 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
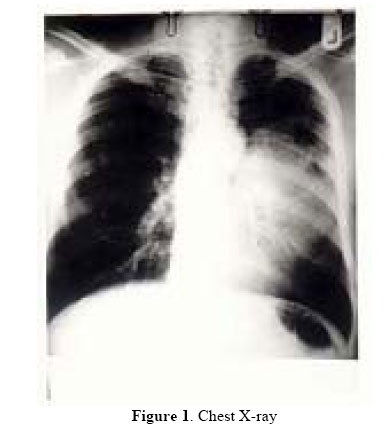
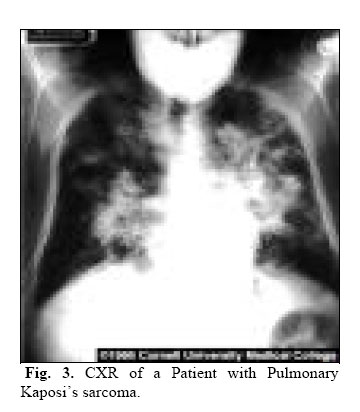
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 49-53 Kaposi’s Sarcoma Of The Lung: A Case Report. Ussiri EV, Lema LEK, Mbembati NAA, Mchembe MDPM Dept. Of Surgery, Muhimbili National Hospital. Code Number: js04038 Pulmonary Kaposi’s sarcoma is a rare condition. Its diagnosis may be tricky due to its similarities in clinical and radiological features with pulmonary opportunistic infections as well as other lung lesions. Treatment for Kaposi’s sarcoma include radiotherapy, chemotherapy and/or immunotherapy whereby lung Kaposi’s sarcoma respond well to chemotherapy. An immunocompetent 68-year-old man was admitted with clinical, radiological and bronchoscopic features of bronchogenic carcinoma. However, the histological result revealed Kaposi’s sarcoma of the lung. The patient was treated with radiotherapy and recovered well from his symptoms. Six months later the patient remain asymptomatic with essentially a normal chest x-ray. Introduction Kaposi’s sarcoma was first described by Moritz Kaposi in 1872 as a multifocal angioproliferative lesions (1,2). However, Goedert et al in 2002 described Kaposi’s sarcoma as a malignancy of lymphatic endothelial cells (3). In 1980s the prevalence of Kaposi’s sarcoma began to increase dramatically and became the most common malignancy in patients with Immunodeficiency disease (1,4). Hong and Lee in 2002 found that extracutenous or visceral Kaposi’s sarcoma lesions were more common in HIV infected patients rather than HIV-negative patients(2). Sung et al (4) in 1997 classified Kaposi’s sarcoma into four types: classic, African (endemic), iatrogenic or drug associated and Acquired Immunodeficiency Syndrome (AIDS)related Kaposi’s sarcoma. Classic Kaposi’s sarcoma usually follows an indolent disease of probably low malignant potential. In contrast, AIDS-Kaposi’s sarcoma is a fulminant disease that requires aggressive pharmacotherapy with poor prognosis especially when it involves visceral organs. Case Report S.M a male patient aged 68 who was referred from Ifakara, Morogoro region and admitted to surgical ward on 9th January 2003 with four months history of gradual onset of productive cough and haemoptysis. Sputum was purulent, not copious or foul smelling. The Cough was not related to posture but accompanied by episodes of haemoptysis, and localized dull ache on the lateral aspect of the left side of the chest. He had no fever, night sweats, and anorexia or weight loss. He did not respond to antibiotic therapy. He was married with eight children, all alive and well. He smoked three packets of cigarettes per day for about 40 years. He was a retired long distance truck driver. Physical examination revealed an elderly man of good nutritional status. He was not dyspnoeic, neither pale, nor febrile. He had no finger or toe clubbing. The cervical, axillary, or inguinal lymph nodes were not palpable. Pulse rate was 80/minute, Blood pressure was 120/70. The respiratory rate was 18/minute, trachea was central and the chest was symmetrical in shape. There was a reduced chest expansion on the left hemithorax and dull percussion note over the left hemithorax with signs of consolidation. The right hemithorax was clinically normal. Other systems were examined and found to be normal. The provisional diagnosis of Bronchogenic Carcinoma was entertained. Investigations done included a chest X-ray that revealed left perihillar opacity with ill-defined margin (Fig.1). Haemoglobin was 12.0 g/dl, WBC: Normal count and distribution, ESR was 80mm/hour Westergren method. Sputum for Acid Fast Bacilli (AFB) was negative, three times. Mid-morning sputum for cytology revealed no evidence of malignant cells ECG was within normal limits and abdominal ultrasound was normal. CT scan of the chest and upper abdomen revealed a soft tissue mass in the left upper lobe of the lung adherent to pleura with a small pleural effusion. No enlarged lymph nodes or bone involvement. No liver metastasis. Features were suggestive of a left lung tumour (Fig.2). Bronchoscopy was done and revealed a blunt carina, narrowed left main bronchus, with a tumour involving the left main bronchus close to its bifurcation into upper and lower lobe bronchi. Biopsies were taken for histological studies and results revealed features of Kaposi’s sarcoma. A review of the histology was requested and the tissue diagnosis confirmed the same. Double ELISA tests for HIV infection were negative. The Hospital Tumour board recommended palliative local (chest) radiotherapy to the patient. He was transferred to Ocean Road Cancer Institute on 13th February 2003 where he received five courses of 30Gy (300 rads) each over a period of five days with dramatic improvement on the symptoms. He was discharged home and reviewed on follow-up at the outpatient clinic three and six months later, and found to remain symptoms free with an essentially normal