 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 32-37 Vesico-vaginal Fistula Surgery in Uganda.Brian Hancock MD FRCS, Mhairi Collie MD FRCS University Hospital of South Manchester and Edinburgh Royal Infirmary.UK Correspondence to: Mr. B.D.Hancock. 21 Yealand Rd, Yealand Conyers, Lancashire. LA5 9SG, UK. Email: brian@yealand.demon.co.uk Code Number: js04034 Background:Childbirth injuries are common in Uganda. This paper describes our
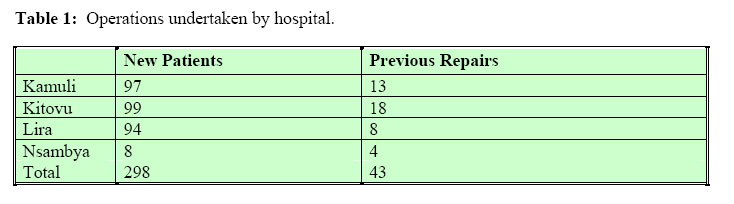
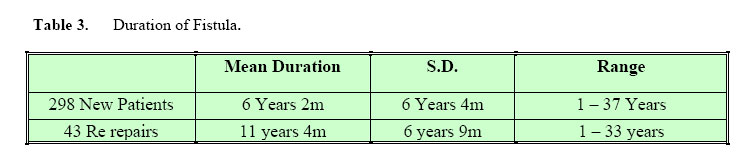
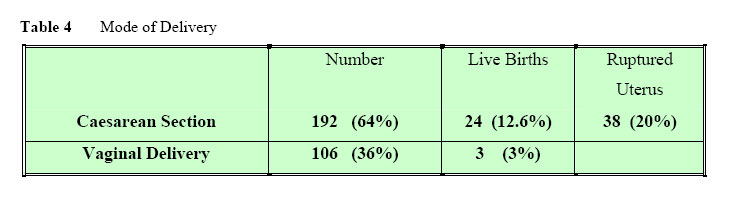
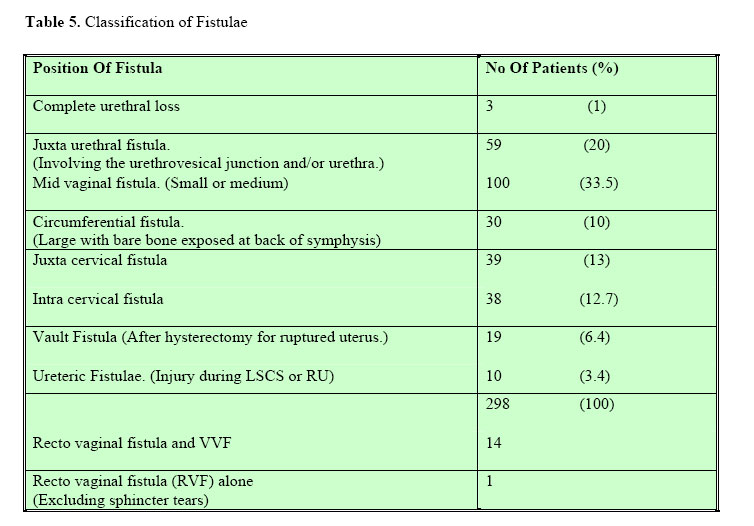
experience with Vesico-vaginal Fistula repair and aftercare. Introduction Vesico-vaginal fistula (VVF) is a devastating outcome from prolonged labour, which every day complicates a significant number of deliveries in the developing world. Studies in Nigeria have indicated an incidence of 1% of all deliveries; and in Ethiopia, 1000 cases are estimated to occur every year1 . The true figures are likely to be higher than this. Improved antenatal care and obstetric facilities have almost wiped out the condition in the developed world. In Ethiopia, the Addis Ababa Fistula Hospital for Poor Women with Childbirth Injuries founded by the Hamlins, is a major world centre for fistula work, with over 20,000 repairs undertaken to date the other being in Northern Nigeria run by Kees Waaldijk who has a personal experience of over 12,000 cases. Results published from the fistula hospital by Kees Waaldijk and from Ann Ward in southern Nigeria are encouraging, with over 90% healing achieved overall3,4,5 . In Uganda, there is no permanent centre undertaking regular fistula repair, although a surgeon of the flying doctor service (AMREF) visiting the north and east of the country undertakes over 150 repairs per year. It was with such a background that a program of surgical camps was set up, co-ordinated by a visiting English surgeon, with input from Ugandan, British and Ethiopian surgeons. This paper presents the results from 18 visits to 3 hospitals in rural Uganda, with treatment of 341 patients. Patients and Methods This was a cohort study, with prospective collation of data. Consecutive patients seen with vesicovaginal fistula between Feb 99 and July 2003 were included. The hospitals visited were Kitovu Mission hospital, Masaka in the west (four visits), Kamuli Mission hospital, Busoga in the east (seven visits) and Lira government hospital in the north (seven visits). Brief visits were also made to Nsambya Mission Hospital in Kampala. Patients were invited to come for treatment free of charge by radio broadcasts prior to the surgeons’ visit. On average 15 patients per week were treated. Most patients who answered the radio call were given a chance of operation during that camp. Where it was not possible to finish all the cases, patients were given a firm date for the next visit. Lira has experienced the biggest backlog of patients such that on one occasion the surgeon’s visit was not publicized.Patient Details A total of 341 patients underwent operation, of which 298 were new cases and 43 re-repairs. A total of 29 patients were seen but asked to return because of constraints of time. Five new patients were turned down for operation .One had a double fistula with other serious medical problems. Another had large fibroids filling the pelvis and three were considered inoperable on account of the extent of the injuries together with a small bladder. One had a urinary diversion by a Mainz 2 pouch. All the patients with a ruptured uterus had an emergency hysterectomy. The incidence of ureteric damage was at least 13% in this group. Parity. In 52% percent of the new patients the fistula followed the first pregnancy; 15% of fistula patients became pregnant again while they had a fistula. Type of Fistula (New Fistulae) and Operative Details Only 20% of the fistulae overall were small, mobile and accessible and classed as easy. Though the classification of Waaldijk5,6 has been recorded recently, our classification is given in simple descriptive terms according to the position of the fistula. In 252 (84%) of the 298 cases, repairs were undertaken transvaginally. The abdominal approach was used in 39 patients (13%), principally for the intra cervical fistulae that followed Caesarean section and for uretero-vaginal fistulae. A combined approach was employed in 7 cases (3%). Ureteric catheters were used to identify and protect at least one ureteric orifice