 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 28-31 Incidence and Patterns of Congenital Talipes Equinovarus (Clubfoot) Deformity At Queen Elizabeth Central Hospital, Banter, Malawi.1Mkandawire N.C. MCh (ORTH); FCS (ECSA), 2Kaunda E Cert. NMT. Lecturer in Orthopaedic and Trauma Surgery, College of Medicine, Blantyre, Malawi, 2Research
Nurse
in QECH and Beit Trust Cure International Hospital, Blantyre, Malawi. Code NUmber: js04033 Background:Clubfoot is one of the most common externally visible congenital deformities recorded in Sub Saharan Africa. The main objective of this study was to assess the overall incidence of clubfoot deformity in neonates born at Queen Elizabeth Central Hospital (QECH) in Malawi. Introduction Clubfoot is one of the most common visible congenital deformities seen in Sub Saharan Africa. This has been confirmed by a study done at Queen Elizabeth Central Hospital, which we have previously reported1. Having noted this fact it was felt necessary to try and assess the incidence and patterns of this deformity at QECH. There is a scarcity of data on the incidence of congenital anomalies in Sub Saharan Africa. Although this data was hospital based it will go a long was estimating the incidence and patterns of clubfoot deformity. Such information is vital in helping to quantify the magnitude of the problem and allows for resource planning in the management of this condition. The objectives of this study were:
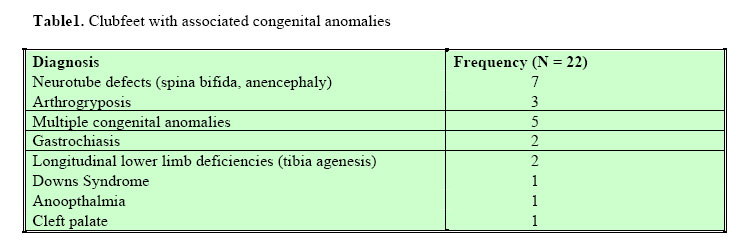
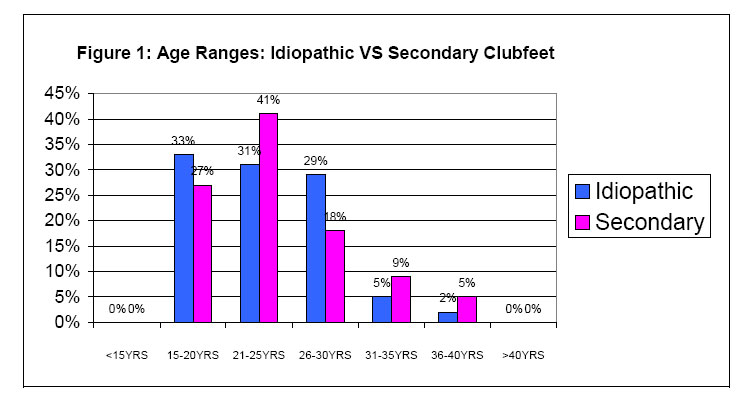
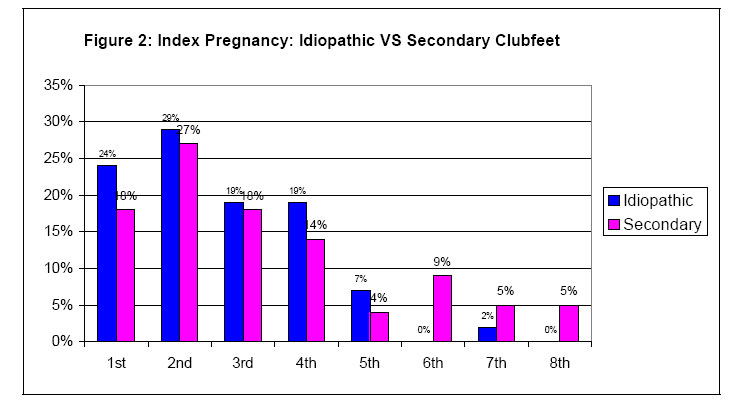
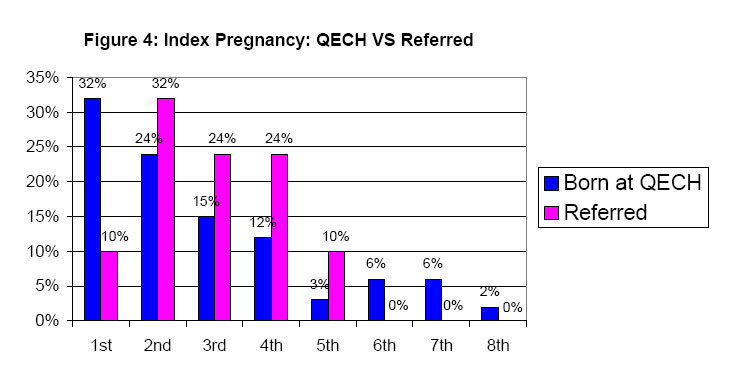
Patients and Methods This was part of an ongoing prospective study cataloguing all congenital anomalies presenting to the neonatal unit at Queen Elizabeth Central Hospital. All neonates with congenital anomalies born at or referred to QECH were enrolled in the study. A subset of neonates with a clubfoot deformity was selected for analysis. The study period was from 1st November 2000 to 11th September 2002. Results Incidence The number of children with clubfoot deformity recorded during the study period was 64; 34 of them being born at QECH and the remainder born elsewhere. The total number of all births at QECH during this period was 16877. This gave an estimated clubfoot incidence of 1 in 496 per number of births or 2 per 1000 births. Patterns of Clubfeet Thirty-six (56%) of children with clubfoot were male and 27 (42%) were female (M:F ratio =1.3:1). One child was a true hermaphrodite. 47 (73%) of the children had bilateral clubfeet. Among the 17 children with a unilateral clubfoot the right side was involved in 12 (71%) of the children. Forty-two children had apparent primary idiopathic clubfoot i.e. an otherwise normal child whose only deformity was the clubfoot. The remaining 22 children had clubfoot deformity associated with other congenital anomalies or a syndromal diagnosis. Table 1 shows the congenital anomalies that were found to be associated with congenital clubfoot deformity. Neurotube defects were the commonest anomalies associated with clubfeet. Obstetric Parameters Gestation period. Fifteen out of 64 children with clubfeet were preterm; eight had idiopathic clubfeet and seven had clubfeet associated with other congenital anomalies. 