 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 41-44 Results of Triple Arthrodesis in Uganda.Bitariho D. M.Med (Ortho.) FCS (ECSA), Norgrove P. M.D., FRCS (C ) Childrens’ Orthopaedic Rehabilitation Unit, Mengo Hospital, P O Box 7161, Kampala, Uganda Code Number: js04036 Background: In Uganda, foot deformities of various kinds and complexities are
common. The aim of this study was to evaluate and determine whether triple
arthrodesis is an effective and reasonable operation in the African perspective. Introduction Triple arthrodesis, first described by Hoke and later by Dunn is regarded as a good salvage procedure to correct deformities and relieve pain of the foot 1,2, 5,6 . Many surgeons believe that triple arthrodesis in children should be deferred until the age of 12 years, for fear of increased failure of fusion, recurrence of deformity or excessive shortening of the foot3 . Others however, feel that triple arthrodesis can be performed at a much earlier age3, 4 . Whereas in the past many reviews with excellent results were reported, more recent reviews have given depressing figures of good results in as low as 25% only6,7 . The aim of the present study was to evaluate the outcome of triple arthrodesis among patients treated for foot deformities in Uganda with a view of assessing the effectiveness of the procedure in the African environment. The residual deformities, functional results and outcome of surgery among patients aged less than 10 years and those 10 years and above were compared. This paper presents the findings. Patients and Method During the years 1996 to 2000, a total of 143 children and youths aged between 6 and 21 years underwent Triple Athrodesis procedure. However, only 36 patients, on whom 42 triple arthrodesis operations were done, returned for follow-up examinations and comprised the study population. The operations were performed for foot deformities that resulted mainly from congenital clubfoot and poliomyelitis. Other causes included cerebral palsy, post injection sciatic nerve injuries, arthrogryposis, congenital equinus, Larsen’s syndrome and trauma. Information regarding the age at operation, length of follow-up, the patients’ main complaints, pre-operative deformity and type of triple arthrodesis done was recorded. Patients were questioned about pain, swelling, instability, post-operative complications and the success of the operation. Physical examination details of the hind and mid-foot morphology, global alignment of the foot and functional evaluation were recorded. Radiographs were used to assess fusion of the joints. The results of surgery were graded using the Mackenzie grading system as adopted from Hallglimson (1943) as follows:
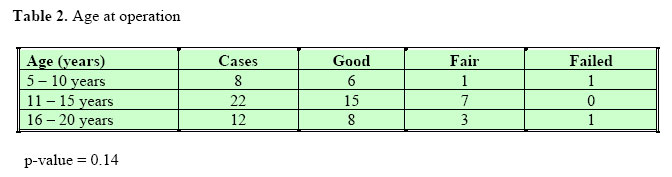
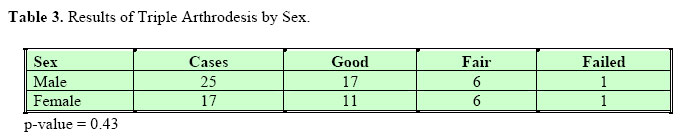
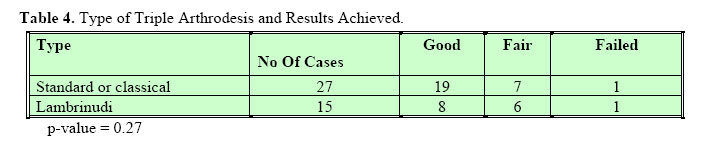
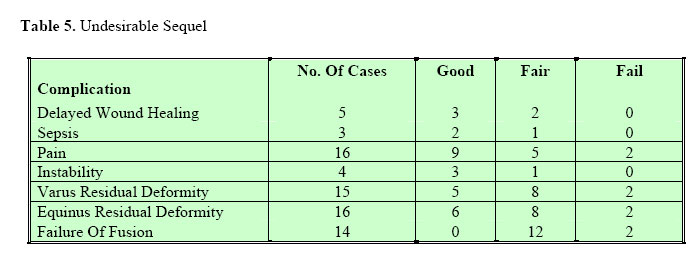
Results During the years 1996 to 2000, triple arthrodesis was performed in 143 children aged between 6 and 21 years. Of these only 36 patients with 42 triple arthrodesis operation were available for follow up and formed the basis of this study. The patients’ ages ranged between 6 and 21 years with a mean of 12.75 years. The commonest causes of foot deformity were poliomyelitis and congenital clubfoot. Table 1 shows the triple arthrodesis grading in the 42 feet. Table 2 compares the results of surgery in different age groups at operation. There was no statistically no difference in outcome of triple arthrodesis in the three age groups (p Value = 0.14). There was no sex difference in the outcome of triple arthrodesis (Table 3). There was no significant difference between standard or classical arthrodesis and Lumbrinudi (Table 4). (Table 5) Discussion As we analysed the results, we had a number of factors to consider. Among them was the fact that we usually deal with neglected, severe and long standing deformities. None of the deformities in this study had