in 82 of 298 new cases (27%). A Martius labial fat graft was used in 66 (22%) of the 298 new cases. At first it was used quite often but with more experience it was used less and less, only in 6 cases of the last 100 cases. Re-Repairs Forty-three patients had had previous attempts at repair, four of which were our failed cases. The others came from nine different hospitals in Uganda. Recto Vaginal Fistulae (RVF) Fourteen patients had a recto vaginal fistula in addition to the VVF (4%) and there was one isolated RVF. (The isolated high RVF probably resulted from accidental injury the upper rectum the time of an emergency hysterectomy for ruptured uterus. It was easily repaired transvaginally. In eleven both fistulae were repaired at the same time. In one, the vesical fistula was considered beyond repair and two others had the rectal fistula repaired alone deferring the vesical closure to a later time. Five patients with high rectal fistulae had a prior colostomy. Results for VVF Surgery Accurate figures were difficult to obtain. The resident doctors who cared for the patients after the surgeon had moved away were diligent in recording the outcome, but there was no uniformity of assessment. Some simply recorded the outcome as dry or wet at the time of discharge. Those that were wet may have had stress incontinence, which may have improved with time. Some had a dye test in theatre, which was the best way of assessing fistula closure. Urethral leakage can be assessed though this is dependant on the degree of bladder filling. Few patients were able to return for follow up, which is so necessary for final assessment of outcome. We saw patients return with a residual fistula who were said to be dry at the time of their discharge and conversely patients who were wet at discharge could come back dry. We asked any patient who was wet on discharge to return for assessment but unfortunately many failed to do so. Given those limitations we knew that we had failed to close the fistula in at least 15 (5%) of the 298 new patients and that another 9 (3%) had severe stress incontinence. We believe that because of inadequate follow up, the failure rate for closure and stress might have been significantly higher. The results for those having a second attempt at repair were not so good. Seven (16.7%) out of 42 had a definite breakdown and another two (5%) had severe incontinence. The true figure was probably higher. Results for RVF Out of the nine cases repaired without a colostomy, eight were reported to have been discharged without a leak. One had a major breakdown had a high fistula found unexpectedly while repairing the VVF. In retrospect the repair should have been deferred until a colostomy had been performed. Of the five patients with a colostomy only one had been closed for certain; the outcome of the remainder is not known. Discussion This survey has show that there is great-unmet need for fistula repairs in Uganda. In the absence at any dedicated fistula hospital or unit set aside for VVF patients in Uganda we have shown that it is possible to get acceptable results by operating fistula camps in hospitals which have no previous experience. Nsambya and Kitovu have regularly performed fistula repairs in the past but Lira and Kamuli have not. We have experienced a long learning curve in becoming reasonably proficient in fistula surgery and believe that apprenticeship to an experienced surgeon is the only way to make progress. We estimate that only 20% of our cases could be classified as easy such that a surgeon with basic skills and interest could repair unaided. It is noteworthy that only 4% of this consecutive series had a coexistent recto-vaginal fistula while in Ethiopia and in Northern Nigeria the corresponding figures were 17% and 10% respectively. There is no clear explanation for this but it is probable that patients seen in the Addis Ababa Fistula Hospital present with more difficult fistulae than the Uganda patients. The high rate of Caesarean section (64%) was noted. Most were done when the baby was already dead. This indicates that many patients can get to hospital when in obstructed labour but arrive when it is too late to save the baby. Most post-Caesarean section fistulas are in the region of the cervix and the conduct of the operations may have had some influence on the development of the fistulas. When the head of a dead baby is deeply impacted in the pelvis craniotomy is a possible way of avoiding a Caesar but if done it