 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 21-24 Pelviureteric Junction Obstruction: A Surgical ExperienceG. A. Maranya, MMED (SURG), CERT UROL (EA), P. R. Oduor, MMED (SURG) Consultant Surgeons, Coast Province General Hospital. Code Number: js04031 Objective: To describe the experience in the management of patients with intrinsic
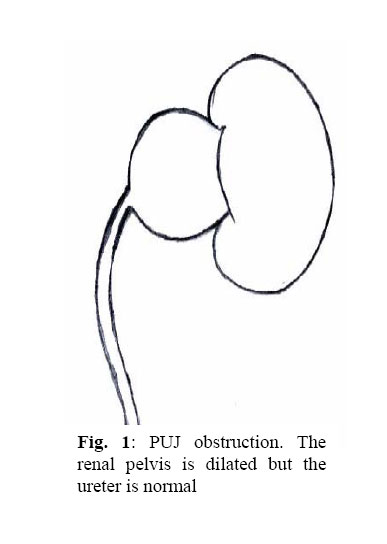
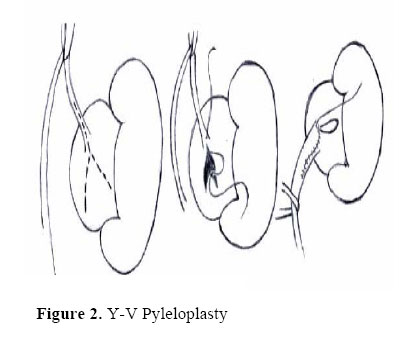
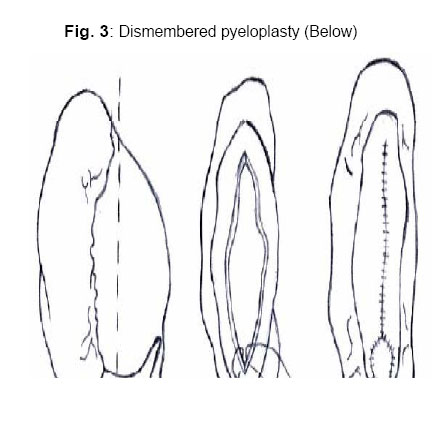
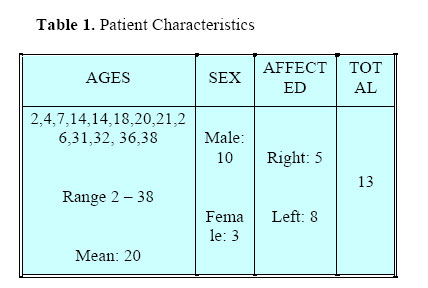
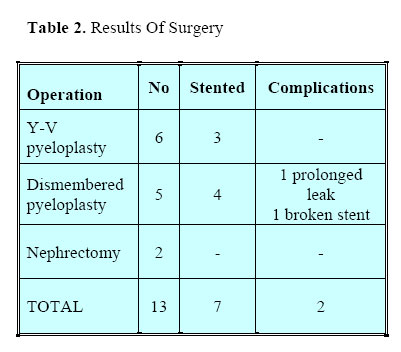
pelviureteric junction obstruction in the town of Mombasa, Kenya. Introduction Pelviureteric junction (PUJ) obstruction is a common site of urinary obstruction in children and is a frequent site of obstruction in adults of all ages1. Obstruction may be caused by a functional abnormality of the proximal ureter (intrinsic obstruction), which is the subject of this presentation. It may also be caused by intraluminal lesions, external compression, usually by an aberrant renal vessel (extrinsic obstruction) or may be secondary to vesicoureteric reflux (secondary obstruction). Intrinsic obstruction accounts for more than 90% of cases, is more common in males than females and affects the left kidney more than the right 2. Bilateral involvement occurs in about 15% of cases. Patients with PUJ obstruction are more likely to have associated congenital anomalies; some of those in the urinary tract being anomalies of position and fusion. Associated primary vesicoureteric reflux; ipsilaterally or contra laterally has been described 3. The pathology of intrinsic PUJ obstruction is characterized by a persistent, narrow, aperistaltic segment of ureter 2-10mm long immediately below the PUJ (Fig 1). The nature of the functional obstruction within this segment is undetermined. Various histological changes have been described within the narrow segment including an increase in the collagenmuscle ratio, thickening of the lamina propria, circular muscle arrangement rather than the normal predominant longitudinal; but it is uncertain if these changes are primary or secondary. Presentation in infancy is most commonly with urinary infection. Sometimes the finding is incidental and occasionally presentation is with a renal mass, haematuria, failure to thrive or persistent vomiting. Most of the adults present with episodic loin pain. In some younger patients the pain may be located in periumbilical region. In many children, however the lesion is found incidentally. Investigations aim at determining the anatomy of the lesion. These are ultrasonography and intravenous urography (IVU). Where the anatomy is in doubt retrograde ureterography may be done. Cystography is restricted to patients with urinary infection or who show distal ureteric dilatation on ultrasound or IVU. This checks for vesico-ureteric reflux. Management may be expectant in children with good function. Follow up is done with regular ultrasound examinations. Surgery by open pyeloplasty is the usual means of correcting PUJ obstruction. The main techniques employed are Y-V plasty (Foley)4 and dismembered pyeloplasty (Anderson – Hynes)5. An outline of the procedures is shown (Fig 2, Fig 3). The technical results are good in more than 90% of cases 2,6,7. Currently, laparoscopic pyeloplasty is the method of choice in many centres 8,9. Retrograde balloon dilatation and endopyelotomy11, involving a cold-knife incision of the ureteric segment using an endoscope passed via a nephrostomy tract, represent alternative minimally invasive procedures. They have shown early satisfactory results, but their eventual role is yet to be defined. Robotic pyeloplasty has also been done12. Patients and Methods. An evaluation of 13 patients with PUJ obstruction, who were operated upon by the authors between 1995 and 2003 was made. Their ages ranged between 2 and 38 years. Mean age was 20years. Male: female ratio was 10:3. The left side was affected in 8 patients and the right side in 5 (Table 1). Presentation was mainly with loin pain. The 2 youngest patients aged 2 and 4 years were presented by the parents with an abdominal mass. A 14year-old patient with bilateral pelvic kidney presented with right lower abdominal pain corresponding to the hydronephrotic kidney. Another 14-year-old boy presented with left flank pain after injury at a football match. This turned out to be traumatic determinism for the PUJ obstruction. All the patients had an abdominal ultrasound examination and an IVU. A 4-year-old child had a micturating cystourethrogram (MCU) to check for vesicoureteric reflux, but this was absent. 