had previous surgery and very few had inadequate conservation manipulations. It is a belief among most local communities that having a deformity is a curse from God or bad spirits and thus no medical intervention should be made. This has been enhanced by lack of formal education and rampant poverty among the rural population. Thus unless a charity organization, such as Christian Blind Mission (CBM), comes in to help facilitate the poor health system, most of these patients are also not attended to by most of health facilities. We recognized the fact that triple arthrodesis is not a perfect procedure, but is the best option in the circumstances of low resources. The aim of the operation was to get a plantigrade and shoeable foot. It was found out that despite some residual deformities, patients appreciated most of the results obtained. This was due to the fact that the post-operated foot looked much better than the pre-operative deformed foot. The children with deformities avoided going to schools because they were despised and ridiculed by their fellow children and even adults, which affected their socio-psychological life. The results obtained in our series may not be comparable to those from the developed world, mostly because of our patients presented late with neglected deformities. There was no ideal result of all the forty-two feet that were reviewed. There was a close correlation between subjective and objective results. One patient graded the result as unqualified success in spite of residual deformities, pseudarthrosis and pain on activity. This is an instructive discrepancy and emphasizes the over-riding importance of function. There was no statistically significant difference (p-Value = 0.14) in results obtained among those patients aged below and those aged above 10 years. This confirmed what had been reported in other studies satisfactory results can be achieved in-patient aged less than twelve years and as has been found out by other surgeons3,4. Our study confirmed what had been reported by other authors that no sex difference in functional outcome exists8. The causes of the deformities in our cases were poliomyelitis and congenital clubfoot in 44% and 36% respectively. The results of surgery were better in poliomyelitis than in clubfoot. Similar findings have been reported in other studies4,8. In our review, the type of triple arthrodesis did not affect the functional out come, although earlier work by Manson et al8 showed that Lambrinudi procedure appeared to give better results than the standard. Undesirable effects of surgery included pain either after normal daily activity or after heavy use in 38% and residual deformities, especially of varus and equinus, in 62% of cases. All the failed cases reported presence of pain. Another common complication was. The varus deformity did not exceed 5° (mild <10°) while equinus was moderate (<10°) in the majority of cases. These also contributed to the majority of fair and failed results. The actual causes of these deformities could not be established from the study but the possible causes could be:
Pseudoarthrosis was observed in 33% of cases where the talo-nanicular joint was involved in all the cases and calcaneocuboid in 2 cases but none for the subtalar joint. Our rates were worse than that reported in literature which ranged from 0% to 23%4. Lack of internal fixation, poor bony apposition and early weight bearing were identified in literature as causes of pseudoathrosis6, and these could not be ruled out in our study. Acknowledgement We thank Maria Regina, Miriam and OURS Management for their untiring efforts in tracing the patients. We are indebted to the management of the Children.s Orthopaedic Unit at Mengo Hospital for the financial support. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04036t5.jpg] [js04036t1.jpg] [js04036t4.jpg] [js04036t3.jpg] [js04036t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}