is better to push the head up from below than forcing a hand down from above which may further damage devitalized tissues. Very few patients with a vaginal delivery reported having had a live baby, as the trauma of a prolonged labour sufficient to cause a fistula is rarely compatible with foetal survival. Conversely 12.6% of those having a Caesarean section delivered a live baby. This almost always indicates that the fistula will be between the lower segment and bladder as a result of accidentally incorporation the bladder in the lower segment closure. Ureteric fistulae result from operative difficulties especially when a hysterectomy is performed for ruptured uterus. It is of note that none of the patients who had a ruptured uterus had this repaired yet this has been shown not only to be possible but safe. We do not routinely wait for three months from time of injury provided the area is clean and healthy7. We only give antibiotics (Gentamycin one dose 120 mg IV) to cover the peri-operative period. Initially, most fistulae were closed in two layers but increasingly a single layer of well-placed sutures was used without any detrimental effect. This involved less mobilization with a saving on time and sutures. Fat grafts were at first routinely used for defects involving the urethro-vesical junction (about 60% of cases) but in the last two years the use of fat grafts was almost abandoned without any reduction in success. There was a beneficial reduction in the amount of dissection, operating time and suture usage. Regarding equipment it is necessary to have a tilting table, as the majority need a steep head down position. The surgeons bring their own sharp dissecting scissors and selection of eyed needles and sutures. A slowly absorbed suture is preferred but chromic catgut alone appears to work as well. Ureteric catheters were necessary in 20% of cases where the ureteric orifices were at risk. After care is vitally important. Nothing must pull on or block the catheter. Nursing skills will always be in short supply and there may be frequent changes of staff. It is essential to make the postoperative care as simple as possible. At first the methods used at the Addis Fistula hospital consisting of two weeks bed rest and open catheter drainage into a kidney dish placed between the patient’s legs were followed. These methods were soon found to be impracticable and were modified. The open kidney dish drainage did not work because it was frequently knocked over or disappeared under the patient in a saggy bed. Closed drainage was tried briefly. It had the advantage that the patients could get up out of bed early but several drawbacks were found. The tubing was often of poor quality and frequently became kinked. The bags became overfull especially in the night. Methods to secure the bag or tubing to the bed lead to pulling on the catheter when the patient moved. The problem was solved by adopting free drainage of an open-ended plastic tubing (IV tubing works) attached to the catheter and draining into a bucket or basin beside the bed. The catheter is secured to the top of the labia with a stitch and no strapping is used. Following the experience of Kees Waaldijk and Tom Raassen we have recently allowed our patients out of bed from the second post-operative day. They carry their buckets with them until the catheter is removed on the 10th day for the simplest cases to the 14th for the rest. A high fluid intake starting before the operation is continued through the postoperative period. There is no need to measure urine output; it is sufficient to observe the colour. If not like water the patient is not drinking enough. Training is an essential part of our work. Many Ugandan surgeons have been assisted at these operations and we wish to encourage them to repair the simple ones themselves. Acknowledgement The senior author is most grateful for instruction received from all the staff at the Addis Ababa Fistula Hospital and from a visit to the unit of Kees Waaldijk in Northern Nigeria. Dr Maura Lynch at Kitovu and Dr Tom Raassen have give very helpful advice for which we are indebted. We are most grateful for all the Uganda medical and nursing staff that have assisted at most of the operations and cared for the patients in our absence. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04034t6.jpg] [js04034t4.jpg] [js04034t7.jpg] [js04034t2.jpg] [js04034t1.jpg] [js04034t5.jpg] [js04034t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}