chest x-ray. Discussion Patients with primary classic Kaposi’s sarcoma appear to be at a higher risk of multiple malignancies5. Study by Iscovich et al5 in 1999 when evaluating the risk of second neoplasms in 1,016 HIV-negative patients with primary classic Kaposi’s sarcoma between 1961 to 1992 in Jewish population found that 61 (6.0 %) patients developed second neoplasms. The commonest neoplasms were Non Hodgkin Lymphoma and cutenous malignant melanoma In the same study it was found that 8.4% of patients with primary malignancies developed a secondary classic Kaposi’s sarcoma. The commonest primary malignancies being Non Hodgkin Lymphoma, Hodgkin Lymphoma, leukaemia and breast cancer (odds ratio were 5.3, 7.5, 5.3 and 2.2 respectively).The case presented had no other malignancy found or any lesion elsewhere in his body suggestive of Kaposi’s sarcoma. Kaposi’s sarcoma of the lung of patients with HIV infection is often indistinguishable by clinical and radiologic criteria from opportunistic pneumonia though both may be present in the same patient6. The commonest clinical symptoms of Kaposi’s sarcoma of the lung includes dyspnoea, cough, occasionally haemoptysis and stridor7,8,9. Most frequent opportunistic chest infection seen in patients with AIDS are tuberculosis, bacterial pneumonia and pneumocystis carinii pneumonia (pcp), which clinically present with acute onset of fever, non-productive cough and dyspnoea10. The presented patient had no fever and was not dyspnoeic. Fibreoptic bronchoscopy and broncho-alveolar lavage and/or biopsy remain the standard investigation to differentiate between opportunistic pneumonia and pulmonary Kaposi’s sarcoma6,9. Hanson et al6 in 1987 performed 13 fibreoptic bronchoscopies in patients with thoracic manifestation of AIDS and identified Kaposi’s sarcoma in four (30%) bronchoscopic specimens. This yield was comparable to that obtained only by open lung biopsy procedures in previous reports. However, Daley et al11 in 1996 when evaluating the role of bronchoscopy and broncho-alveolar lavage in HIV positive patients with pulmonary manifestations found that the commonest opportunistic pulmonary infection was pulmonary tuberculosis (75 %), bacterial pneumonia (14 %), pcp (one patient) and Kaposi’s sarcoma (two patients-1%). It was concluded that bronchoscopy with bronchoalveolar lavage added little to the diagnosis and should not be used for routine work-up in developing countries where tuberculosis is endemic. Similar study was done in Rwanda and revealed non-specific pneumonitis (38%), pulmonary tuberculosis (23%), cryptococcosis (13%), Kaposi’s sarcoma (9%), pcp (5%), undetermined cause (16%)12. Typically radiographic features of pulmonary Kaposi’s sarcoma (Fig.3) include bilateral involvement, ill-defined patchy opacities, hilar lymph node enlargement and pleural effusion1. Radiological features of pcp include bilateral patchy opacities with or without a cyst (Fig.4). The case presented had an ill-defined left perihilar opacity on CXR which on CT scan examination (Figures 1 and 2) showed a left lung tumour involving pleura with small effusion on the same side. Ventilating rigid bronchoscopy revealed a tumour involving left main bronchus, left upper and left lower lobe bronchi. Biopsy was taken and histology results were confirmatory of Kaposi’s sarcoma. This was the second case of pulmonary Kaposi’s sarcoma in HIV-negative patients seen in Thoracic Surgical Unit over a 20-year period. Literature search found a report of only one case of pulmonary Kaposi’s sarcoma in an immunocompetent 32 years old heterosexual male. This patient was treated with vincristine and died of brain metastasis13. Kaposi’s sarcoma is common in HIV-infected patients and rare in HIV-negative or immunocompetent individuals. Pulmonary Kaposi’s sarcoma is rare in both HIV infected as well as immunocompetent persons. This is the main reason, which makes this case worth reporting. Systemic chemotherapy is said to be the most effective treatment for pulmonary Kaposi’s sarcoma although its efficacy may be limited by neutropenia14,15. The commonest chemotherapeutic agents used include Adriamycin, Bleomycin, Vincristine, Liposomal Daunorubicin and Doxorubicin and Paclitaxel (Taxol)14,15,16,17. Combination chemotherapy has been found to have a dramatic clinical and functional improvement than a single agent. It has been found that patients with AIDSassociated pulmonary Kaposi’s sarcoma on chemotherapy and Highly Active Antiretroviral Therapy (HAART) increased survival18. Our patient was treated with local radiotherapy to the chest using 5 courses of 30 Gy, as he could not afford chemotherapy. Had a good response such that there was no more chest pain or haemoptysis. He was discharged home and seen at follow-up at three and six months outpatient clinic once a months. References:
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04038f3.jpg] [js04038f4.jpg] [js04038f2.jpg] [js04038f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}