3 patients had retrograde ureteric catheterization and ureterography as the ureter was not outlined on IVU. The ureters were normal. In 2 children aged 2 and 7 years, the affected kidney was not outlined on IVU but ultrasonography had shown hydronephrosis. Exploration was done; the younger patient had nephrectomy for a grossly hydronephrotic kidney and the other had Y-V plasty. Y-V plasty was done on 6 patients, dismembered pyeloplasty on 5 and nephrectomy on 2 (Table 2). Stenting of the repairs with a double-J-stent was done in 7 patients. The operations were done via extraperitoneal lumbar approaches except in the patient with pelvic kidneys where a peritoneal approach through a Pfannenstiel incision was made. Two patients who underwent renal exploration with a tentative diagnosis of PUJ obstruction turned out to have different pathology. A 7-year-old boy had a right renal cell carcinoma, and a 4-year-old boy had a variant of polycystic kidney on the left side. In both cases nephrectomy was done, and they were excluded from the study. One patient with dismembered pyeloplasty had a broken double 'J' stent. This device had long expired. The patient voided small fragments of the stent over a long period of time. Eventually 2 small fragments were left in the kidney on follow up IVU. The renal function and results of the affected side was good. He will require ureteroscopic removal of these fragments to prevent eventual calculi formation. The patient with pelvic kidneys has dismembered pyeloplasty for PUJ obstruction of the right kidney. He had prolonged urine leak of about 1 month. The repair was not stented. The results of the pyeloplasty were therefore good. Discussion PUJ obstruction in the patients studied occurred principally on the left, with male preponderance and a wide age range, concurring with findings in the literature1. Abnormalities of position or rotation were seen in 2 patients; one with bilaterally malrotated kidneys and the other with pelvic kidneys. No bilateral disease was found. This demonstrated the wide range of disease13 The retrograde ureterographic studies and MCU did not demonstrate any ureteric abnormality with which this may be associated14. The operations of pyeloplasty were open, as contrasted with laparoscopic, which has gained ground both in children and adults 8,9. Nevertheless the results were good, which compares well with the literature 2,6,7. The broken double –J- stent was long expired and this calls for caution in the use of articles with long expiry. It is advisable to test the tensile strength of such an appliance before use. Although a double 'J' stent reduces the duration of urine leakage, its use is a waning, in preference for non-stented pyeloplasties, with their attendant absence of stent related complications15. The 2 youngest patients are the ones who had nephrectomy demonstrating the varied nature of this entity13. The finding of a renal carcinoma and polycystic kidney demonstrate the need to always consider other possibilities despite clinical and radiological suggestions of PUJ obstruction. Conclusion The results of pyeloplasty are good in relieving the symptoms and preventing renal deterioration in selected patients. Complications are few if meticulous surgical technique and general care is applied. The possibility of other pathology as differential diagnosis should always be borne in mind. Acknowledgement. I sincerely thank Samora Maranya for the drawings, and Jason Mwawana for the computer work. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04031t2.jpg] [js04031f1.jpg] [js04031t1.jpg] [js04031f3.jpg] [js04031f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}