the general public. When introduced few private laboratories own them. This prohibits the tests to be used for screening purposes. PSA was introduced in Tanzania five years ago. This paper presents the experience on case finding of prostate cancer in patients presenting with lower urinary tract symptoms (LUTS) in a private clinic in Dar- Es Salaam. Patients and Methods This was a prospective case finding study of four years in a private hospital in the centre of Dar-Es Salaam during the period of January 2000 to December 2003. Patients eligible for this study were all those who were 50 years or more who presented with lower urinary tract symptoms requiring investigations and treatment. The hospital had one working urologist who saw all patients presenting with urology problems. Those patients had a history and physical examination done except digital rectal examination (DRE), which was carried out after blood for PSA had been drawn. Other investigations done included serum creatinine, abdominal ultrasound of the kidney, ureter, bladder and prostate. The hospital has no rectal probe for Trans-rectal ultrasound (TRUS). The other investigations were tailored to the other presenting symptoms and signs of the patient. Those who had urethral stricture with a normal PSA and DRE were however excluded, as the tissue biopsy was not obtained. The age of the patient and the presenting symptoms were recorded. The urologist documented all the findings of the DRE. Those patients who had abnormal DRE findings in the prostate had a tru-cut biopsy taken from the prostate by finger guidance. Patients who had an elevated PSA without suspicious nodule had sextant core biopsies done. Cut off point for PSA in the lab was 4ng/ml. Patients who had significant urinary symptoms were treated by TURP or open prostatectomy. Tissues from prostatectomy were examined to determine whether prostate cancer was evident. The Gleason score was also done and recorded at histology. Patients with prostate cancer were treated by Orchidectomy, Lutenizing Hormone Releasing Hormone (LHRH) agonist (Zoladex), Radiotherapy or watchful waiting according to the stage and grade of the disease. Results A total of 219 consecutive patients with lower urinary tract symptoms were seen at the hospital. However 201 are presented in this study. Eighteen patients who had LUTS secondary to urethral stricture were excluded as none of them had prostate biopsy done. The age range of the patients was from 50 to 98 with a mean of 68.4 years. The majority (72.1%) of the patients belonged to the age groups 60–69 and 70–79 (Table 1). The reason for consultation was significant bothersome symptoms of lower urinary tract in 101 (50.2%) of the patients and retention of urine in 86 (42.8%). The other presenting features were stones, hernia and UTI. Two patients had paraplegia The range of PSA was 0.68 to >100 ng/ml. The upper range in this laboratory was indicated as more than 100 a draw back to the average results of PSA to cancer group of patients. Twenty-eight (13.9%) of all patients had prostate cancer and had an average age of 68.7 years. Apart from lower urinary tract symptoms some patients presented with metastatic symptoms of paraplegia, low back pain, anaemia, oedema of the legs, weight loss and general weakness. The DRE was abnormal in 23 patients together with raised PSA. Two patients without abnormality of DRE were diagnosed CP on finding a raised PSA. The other three patients were diagnosed as incidental findings from TURP with a normal PSA (Table 3). Twenty-four patients had Orchidectomy as the treatment (one patient started with Zoladex and had to have Orchidectomy done due to cost constraint); one patient was treated with LHRH agonist Zoladex while one patient received radiotherapy outside the country. Two of the three patients who had incidental carcinoma with a favourable Gleason score were managed on watchful waiting with regular PSA checks. Discussion The advantage of early diagnosis of prostate cancer and its treatment by radical surgery and its influence to survival is well documented12 . Being asymptomatic in the early stage, prostate cancer discovery is facilitated by the use of screening and PSA, which has increased the detection and lead to the recommendation of mass screening for it13,14. However the debate on the logic of treatment of localized disease, which is usually found during screening with the slow growth of the tumour has also been posed15 . Moreover community screening due to metastasis of CP to the spine (Table 2). Taking all patients together the average PSA measured by Min-Vadas France BioMurex Lab reagents was 13.12ng/ml. However the average PSA in the 173 patients with BPH was 6.71ng/ml. Patients with prostatic cancer had an average PSA of 51.99ng ml. of prostate cancer by use of PSA in expensive and though desirable is prohibitive in poor countries where case finding studies will remain the main source of data. The mean age in this series of patients was slightly higher than those reported in one publication in this continent10 . All of the patients had significant lower urinary tract symptoms. The majority of the patients (86.1%) were found to have BPH while 13.9% had prostate cancer. This ratio is slightly higher than that reported in Egypt10 but is comparable with findings in another study which on top of DRE and PSA used Transrectal Ultrasound (TRUS) which could probably explain the higher pick up ratio16 . The high ratio in our series of patients, may be an indication of a possibly high incidence of Carcinoma of the Prostate in our population in black Africa. Indeed prostate cancer rarely causes symptoms early in the course of disease because the majority (70- 85%) of adenocarcinoma arises in the periphery of the gland (peripheral zone), distant from the urethra. In the other group of patients (15-30%), the cancer develops from the other zones. The presence of symptoms as a result of prostate cancer suggests coexistence with BPH, a locally advanced or metastatic disease, as was the case in the majority of our patients who had advanced disease at diagnosis. Only five patients out of the twenty-eight patients were diagnosed with early malignancy and would qualify for Radical Prostatectomy. All suspicious lesions at DRE underwent a biopsy and confirmed the disease a high pick up rate. In one series it was reported that approximately 50% of suspicious lesions represented cancer on prostate biopsy 17 . Because of the significant risk of prostate cancer, prostate biopsy is recommended for all men who have DRE abnormalities, regardless of the PSA level, since there is still a chance, however small of CP even when PSA level is less than 4 ng/ml 3. It is of paramount important to note here that till now clinical presentation and abnormal DRE remains the main way of diagnosis of CP in most of the hospitals in this country. However, we also emphasize that DRE misses from 23% to 45% of the cancers that are subsequently found with prostatic biopsies done for serum PSA elevation or Trans-rectal ultrasound abnormalities18,19. In our series five patients would have been missed since their DRE was normal. The studied population here is not a representative sample as this was a selected group who can afford treatment in a private hospital. Secondly the number of patients is small to draw a conclusion but the proportion of CP is high. Also the stage at which the disease at diagnosis was advanced similar to What others report that prostate cancer detected by DRE in screened and unscreened populations of men are pathologically advanced in more than 50% of men15. Where possible in developing countries a combination of DRE and PSA in patients with LUTS should be used to pick up more cases with CP. There is however a need to establish the true prevalence of CP in a black African country by a well planned randomized study using PSA, DRE and TRUS. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04030t3.jpg] [js04030t1.jpg] [js04030t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}