49 children with clubfeet were born at term. Multiple births Out of the 64 children with clubfeet only 4 were from multiple births. All 4 were involved in twin pregnancies and all 4 were the second twin. Birth weight Nine had Low Birth weight (LBW); 6 were Small for Gestation Age (SGA); 56 were Appropriate for Gestation Age(AGA) and 2 were Large for Gestation Age (AGA). Among the 9 who had Low Birth Weight, 8 were premature and only one was term. Seven were associated with idiopathic clubfeet and only 2 had other associated congenital anomalies. Among the 6 who were small for gestation age, 2 were premature and 4 were term. Four had primary idiopathic clubfeet and 2 had associated congenital anomalies. Mode of delivery Among the 64 cases with clubfeet, 54 were spontaneous vertex deliveries; 7 were breech presentations of which 5 had associated congenital anomalies and 2 were idiopathic clubfeet. Three were delivered by Caesarean section the indications of which were breech presentation in a primigravida, previous scars and cephalopelvic disproportion. Stillbirth and neonatal deaths There were 3 stillbirths. The causes were anencephaly, severe prematurity and gross multiple congenital anomalies. There were 2 neonatal deaths; one child had gross multiple congenital anomalies and the other had gastrochiasis. Maternal demographics Figure 1 shows the age ranges of mothers whose neonates had idiopathic clubfeet compared with those whose clubfeet are associated with other congenital anomalies. The peak age ranges between these groups are similar, with 2/3 of the births occurring within the age range 15 years to 25 years in both groups. Figure 2 shows the relationship between pregnancy order and frequencies of clubfeet; comparing mothers whose children had idiopathic clubfeet with those whose children had clubfeet associated with other anomalies. The two groups had similar patterns with most mothers having the child with a clubfoot in the first or second pregnancy. Figure 3 and Figure 4 show, respectively, age ranges and pregnancy order comparing mothers whose children were born at QECH and those born elsewhere. Maternal demographic characteristics and obstetric histories between those who delivered at QECH and those who were referred are shown to be similar. Discussion The incidence of clubfeet among children born at QECH is estimated at 2 per 1000 live births. Studies among black South Africans showed that the incidence of congenital clubfoot is between 1.5 per 1000 and 3.5 per 1000 live births2,3. Amongst Caucasian populations the incidence of congenital clubfoot is between 0.64 and 2.5 per 1000 live births4,5. Our study confirmed findings that boys are involved more frequently than girls; bilateral involvement is more common than unilateral involvement and the right side is more commonly involved than the left side. Children with clubfeet associated with other congenital anomalies accounted for 22 (34%) of all cases. The commonest congenital anomalies associated with clubfoot deformity involve the neurotube (spina bifida and anencephaly). The demographic characteristics and obstetric history of mothers were similar whether the children were born at QECH or elsewhere and whether the child had idiopathic clubfoot or had other congenital anomalies. We conclude that this hospital based clubfoot incidence study over nearly a two-year period should be continued and expanded to other hospitals and also to traditional birth attendant in order to establish the true incidence of clubfoot in Malawi. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04033f2.jpg] [js04033f4.jpg] [js04033t1.jpg] [js04033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}